Sustainability of the Niger State CDTI Project, Nigeria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Osprey Group Profile
Osprey Group Profile The preferred and trusted partner for international companies seeking to grow their business in West Africa Africa Europe North Africa West Africa East Africa South Africa Head Quarter Africa Head Quarters Europe Osprey House 47 Mississippi Wraysbury Hall Street, Ferry Lane Maitama District, TW196HG Staines, Middlesex Abuja FCT. Nigeria. London, UK. Introduction to Osprey Welcome to Osprey Investments Group, where our mission is to help drive development in West Africa by facilitating inward investment supported by world- class consultancy services delivered by competent technical partners. We achieve this by: • Connecting potential investors to opportunities in Africa and specifically marketing investment opportunities to multi-national firms in Asia, Europe and the US, • Facilitating fair and durable projects between Government and big multinational firms, • Promoting technology and skills transfer to local firms to improve efficiency, raise productivity and boost skilled employment, • Helping multi-national firms understand the risk/return trade-off of investing in Africa, and • Providing our clients with world-class technical resources. We are passionate about West Africa and firmly believe it will become one of the top 20 economies by 2020. With more than 44 years experience of working in Nigeria and a dedicated team of staff based in the capital Abuja, we can help your business gain a strategic foothold in the West African market place. Introduction to ECOWAS Population: 300 million Size: 923,768 sq. km Growth rate: 8.4% (ranked 15th in world) GDP (PPP): $378 billion (ranked 32nd in world) GDP per capita: $2500 GNI: $176 billion Labour force: 50 million Inflation rate: 13.7% Market value of publicly traded shares: $51 billion Largest ethnic groups: Hausa, Igbo, Yoruba Ref: CIA World fact book Why West Africa? West Africa, with an area of over 2.5 million square miles and estimated population of 325.5 million is Size of market comparable in size and people to the continental USA. -

A LETTER from KI-TORO MAHAMMAN GAANI, KING of BUSA (BORGU, NORTHERN NIGERIA) ABOUT the 'KISRA' STORIES of ORIGIN (C. 1910)
A LETTER FROM KI-TORO MAHAMMAN GAANI, KING OF BUSA (BORGU, NORTHERN NIGERIA) ABOUT THE ‘KISRA’ STORIES OF ORIGIN (c. 1910). P.F. DE MORAES FARIAS The context of the documents presented in this paper is firstly the history of Busa (‘Bussa’ in maps and administrative language), and Busa’s place within the general history of Borgu; secondly the traditions of origin of Borgu ruling lineages; and thirdly the West African travels of the French explorer G.R. de Gironcourt (1908- 1909 and 1911-1912). We will briefly examine these three areas in succession, before turning our attention to the documents themselves. Busa in Borgu: Factors for unity and factors for cleavage Busa is best remembered in Europe as the place where Mungo Park met his death in March or April 1806. But in its own right Busa is a major historical area within the region traditionally known as Borgu. The location of Busa’s capital has changed over time, and it is now at New Busa following the construction of the Kainji dam across the Niger.1 Borgu has a significant degree of historical cohesion, which was brought about by three overlapping factors dating from the precolonial period. The first factor was the body of traditions about fanning-out migrations, and dynastic origins, which still links Borgu’s old polities together. According to these traditions, initially members of the same lineage founded a few kindred states, but new fissions took place in these states: segments of the 1 See K. Lupton, ‘The Death of Mungo Park at Bussa’, Nigeria Magazine, 72, 1962, 58-70; M. -
The World Bank Implementation Status & Results
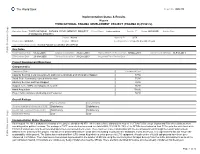
The World Bank Report No: ISR4370 Implementation Status & Results Nigeria THIRD NATIONAL FADAMA DEVELOPMENT PROJECT (FADAMA III) (P096572) Operation Name: THIRD NATIONAL FADAMA DEVELOPMENT PROJECT Project Stage: Implementation Seq.No: 7 Status: ARCHIVED Archive Date: (FADAMA III) (P096572) Country: Nigeria Approval FY: 2009 Product Line:IBRD/IDA Region: AFRICA Lending Instrument: Specific Investment Loan Implementing Agency(ies): National Fadama Coordination Office(NFCO) Key Dates Public Disclosure Copy Board Approval Date 01-Jul-2008 Original Closing Date 31-Dec-2013 Planned Mid Term Review Date 07-Nov-2011 Last Archived ISR Date 11-Feb-2011 Effectiveness Date 23-Mar-2009 Revised Closing Date 31-Dec-2013 Actual Mid Term Review Date Project Development Objectives Component(s) Component Name Component Cost Capacity Building, Local Government, and Communications and Information Support 87.50 Small-Scale Community-owned Infrastructure 75.00 Advisory Services and Input Support 39.50 Support to the ADPs and Adaptive Research 36.50 Asset Acquisition 150.00 Project Administration, Monitoring and Evaluation 58.80 Overall Ratings Previous Rating Current Rating Progress towards achievement of PDO Satisfactory Satisfactory Overall Implementation Progress (IP) Satisfactory Satisfactory Overall Risk Rating Low Low Implementation Status Overview As at August 19, 2011, disbursement status of the project stands at 46.87%. All the states have disbursed to most of the FCAs/FUGs except Jigawa and Edo where disbursement was delayed for political reasons. The savings in FUEF accounts has increased to a total ofN66,133,814.76. 75% of the SFCOs have federated their FCAs up to the state level while FCAs in 8 states have only been federated up to the Local Government levels. -

Violence in Nigeria's North West
Violence in Nigeria’s North West: Rolling Back the Mayhem Africa Report N°288 | 18 May 2020 Headquarters International Crisis Group Avenue Louise 235 • 1050 Brussels, Belgium Tel: +32 2 502 90 38 • Fax: +32 2 502 50 38 [email protected] Preventing War. Shaping Peace. Table of Contents Executive Summary ................................................................................................................... i I. Introduction ..................................................................................................................... 1 II. Community Conflicts, Criminal Gangs and Jihadists ...................................................... 5 A. Farmers and Vigilantes versus Herders and Bandits ................................................ 6 B. Criminal Violence ...................................................................................................... 9 C. Jihadist Violence ........................................................................................................ 11 III. Effects of Violence ............................................................................................................ 15 A. Humanitarian and Social Impact .............................................................................. 15 B. Economic Impact ....................................................................................................... 16 C. Impact on Overall National Security ......................................................................... 17 IV. ISWAP, the North West and -

Boko Haram Beyond the Headlines: Analyses of Africa’S Enduring Insurgency
Boko Haram Beyond the Headlines: Analyses of Africa’s Enduring Insurgency Editor: Jacob Zenn Boko Haram Beyond the Headlines: Analyses of Africa’s Enduring Insurgency Jacob Zenn (Editor) Abdulbasit Kassim Elizabeth Pearson Atta Barkindo Idayat Hassan Zacharias Pieri Omar Mahmoud Combating Terrorism Center at West Point United States Military Academy www.ctc.usma.edu The views expressed in this report are the authors’ and do not necessarily reflect those of the Combating Terrorism Center, United States Military Academy, Department of Defense, or U.S. Government. May 2018 Cover Photo: A group of Boko Haram fighters line up in this still taken from a propaganda video dated March 31, 2016. COMBATING TERRORISM CENTER ACKNOWLEDGMENTS Director The editor thanks colleagues at the Combating Terrorism Center at West Point (CTC), all of whom supported this endeavor by proposing the idea to carry out a LTC Bryan Price, Ph.D. report on Boko Haram and working with the editor and contributors to see the Deputy Director project to its rightful end. In this regard, I thank especially Brian Dodwell, Dan- iel Milton, Jason Warner, Kristina Hummel, and Larisa Baste, who all directly Brian Dodwell collaborated on the report. I also thank the two peer reviewers, Brandon Kend- hammer and Matthew Page, for their input and valuable feedback without which Research Director we could not have completed this project up to such a high standard. There were Dr. Daniel Milton numerous other leaders and experts at the CTC who assisted with this project behind-the-scenes, and I thank them, too. Distinguished Chair Most importantly, we would like to dedicate this volume to all those whose lives LTG (Ret) Dell Dailey have been afected by conflict and to those who have devoted their lives to seeking Class of 1987 Senior Fellow peace and justice. -

Socio-Economic Survey, 2014
NIGER STATE BUREAU OF STATISTICS (WITH TECHNICAL SUPPORT OF THE NATIONAL BUREAU OF STATISTICS) SOCIO-ECONOMIC SURVEY, 2014 Niger State Bureau of Statistics (NSBS) www.nigerstats.ni.gov.ng E-mail: [email protected] SOCIO-ECONOMIC SURVEY, 2014 NIGER STATE BUREAU OF STATISTICS ii SOCIO-ECONOMIC SURVEY, 2014 Table of Contents VISION AND MISSION STATEMENTS OF NIGER STATE BUREAU OF 1.16 Data Processing and Analysis ........................................ 4 STATISTICS (NSBS) ...............................................................................viii 1.17 Tabulation Plan ...............................................................4 Vision .......................................................................................................viii 1.18 Report Writing .................................................................4 Mission ....................................................................................................viii FOREWORD ............................................................................................. ix CHAPTER TWO .........................................................................................5 ACKNOWLEDGEMENT ............................................................................ x HOUSEHOLD CHARACTERISTICS ..........................................................5 BRIEF NOTE ON NIGER STATE .............................................................. xi 2.1 Average Household Size ................................................5 CHAPTER ONE .........................................................................................1 -

LGA Agale Agwara Bida Borgu Bosso Chanchaga Edati Gbako Gurara
LGA Agale Agwara Bida Borgu Bosso Chanchaga Edati Gbako Gurara Katcha Kontagora Lapai Lavun Magama Mariga Mashegu Mokwa Munya Paikoro Rafi Rijau Shiroro Suleja Tafa Wushishi PVC PICKUP ADDRESS Santali Road, After Lga Secretariat, Agaie Opposite Police Station, Along Agwara-Borgu Road, Agwara Lga Umaru Magajib Ward, Yahayas, Dangana Way, Bida Lga Borgu Lga New Bussa, Niger Along Leg Road, Opp. Baband Abo Primary/Junior Secondary Schoo, Near Divisional Police Station, Maikunkele, Bosso Lga Along Niger State Houseso Assembly Quarters, Western Byepass, Minna Opposite Local Govt. Secretariat Road Edati Lga, Edati Along Bida-Zungeru Road, Gbako Lga, Lemu Gwadene Primary School, Gawu Babangida Gangiarea, Along Loga Secretariat, Katcha Katcha Lga Near Hamdala Motors, Along Kontagora-Yauri Road, Kontagoa Along Minna Road, Beside Pension Office, Lapai Opposite Plice Station, Along Bida-Mokwa Road, Lavun Off Lga Secretariat Road, Magama Lga, Nasko Unguwan Sarki, Opposite Central Mosque Bangi Adogu, Near Adogu Primary School, Mashegu Off Agric Road, Mokwa Lga Munya Lga, Sabon Bari Sarkin Pawa Along Old Abuja Road, Adjacent Uk Bello Primary School, Paikoro Behind Police Barracks, Along Lagos-Kaduna Road, Rafi Lga, Kagara Dirin-Daji/Tungan Magajiya Road, Junction, Rijau Anguwan Chika- Kuta, Near Lag Secretariat, Gussoroo Road, Kuta Along Suleja Minna Road, Opp. Suleman Barau Technical Collage, Kwamba Beside The Div. Off. Station, Along Kaduna-Abuja Express Road, Sabo-Wuse, Tafa Lga Women Centre, Behind Magistration Court, Along Lemu-Gida Road, Wushishi. Along Leg Road, Opp. Baband Abo Primary/Junior Secondary Schoo, Near Divisional Police Station, Maikunkele, Bosso Lga. -

Evaluation of the Effect of Flooding on Danchitagi Community of Lavun Local Government Area, Niger State, Nigeria
Hummingbird Publications © December, HP Journal of Env. Design & Constructions Mgt. 2019 www.hummingpubng.com Vol. 19 No. 4 JECM 2019 Evaluation of the Effect of Flooding on Danchitagi Community of Lavun Local Government Area, Niger State, Nigeria M. A. Emigilati 1 Abdulkadir Nasiru 2 Department of Geography, Federal University of Technology, Minna – Niger State, Nigeria. Keyword: Abstract Niger State and precisely Danchitagi community in Danchitagi Lavun Local Government Area will continue to labour community, under the pains of flood disaster unless there is a Flooding, radical approach to avert the disaster. The aim of this farmland and study was to evaluate the effects of flooding on Lavun Danchitagi community in Lavun Local Government Area of Niger State, Nigeria. The researcher randomly distributed 355 household questionnaires while the instrument of in-depth interviews schedule was administered to the respondents. Frequency percentage statistics was utilized for data analysis and presentation. The finding shows that 193 (54.4%) of the respondents believed that the main cause of flood in the study area is from heavy rainfall, 148 (41.7%) of the respondents agreed that the main cause of flooding is due to flood plain development, poor drainage system ranked third with 13 (3.7%) of the respondents and blockage in the drainage ranked the least with one respondent. The results also shows that about 341 (96.1%) of the respondents said that their farmlands were being affected by flood while 14 (3.9%) said their farmlands were not being affected by flood since their farmlands were located far away from flood plain. Loss Page 103 of 322 JECM Vol. -

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

The Politics of Neglect in the Resettled Communities of Borgu: a Recipe for Armed Struggle
67 AFRREV VOL. 11 (2), S/NO 46, APRIL, 2017 AN INTERNATIONAL MULTI-DISCIPLINARY JOURNAL, ETHIOPIA AFRREV VOL. 11 (2), SERIAL NO. 46, APRIL, 2017: 67-82 ISSN 1994-9057 (Print) ISSN 2070-0083 (Online) DOI : http://dx.doi.org/10.4314/afrrev.v11i2.6 The Politics of Neglect in the Resettled Communities of Borgu: A Recipe for Armed Struggle Niworu, Salihu Mohammed Department of Political Science Faculty of Management and Social Sciences Ibrahim Badamasi University, Lapai, Niger State, Nigeria E-mail: [email protected], [email protected] -------------------------------------------------------------------------- Abstract This paper attempted a contribution to finding solution to the incessant armed agitations that bedevilled all regions of the Nigerian political economy. Common consumption goods have eluded majority of the less privileged Nigerians. In cognizance of this, aggrieved youths take up arms in agitation for a fair share of the wealth that accrued to the federal government from the natural endowments of their local communities. The Borgu resettled communities are not exonerated from the politics of neglect and deprivations other regions are amplifying to the global community. Borgu produces electricity, but they do not have light, no quality schools, good access roads and efficient health facilities in spite of the sacrifices they make for national development. The paper recommended among others that good roads, electricity, health facilities and schools be provided for the people of Borgu. Copyright © International Association of African Researchers and Reviewers, 2006-2017: www.afrrevjo.net. Indexed African Journals Online: www.ajol.info 68 AFRREV VOL. 11 (2), S/NO 46, APRIL, 2017 Introduction Power in whatever perspective it is viewed, be it political, economic or electric power, is very central in the production process of any given political economy. -

Microbiological Survey and Appraisal of Local Milk Production in Kwara and Niger State, Nigeria Okeke, K.S*1, Makun, H
G.J.B.A.H.S.,Vol.5(2):139-153 (April-June,2016) ISSN: 2319 – 5584 Microbiological Survey and Appraisal of Local Milk Production in Kwara and Niger State, Nigeria Okeke, K.S*1, Makun, H. A2, Damisa, D3, Akoma, O4 1 Department of Nutrition and Dietetics,The Federal Polytechnic Bida, Niger State, Nigeria. 2 Department of Biochemistry, Federal University of Technology, Minna, Nigeria. 3Department of Microbiology, Federal University of Technology, Minna, Nigeria. 4 Department of Science Laboratory Technology, The Federal Polytechnic Bida, Nigeria. *Corresponding Author Abstract The study appraised Information regarding the demographic data, milk production practices, cattle feeds management, transportation and marketing of milk products. A well-structured questionnaire and field observations was used to collect data from local milk producers with lactating cows and vendors from Niger and Kwara State. There was a great variation in dairy production practises across the two states. Result indicates that more than 70% of respondents were females below 20years of age. The respondents were mostly Fulani 80%-100%, across the two States. In terms of Educational qualifications, 90%-100% of the Pastoralists in all the LGAs did not attend Western education. The use of bottles in marketing of milk products was observed in Agaie LGA. Eight out of ten LGAs surveyed revealed 45%-100% no sanitary inspector visitation or inspection of their milk product. This study presents findings that could be used for planning strategies for standardization of processing methods of dairy products and forming of policies that can lead to the improvement of the dairy industry as well as public health safety Key words: dairy farm, microbiological survey, milk products, Traditional Technology, 1.0 Introduction Dairy production contributes about 12.7% of agricultural gross domestic products in Nigeria. -

International Journal of Language, Literature and Gender Studies (LALIGENS), Bahir Dar- Ethiopia Vol
1 LALIGENS, VOL. 8(2), S/N 18, AUGUST/SEPT., 2019 International Journal of Language, Literature and Gender Studies (LALIGENS), Bahir Dar- Ethiopia Vol. 8 (2), Serial No 18, August/Sept., 2019:1-12 ISSN: 2225-8604(Print) ISSN 2227-5460 (Online) DOI: http://dx.doi.org/10.4314/laligens.v8i2.1 BABEL OF NIGER STATE 1IHENACHO, A. A., JAMIU, A. M., AGU, M. N., EBINE, S. A., ADELABU, S. & OBI, E. F. Faculty of Languages and Communication Studies IBB University, Lapai, Niger State, Nigeria 1+2348127189382 [email protected] Abstract This paper is a preliminary report on an ongoing research being carried out in the Faculty of Languages and Communication Studies of Ibrahim Badamasi Babangida University, Lapai, Niger State, Nigeria. The research is on ‘Language education and translation in Niger State’. The languages involved in the research are: Arabic, English, French, Gbagyi, Hausa and Nupe. The aim of this research which is funded by the Nigerian Tertiary Education Trust Fund (TETFund) is ‘to help improve the outcome of language education and translation in Niger State in both quality and quantity’ As a preliminary inquiry, the research team visited 78 institutions of learning at all levels (primary, secondary and tertiary) in all the three geopolitical zones of Niger State, as well as media houses located in the capital, Minna, and obtained responses to the questionnaires they took to the institutions. While pursuing the aim and objectives of their main research, the team deemed it necessary to consider the position (and the plight) of the multiplicity of other languages of Niger State (than the three major ones – Gbagyi, Hausa and Nupe) in relation to Nigeria’s language policy in education.