Equality and Diversity Demographics 2019 Comparative Data The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Agency Information - Environmental Health (V3.0 2020 July) Page 1 of 2
Information about agencies to be shared in ‘Making Enquiries under S.42’ training 1. Who are we? Environmental Health Service 2. Who are we? Each Local Authority, with the exception of Derbyshire County Council (DCC), has environmental health professionals in the form of Environmental Health Officers (EHOs)/ Environmental Health Practitioners (EHPs)/ Environmental Health Technical Officers (EHTO), Enforcement Officers who can enforce various types of public health, housing, pollution, food and health and safety legislation. They are primarily regulatory officers but do play a major role in protecting public health, maintaining a safe environment and have both technical and scientific expertise to offer support and advice to partnering agencies, businesses, community groups and the public. 3. What do we do? (The below text sets out some of the relevant areas in s.42 enquiries, but is not limited to these items). EHOs/EHPs/EHTOs/Enforcement Officers have a regulatory role in ensuring public safety in a wide number of areas; being responsible for carrying out measures to protect public health, enforcing legislation relating to the natural and built environments that benefit human health and providing support to minimize health and safety hazards. Particular statutory obligations relate to domestic home environments to ensure ‘fitness for habitation’ by the removal of serious hazards (known as Category 1 hazards*) to achieve the ideal standards within a property. The risk of harm to a person may arise given physical and psychological hazards in the home environment i.e. structural collapse, carbon monoxide from defective appliances, or excess cold from poorly heated and insulated homes. Table 1 below indicates some of the key hazard areas which are checked when a property is assessed by an EH Professional. -

Feeding Derbyshire Healthy Holidays Programme October Half-Term 2020 Report
Feeding Derbyshire Healthy Holidays Programme October Half-Term 2020 Report Introduction Feeding Derbyshire worked with 15 independent Healthy Holidays Clubs across all districts of Derbyshire. 14 have submitted their feedback to date. As in the Summer Holidays, we made a universal offer to the holiday clubs, providing food and take-home activities to children living within the areas they served. Club organisers ensured that vulnerable families and those on Free School Meals were made aware of and signed up to the programme. School Holiday Clubs supported All of the 15 Holiday Clubs opted to receive a Fareshare subscription. This October, the FareShare offer that Feeding Derbyshire subscribed to consisted of three days’ supply of food for each week that a child attended the holiday club. This included: 6 pieces of fruit for each child Breakfast products Lunch making ingredients Hot meal ingredients Locations served by the School Holiday Clubs Heanor, Langley Mill, Loscoe, Langley, Amber Valley Riddings, Amber Valley Hurst Farm, Matlock, Derbyshire Dales Kirk Hallam, Erewash Long Eaton, Sawley and Sandiacre, Erewash Rother Ward Chesterfield Staveley, Barrow Hill, Poolsbrook, Hollingwood, Mastin Moor, Duckmanton , Inkersall, Chesterfield. Grassmoor, NE Derbyshire Holmewood and Heath, NE Derbyshire Creswell, Bolsover Doe Lea, Bolsover Buxton, High Peak Swadlincote, South Derbyshire Volume of Food Supplied. FareShare have confirmed that 10.5 tonnes of food was distributed to the 15 School Holiday Clubs taking part in the Healthy Holidays programme over the October half-term. This is equivalent to 25,000 meals. 1 Total Number of Children/Families Supported Using the figures supplied by the 14 Holiday Clubs that have submitted their feedback, 2054 children and their families benefitted from the Healthy Holidays Programme. -

Crime Reduction & Community Safety Group Tilley Awards 2008
Crime Reduction & Community Safety Group Tilley Awards 2008 Application form Please ensure that you have read the guidance before completing this form. By making an application to the awards, entrants are agreeing to abide by the conditions laid out in the guidance. Please complete the following form in full, within the stated word limit and ensuring the file size is no more than 1MB. Failure to do so will result in your entry being rejected from the competition. Completed application forms should be e-mailed to [email protected]. All entries must be received by noon on Friday 25th April 2008. No entries will be accepted after this time/date. Any queries on the application process should be directed to Alex Blackwell on 0207 035 4811. Section A: Application basics 1. Title of the project: The Thickley Bank Project/Partnership Intervention at Neighbourhood Level 2. Key issue that the project is addressing e.g. Alcohol related violence: Alcohol related crime, anti social behaviour, general disorder, criminal damage, secondary fires and lack of community confidence. Author contact details 3. Name of application author: Councillor Brian R. Murray-Carr 4. Organisation submitting the application: Bolsover Community Safety Partnership 5. Full postal address: Bolsover District Council, Sherwood Lodge, Bolsover, Derbyshire, S44 6NF 6. Email address: [email protected] 7. Telephone number: 01246 242589 Secondary project contact details 8. Name of secondary contact involved in the project: Carolyn Bowen 9. Secondary contact email address: [email protected] 10. Secondary contact telephone number: 01246 242589 Page 1 of 9 The Thickley Bank Project/Partnership Intervention at Neighbourhood Level Endorsing representative contact details 11. -

NHS Derby and Derbyshire Clinical Commissioning Group Constitution V3.8
NHS Derby and Derbyshire Clinical Commissioning Group Constitution NHS Derby and Derbyshire Clinical Commissioning Group Constitution v3.8 VERSION CONTROL Version Effective Date Changes 1.0 August 2018 Standard model 2.0 15 October 2018 Draft NHS Derby and Derbyshire CCG Constitution 2.1 13 November 2018 Updated Draft NHS Derby and Derbyshire CCG Constitution with NHSE Feedback 2.2 28 November 2018 Updated Draft NHS Derby and Derbyshire CCG Constitution with NHSE Feedback 2.3 11 December 2018 Updated Draft NHS Derby and Derbyshire CCG Constitution with NHS Feedback, E Polgar NHS England , Derbyshire CCG’s Lay Members and Engagement with the Derbyshire CCGs membership 2.4 25 January 2019 Updated Draft NHS Derby and Derbyshire CCG Constitution following approval of the draft at the Derbyshire CCGs Governing Body Meetings in Common 24 January 2019 3.0 31 January 2019 Updated Draft NHS Derby and Derbyshire CCG Constitution following formal feedback from NHS England received 31.1.19 3.1 19 February 2019 Final Approved NHS Derby and Derbyshire CCG Constitution 3.2 13 February 2020 Updated Terms of Reference for Primary Care Commissioning Committee and Audit Committee. 3.3. 8 April 2020 Updated 1.1, 2.2, 2.3, 2.10 and 4.1of Annexure 1: Decisions, Authorities and Duties Delegated to Officers of the CCG Governing Body; for the duration of the COVID-19 emergency, as approved by the CCG Governing Body on 2 April 2020 3.4 16 April 2020 Updated Section 3.6 GB Quorum of Appendix 3: Standing Orders, for the duration of the COVID-19 emergency, as approved by the CCG Governing Body on 16 April 2020. -

The Ultimate Peak District & Derbyshire Bucket List
The Ultimate Peak District & Derbyshire Bucket List: 101 Great Things To Do 1. Embrace the great outdoors in the UK’s first National Park Established in 1951, the Peak District is the country’s oldest National Park. If you love the outdoors, this protected area of natural beauty - which covers 555 square miles in total - offers over 200 square miles of stunning open access land to explore. 2. Visit the ‘jewel in the Peak District’s crown’ at Chatsworth House Home to the Duke and Duchess of Devonshire, Chatsworth is one of the UK’s favourite stately homes. Discover over 30 magnificent rooms, a 105-acre garden, parkland, a farmyard and playground, and one of Britain’s best farm shops. 3. Conquer the tallest ‘Peak’ in the Peak District At 636 metres above sea level, you’ll feel like you’re standing on top of the world when you conquer the Kinder Scout plateau. It’s the highest point in the National Park and was also the site of the 1932 Mass Trespass, a landmark event which sparked a debate about the right to roam in the countryside, leading to the establishment of the Peak District as the first National Park two decades later. 4. Discover the UK’s oldest Ice Age cave art at Creswell Crags Walk in the footsteps of Ice Age hunters, uncover the secrets of early man, discover incredible Ice Age cave art and marvel at the UK’s largest discovery of ritual protection marks at this picturesque limestone gorge on the Derbyshire/Nottinghamshire border. 5. -

William Henry Oliver
1 WILLIAM HENRY OLIVER 1881 3437 f 48 Cutthorpe Oliver William H 25 Police constable Bonsall Lucy A w 20 Church broughton Henrietta d 2 Cutthorpe Grace B d 8m Cutthorpe 1891 2761 f 113 Marsden St Chesterfield Oliver William H 35 Police sergeant Bonsall Lucy A w 30 Church broughton Henrietta d 12 Brampton Grace B d 10 Brampton Charlotte d 8 Brampton Millicent d 6 Brampton Ellen d 4 Chesterfield Jackson William F boarder 28 Groom Church broughton 1901 3254 f33 Hockley Bolsover Oliver William H 45 Police sergeant Bonsall Lucy A w 40 Church broughton Henrietta d 22 Dressmaker Cutthorpe Grace d 20 Dressmaker Church broughton Ellen d 14 Chesterfield 1911 440/8/21240 20 Hardwick St Buxton Oliver William H 55 County court bailiff Bonsall Lucy Ann w 50 Church broughton married 32 years; 5 childen, all living William Henry Oliver Baptised 30 Sept 1855 .s James, fwk & Millicent Bonsall Married Lucy Ann Jackson Oct-Dec 1877 Burton on Trent 6b 51 Lucy Ann died 16/10/1918 Islington Died 28 Feb 1917; living at 7 Hall Bank Buxton Admin 15 March to Lucy Ann, widow; Effects £98/15/10 Children Henrietta bp 4/5/1879 Old Brampton; married Arthur Taylor Wright 27/5/1901 Bolsover 1911 Living New Mills ; husband a hand engraver to calico printer; b Cutthorpe Grace Olivia bp 8/8/1880 Church broughton; m Reid Bowman 1904 Hayfield Reg D 1911 living New Mills ; husband engraver to calico printer Died 25/7/ 1964 Stockport FACH ID: BRCL01 PC William Henry Oliver Researcher: Clive Leivers 2 Charlotte bp 20/8/1882; married John Gardner Campbell 2/3/1904 St John's Buxton -

A632 Matlock to County Boundary Draft Speed Limit Order
THE DERBYSHIRE COUNTY COUNCIL ROAD TRAFFIC REGULATION ACT 1984 (A632 MATLOCK TO COUNTY BOUNDARY AND ADJACENT ROAD) (30MPH, 40MPH AND 50MPH SPEED LIMIT) ORDER 2020 Derbyshire County Council hereby gives notice that it proposes to make an Order under the Road Traffic Regulation Act 1984, the effect of which will be, in respects of roads in the Districts of Derbyshire Dales, North-East Derbyshire and Bolsover and the Borough of Chesterfield: It is proposed to consolidate all Speed Limit Traffic Regulation Orders pertaining to the A632 from its junction with the A615 in Matlock to its County Boundary with Nottinghamshire and its adjacent road of Vernon Lane in Kelstedge. There will be no changes to the current speed limits or position of the existing speed limits. This technical adjustment will assist the police with their enforcement duties. Due to ongoing Covid 19 social distancing requirements a copy of the Order and documents giving more detailed particulars of the Order are available on request by emailing [email protected] or calling 01629 538674 until 6 weeks after the Order is made. For plans, a copy of the notice and the statement of reasons please go to: www.derbyshire.gov.uk/council/public-and-statutory-notices/public-and- statutory-notices.aspx All objections and other representations to the proposal must (a) be in writing (b) state the grounds on which it is made and (c) provide a name and address for contact purposes (d) be sent to the Interim Director – Economy, Transport and Environment, Derbyshire County Council, County Hall, Matlock DE4 3AG (For Attention of Traffic and Safety Team quoting reference Z3237) or email [email protected] by Friday 18th September 2020. -

Valley Road, Bolsover, Chesterfield, Derbyshire Guide Price £190,000
Valley Road, Bolsover, Chesterfield, Derbyshire Asking Price: £175,000 Freehold reedsrains.co.uk Chesterfield T: 01246 236991 Valley Road, Bolsover, Chesterfield, Derbyshire Asking Price: £175,000 Freehold No upward chain is offered on this well Bedroom One presented two bedroom detached bungalow. 9'6" x 12'2" (2.9m x 3.7m) Internally the property does require some Benefitting from a wall of fitted wardrobes, modernisation however it is sat on a lovely plot laminate flooring, double glazed window to the with excellent views over countryside on the rear and wall mounted radiator. rear patio. There is ample parking, single detached garage with workshop and an Bedroom Two enclosed private garden. Call now to arrange 10'2" x 12'6" (3.1m x 3.8m) your early viewing. EPC D. Having a double glazed window to the rear, sliding patio door to the rear, fitted wardrobes Entrance Hall and wall mounted radiator. Having a double glazed door to the side giving access into the hallway. The hallway Outside comprises of a wall mounted radiator and a To the front of the property is a lawned garden. loft hatch to the ceiling. To the side is a driveay providing ample off street parking and this inturn leads to single Kitchen detached garage. The single garage benefits 9'10" x 9'10" (3m x 3m) from an up and over door, power and lighting Fitted with range of wall and base units with and also haing a separate workshop area. The roll edge work surfaces. There is space for a rear garden is low maintenance and benefits free standing electric cooker, space for a from a patio with beautiful views over open For full EPC please contact the branch. -

Minutes of the Annual Parish Meeting Held in Tibshelf Village Hall, 110
Minutes of the MEETING of TIBSHELF PARISH COUNCIL held in The Parish Meeting Room, Tibshelf Village Hall, 110 High Street, Tibshelf. DE55 5NU on Tuesday 16th July 2019 at 7.00pm Present: Councillors A Beckett, P Billington, I Brentnall, M Coupe, G Foley, K M Salt MBE, R Vaughan, D S Watson, C Whitehead and S E Wood In attendance: Mrs. R Price Parish Clerk, One member of the public NON-EXEMPT ITEMS 0719/2145 Apologies for Absence An apology for absence was received from Councillor R Heffer 0719/2146 Declarations of Members Interests Councillor R Vaughan declared an interest in Item 11 on the agenda 0719/2147 Public Speaking Members of the Public: A member of the public raised an issue concerning the need for clear and regular communications from the parish council to keep residents informed and asked what they planned to do to improve communication between the electorate and the elected. He also asked about the provision of dog bins in the parish. The Chair informed the resident that the issue of improving communication was being dealt with as a priority. She also explained that there were 14 dog bins provided throughout the parish and that the parish council provided dog bags free of charge. Police: The police were not present County Council: Cllr. Moesby was not present District Council: Councillor Watson informed members that the BDC were looking at all pockets of land that they owned and assessing whether they should dispose of them 0719/2148 Minutes of the Parish Council Meeting held on 18th June 2019 It was Proposed by Councillor Coupe, Seconded by Councillor Whitehead and RESOLVED that the Minutes of the Meeting of Tibshelf Parish Council held on 18th June 2019 be approved as an accurate record, The minutes were duly signed by the Chairman. -
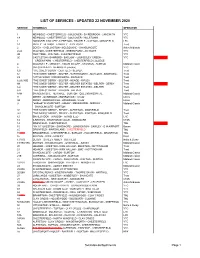
List of Services - Updated 22 November 2020
LIST OF SERVICES - UPDATED 22 NOVEMBER 2020 SERVICE TERMINALS OPERATOR 1 NEWBOLD - CHESTERFIELD - BOLSOVER - SHIREBROOK - LANGWITH YTC 1A NEWBOLD - CHESTERFIELD - BOLSOVER - HILLSTOWN YTC 1 "MANSFIELD MILLER" ALFRETON - TIBSHELF - SUTTON - MANSFIELD LRC 1A RIPLEY - HEANOR - LANGLEY - ALDERCAR Trent 2 DERBY - CHELLASTON - MELBOURNE - SWADLINCOTE Arriva Midlands 2/2A WALTON - CHESTERFIELD - GREEN FARM - ASHGATE YTC 2B YEW TREE - WALTON - CHESTERTFIELD YTC 2C CASTLETON - BAMFORD - BASLOW - LOUNDSLEY GREEN - YTC GREEN FARM - CHESTERFIELD - CHESTERFIELD COLLEGE 4 WOODVILLE - MIDWAY - SWADLINCOTE - STANTON - BURTON Midland Classic 5 CHESTERFIELD - NEWBOLD (circular) YTC 6.0 "THE SIXES" DERBY - DUFFIELD - BELPER Trent 6.1 "THE SIXES" DERBY - BELPER - WIRKSWORTH - MATLOCK - BAKEWELL Trent LS "LITTLE SIXES" WIRKSWORTH - MATLOCK Trent 6.2/6.3/6E "THE SIXES" DERBY - BELPER - HEAGE - RIPLEY Trent 6N "THE SIXES" DERBY - BELPER - BELPER ESTATES - BELPER - DERBY Trent 6.4 "THE SIXES" DERBY - BELPER - BELPER ESTATES - BELPER Trent 6.X "THE SIXES" DERBY - KILBURN - BELPER Trent 8/8H SWADLINCOTE - NEWHALL - BURTON - QUEENS HOSPITAL Midland Classic 9 DERBY - OCKBROOK - BORROWASH circular Littles 9A DERBY - BORROWASH - OCKBROOK circular Littles 9 "airline9 " E M AIRPORT - ASHBY - MELBOURNE - MIDWAY - Midland Classic SWADLINCOTE - BURTON 9.1 "THE NINES" DERBY - RIPLEY - ALFRETON - MANSFIELD Trent 9.3 "THE NINES" DERBY - RIPLEY - ALFRETON - PINXTON - MANSFIELD Trent 12 SHIREBROOK - WARSOP - MANSFIELD LRC 14 ILKESTON - STANTON-BY-DALE - SANDIACRE CT4N 14 DRONFIELD -

Promote Healthy Lifestyles Presentation
Priority 2: Healthy lifestyles Promote healthy lifestyles by developing services to prevent and reduce harmful alcohol consumption, substance misuse, obesity, physical inactivity, smoking and sexual ill-health Focus on preventing and reducing alcohol misuse, obesity and physical inactivity • 1 Derbyshire Population Size Pyramid (2010-2035) • 2 • 3 90+ Male Female 85-89 80-84 75-79 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 0-4 35000 25000 15000 5000 5000 15000 25000 35000 Source: 2010-Based Population Projections, Office for National Statistics (ONS), March 2012 Male 2010 Female 2010 Male 2035 Female 2035 • For both men and women, • Over the next twenty-five • The population increase will be there are more people in the years, it is expected that particularly pronounced among 45-49 and 40-44 brackets than almost all age groups will the older age groups, with any other age band have higher numbers than substantial increase for every they do now age group over 65 • Bolsover had the highest • Derbyshire’s adult obesity obesity rate, at 27.4% of the rate was 25.3%, which is 1.1 adult population. Derbyshire percentage points higher Dales had the lowest rate at than the national average 23.0% (24.2%) Percentage of the adult population with obesity 2006-2008 35 30 25 20 15 over 27.4 26.5 26.8 25.1 23.3 25.8 24.0 25.3 24.2 10 23.0 5 0 Percentage of people aged 16 and Amber Bolsover Chesterfield Derbyshire Erewash High Peak North East South Derbyshire England Valley Dales Derbyshire Derbyshire Source: 2006-2008, -

Gould-Aalco Markham Vale Chesterfield
From From M18 Eckington Sheffield B6052 From Gould Alloys Ltd Worksop Markham Lane A6135 Markham Vale A619 Chesterfield S44 5HS B6419 J30 Tel : +44 (0)1246 263300 B6053 A616 Clowne J34 Maltby Rotherham M18 B6051 A61 J33 Sheffield J32 B6052 Staveley A619 A57 J31 B6050 A61 A57 A57 B6050 B6050 M1 B6418 A625 A6135 M1 Worksop Cutthorpe Brimington Dronfield A619 Shuttlewood J29a A619 A61 J30 See Inset A619 B6051 A61 B6150 A619 Chesterfield B6417 CHESTERFIELD J29a Chesterfield A619 Bolsover Bakewell M1 A619 A632 A632 Bolsover A617 A60 BakewellFrom A619 A6 A632 A61 J29 A617 A617 From Ollerton From M1 Southbound A61 Leave the M1 at Junction 29a, at the roundabout at the end of the A632 slip road take the first exit onto the A6192 towards Chesterfield / Markham Vale & Bolsover. At the next roundabout take the first exit to remain onto Markham Lane. Inset Continue for 200 metres and you will find us on the left hand side. Wingerworth From M1 Northbound J29 B6417 Leave the M1 at Junction 29a, at the roundabout at the end of the slip road take the fourth exit onto the A6192 towards Chesterfield A6172 / Markham Vale & Bolsover. A617 At the next roundabout take the first exit to remain onto Markham n Lane. L m a From Continue for 200 metres and you will find us on the left hand side. h k r A6175 Mansfield J29a a M1 From M18 M North Follow the M18 southbound leaving at Junction 32 to join the M1 Markham Rd Wingfield southbound. Leave the M1 at Junction 29a, at the roundabout at the end of the slip road take the first exit onto the A6192 towards Chesterfield M1 N / Markham Vale & Bolsover.