Cals Provider Manual the First 30 Minutes Edition 15 2019
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Safety of Heparin Bridging Therapy for Transrectal Ultrasound-Guided Prostate Biopsy in Patients Requiring Temporary Discontinua
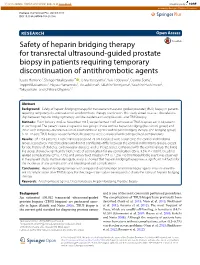
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Springer - Publisher Connector Hamano et al. SpringerPlus (2016) 5:1917 DOI 10.1186/s40064-016-3610-6 RESEARCH Open Access Safety of heparin bridging therapy for transrectal ultrasound‑guided prostate biopsy in patients requiring temporary discontinuation of antithrombotic agents Itsuto Hamano1, Shingo Hatakeyama1* , Tohru Yoneyama2, Yuki Tobisawa1, Osamu Soma1, Teppei Matsumoto1, Hayato Yamamoto1, Atsushi Imai2, Takahiro Yoneyama2, Yasuhiro Hashimoto2, Takuya Koie1 and Chikara Ohyama1,2 Abstract Background: Safety of heparin bridging therapy for transrectal ultrasound-guided prostate (TRUS) biopsy in patients requiring temporary discontinuation of antithrombotic therapy is unknown. This study aimed to assess the relation- ship between heparin bridging therapy and the incidence of complications after TRUS biopsy. Methods: From January 2005 to November 2015, we performed 1307 consecutive TRUS biopsies on 1134 patients in our hospital. The patients were assigned to two groups: those without heparin bridging (the control group) and those with temporary discontinuation of antithrombotic agents with heparin bridging therapy (the bridging group). A 10–12-core TRUS biopsy was performed; the patients were evaluated for bleeding-related complications. Results: Of 1134 patients, 1109 (1281 biopsies) and 25 (26 biopsies) were assigned to the control and bridging group, respectively. Patient background did not significantly differ between the control and bridging groups, except for age, history of diabetes, cardiovascular diseases, and CHADS2 scores. Compared with the control group, the bridg- ing group showed a significantly higher rate of complication for any complication (35 vs. 8.3%, P < 0.001), bleeding- related complications (27 vs. -

Predictive Score for Positive Upper Endoscopies Outcomes in Children with Upper Gastrointestinal Bleeding. Score Prédictif De L
Predictive score for positive upper endoscopies outcomes in children with upper gastrointestinal bleeding. score prédictif de la présence de lésions endoscopiques dans l’hémorragie digestive haute de l’enfant Sonia Mazigh 1, Rania Ben Rabeh 1, Salem Yahiaoui 1, Béchir Zouari 2, Samir Boukthir 1, Azza Sammoud 1 1- Service de médecine C Hôpital d'enfants Béchir Hamza de Tunis- Université de Tunis El Manar, Faculté de Médecine de Tunis 2- Département d'épidémiologie et de médecine préventive - Université Tunis El Manar, Faculté de Médecine de Tunis, résumé summary Prérequis: L'hémorragie digestive haute (HDH) est une urgence Background: Upper gastrointestinal bleeding (UGIB) is a common fréquente en pédiatrie. L'endoscopie digestive haute (EDH) est pediatric emergency. Esophago-gastro-duodenoscopy (EGD) is the l'examen de choix pour identifier l’origine du saignement. first line diagnostic procedure to identify the source of bleeding. Néanmoins l’étiologie demeure inconnue dans 20% des cas. En However etiology of UGIB remains unknown in 20% of cases. outre, l'endoscopie d'urgence n'est pas disponible dans de Furthermore, emergency endoscopy is unavailable in many hospitals nombreux hôpitaux dans notre pays . in our country. Objectifs: Décrire les lésions endoscopiques retrouvées chez Aims: Identify clinical predictors of positive upper endoscopy l'enfant dans l'HDH, identifier les facteurs prédictifs de la présence outcomes and develop a clinical prediction rule from these de ces lésions et élaborer un score clinique à partir de ces parameters. paramètres. Methods: Retrospective study of EGDs performed in children with Méthodes: Etude rétrospective des EDH réalisées chez les enfants first episode of UGIB, in the endoscopic unit of Children's Hospital of présentant un premier épisode d'HDH, à l'unité d'endoscopie Tunis, during a period of six years. -

Colorectal Cancer Health Services Research Study Protocol: the CCR-CARESS Observational Prospective Cohort Project José M
Quintana et al. BMC Cancer (2016) 16:435 DOI 10.1186/s12885-016-2475-y STUDYPROTOCOL Open Access Colorectal cancer health services research study protocol: the CCR-CARESS observational prospective cohort project José M. Quintana1,8* , Nerea Gonzalez1,8, Ane Anton-Ladislao1,8, Maximino Redondo2,8, Marisa Bare3,8, Nerea Fernandez de Larrea4,8, Eduardo Briones5, Antonio Escobar6,8, Cristina Sarasqueta7,8, Susana Garcia-Gutierrez1,8, Urko Aguirre1,8 and for the REDISSEC-CARESS/CCR group Abstract Background: Colorectal cancers are one of the most common forms of malignancy worldwide. But two significant areas of research less studied deserve attention: health services use and development of patient stratification risk tools for these patients. Methods: Design: a prospective multicenter cohort study with a follow up period of up to 5 years after surgical intervention. Participant centers: 22 hospitals representing six autonomous communities of Spain. Participants/Study population: Patients diagnosed with colorectal cancer that have undergone surgical intervention and have consented to participate in the study between June 2010 and December 2012. Variables collected include pre-intervention background, sociodemographic parameters, hospital admission records, biological and clinical parameters, treatment information, and outcomes up to 5 years after surgical intervention. Patients completed the following questionnaires prior to surgery and in the follow up period: EuroQol-5D, EORTC QLQ-C30 (The European Organization for Research and Treatment of Cancer quality of life questionnaire) and QLQ-CR29 (module for colorectal cancer), the Duke Functional Social Support Questionnaire, the Hospital Anxiety and Depression Scale, and the Barthel Index. The main endpoints of the study are mortality, tumor recurrence, major complications, readmissions, and changes in health-related quality of life at 30 days and at 1, 2, 3 and 5 years after surgical intervention. -
A Guide for Parents Whose Child Needs an Operation
Who Will Hold My Hand? A GUIDE FOR PARENTS WHOSE CHILD NEEDS AN OPERATION FROM THE AMERICAN COLLEGE OF SURGEONS Kathryn D. Anderson, MD, FACS, FRCS Who Will Hold My Hand? A GUIDE FOR PARENTS WHOSE CHILD NEEDS AN OPERATION ii The information and advice in this book are based on the training, personal experiences, and research of the author. Its contents are obtained from sources the author believes to be reliable; however, the information presented is not intended to substitute for professional medical advice. The author and the publisher urge you to consult with your physician or other qualified health care provider prior to starting any treatment or undergoing any surgical procedure. Because there is always some risk involved, the author and publisher cannot be responsible for any adverse effects or consequences resulting from the use of any of the suggestions, preparations, or procedures described in this book. Copyright © 2009 by American College of Surgeons at 633 N. Saint Clair Street Chicago, IL 60611-3211 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the copyright owners. iii Table of Contents Acknowledgments viii Introduction 1 PART 1: Let’s Walk through the Day of the Operation 5 1 What Happens Before and After the Operation? 7 GETTING READY FOR THE OPERATION 7 DURING THE PROCEDURE 10 RECOVERY 11 INTENSIVE CARE 12 SCARS 14 2 What -

The Clinical Management of Acute Mechanical Small Bowel Obstruction
22 Osteopathic Family Physician (2015) 22 - 26 Osteopathic Family Physician, Volume 7, No. 6, November/December, 2015 REVIEW ARTICLE Te Clinical Management of Acute Mechanical Small Bowel Obstruction Cliford Medina, MD, MBA, FACP1 and Matthew Kalliath, OMS-IV2 1McLeod Inpatient Physicians 2Edward Via College of Osteopathic Medicine - Carolinas Campus KEYWORDS: Acute mechanical small bowel obstruction (AMSBO) is a common emergency and a significant cause of hospitalization. Due to the variation in small bowel obstruction-related symptomatology, many patients are unaware Small Bowel of the seriousness of their clinical condition and do not seek immediate medical attention. Consequently, such Obstruction patients forego a visit to the hospital emergency department and often present to their primary care physician (PCP). PCPs, with hospital admitting privileges, and other hospital-based physicians, must have a sound understanding Conservative of the principles underlying the treatment of AMSBO. All patients with suspected AMSBO should be hospitalized Management and treated initially with conservative management. This includes bowel rest with early decompression, fluid resuscitation, and correction of electrolyte abnormalities. Water-soluble contrast medium can be useful adjunct in this approach; it has both diagnostic and therapeutic purposes. Furthermore, water-soluble contrast medium is safe and reduces the need for surgery, time to resolution and hospital stay. Non-operative management can be prolonged up to 72 hours in the absence of strangulation or peritonitis. In contrast, ambulatory patients presenting with ominous clinical signs and symptoms should be considered for immediate surgical intervention. Indications for surgery include strangulation, peritonitis, intractable vomiting, complete or closed loop bowel obstruction, or failure to improve after 72 hours of conservative management. -

Chapter 11 SURGICAL EMERGENCIES Learning Objectives: • Assess, Resuscitate and Stabilize a Surgical Emergency Patient’S Condition Rapidly and Accurately
Chapter 11 SURGICAL EMERGENCIES Learning Objectives: • Assess, resuscitate and stabilize a surgical emergency patient’s condition rapidly and accurately. • Understand the basic pathophysiology of Traumatic brain injury. • Evaluate patients with head injuries. • Perform a focused neurologic examination. • Explain the importance of adequate resuscitation in limiting secondary brain injury. • Determine the need for patient transfer, admission, consultation, or discharge. • Arrange appropriately for a patient’s inter-hospital or intra-hospital transfer (what, who, when, how). CLINICAL ORIENTATION MANUAL SURGICAL AND NON-SURGICAL EMERGENCIES INTRODUCTION Trauma is a leading cause of death and disability in Bhutan. Motor vehicle crashes caused the maximum deaths in last couple of years followed by fall injuries either in the farm work setting or at the construction sites leading to significant morbidity and mortality. On the other hand, surgical emergencies pose a significant anxiety and dilemma to the local health staff as well as to the patient where there is no surgical set up. It is important to at least alleviate the anxiety of the patient and also to know which cases require urgent surgical consultation or immediate transfer to the surgical centers. Surgical emergencies focus on general trauma, head injury, burns, wound care, pediatric trauma, and trauma in pregnancy and non-traumatic surgical emergencies. APPROACH TO TRAUMA Definition: Trauma is defined as any physical injury severe enough to pose a threat to limb or life. Patient assessment a) Pre-hospital phase: responsibility of first responder and basic life support provider (HHC and EMRs). b) Hospital phase: hospital emergency response. Triage: system of making a rapid assessment of each patient and assigning a priority rating on the basis of clinical need and urgency with the goal to do the greatest good for the greatest number. -

Bologna Guidelines for Diagnosis
ten Broek et al. World Journal of Emergency Surgery (2018) 13:24 https://doi.org/10.1186/s13017-018-0185-2 REVIEW Open Access Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group Richard P. G. ten Broek1,39*†, Pepijn Krielen1†, Salomone Di Saverio2, Federico Coccolini3, Walter L. Biffl4, Luca Ansaloni3, George C. Velmahos5, Massimo Sartelli6, Gustavo P. Fraga7, Michael D. Kelly8, Frederick A. Moore9, Andrew B. Peitzman10, Ari Leppaniemi11, Ernest E. Moore12, Johannes Jeekel13, Yoram Kluger14, Michael Sugrue15, Zsolt J. Balogh16, Cino Bendinelli17, Ian Civil18, Raul Coimbra19, Mark De Moya20, Paula Ferrada21, Kenji Inaba22, Rao Ivatury21, Rifat Latifi23, Jeffry L. Kashuk24, Andrew W. Kirkpatrick25, Ron Maier26, Sandro Rizoli27, Boris Sakakushev28, Thomas Scalea29, Kjetil Søreide30,31, Dieter Weber32, Imtiaz Wani33, Fikri M. Abu-Zidan34, Nicola De’Angelis35, Frank Piscioneri36, Joseph M. Galante37, Fausto Catena38 and Harry van Goor1 Abstract Background: Adhesive small bowel obstruction (ASBO) is a common surgical emergency, causing high morbidity and even some mortality. The adhesions causing such bowel obstructions are typically the footprints of previous abdominal surgical procedures. The present paper presents a revised version of the Bologna guidelines to evidence- based diagnosis and treatment of ASBO. The working group has added paragraphs on prevention of ASBO and special patient groups. Methods: The guideline was written under the auspices of the World Society of Emergency Surgery by the ASBO working group. A systematic literature search was performed prior to the update of the guidelines to identify relevant new papers on epidemiology, diagnosis, and treatment of ASBO. -

Acute Lower Gastrointestinal Bleeding
The new england journal of medicine Clinical Practice Caren G. Solomon, M.D., M.P.H., Editor Acute Lower Gastrointestinal Bleeding Ian M. Gralnek, M.D., M.S.H.S., Ziv Neeman, M.D., and Lisa L. Strate, M.D., M.P.H. This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the authors’ clinical recommendations. From the Institute of Gastroenterology A 71-year-old woman with hypertension, hypercholesterolemia, and ischemic heart and Hepatology (I.M.G.) and Medical disease, who had a cardiac stent placed 4 months earlier, presents to the emergency Imaging Institute (Z.N.), Emek Medical Center, Afula, and Rappaport Faculty of department with multiple episodes of red or maroon-colored stool mixed with clots Medicine, Technion–Israel Institute of Tech during the preceding 24 hours. Current medications include atenolol, atorvastatin, nology, Haifa (I.M.G.) — both in Israel; aspirin (81 mg daily), and clopidogrel. On physical examination, the patient is dia- and the Department of Medicine, Divi sion of Gastroenterology, University of phoretic. While she is in a supine position, the heart rate is 91 beats per minute and Washington School of Medicine, Seattle the blood pressure is 106/61 mm Hg; while she is sitting, the heart rate is 107 beats (L.L.S.). Address reprint requests to Dr. per minute and the blood pressure is 92/52 mm Hg. The remainder of the examina- Gralnek at the Institute of Gastroenterol ogy and Hepatology, Emek Medical Cen tion is unremarkable, except for maroon-colored stool on digital rectal examination. -

ACS/ASE Medical Student Core Curriculum Postoperative Care
ACS/ASE Medical Student Core Curriculum Postoperative Care POSTOPERATIVE CARE Prompt assessment and treatment of postoperative complications is critical for the comprehensive care of surgical patients. The goal of the postoperative assessment is to ensure proper healing as well as rule out the presence of complications, which can affect the patient from head to toe, including the neurologic, cardiovascular, pulmonary, renal, gastrointestinal, hematologic, endocrine and infectious systems. Several of the most common complications after surgery are discussed below, including their risk factors, presentation, as well as a practical guide to evaluation and treatment. Of note, fluids and electrolyte shifts are normal after surgery, and their management is very important for healing and progression. Please see the module on Fluids and Electrolytes for further discussion. Epidemiology/Pathophysiology I. Wound Complications Proper wound healing relies on sufficient oxygen delivery to the wound, lack of bacterial and necrotic contamination, and adequate nutritional status. Factors that can impair wound healing and lead to complications include bacterial infection (>106 CFUs/cm2), necrotic tissue, foreign bodies, diabetes, smoking, malignancy, malnutrition, poor blood supply, global hypotension, hypothermia, immunosuppression (including steroids), emergency surgery, ascites, severe cardiopulmonary disease, and intraoperative contamination. Of note, when reapproximating tissue during surgery, whether one is closing skin or performing a bowel anastomosis, tension on the wound edges is an important factor that contributes to proper healing. If there is too much tension on the wound, there will be local ischemia within the microcirculation, which will compromise healing. Common wound complications include infection, dehiscence, and incisional hernia. Wound infections, or surgical site infections (SSI), can occur in the surgical field from deep organ spaces to superficial skin and are due to bacterial contamination. -

BILIARY ATRESIA, Treatment Results and Native Liver Function
Pediatric Surgery and Pediatric Graduate School, Children’s Hospital Institute of Clinical Medicine, University of Helsinki and National Graduate School of Clinical Investigation Helsinki, Finland BILIARY ATRESIA Treatment Results and Native Liver Function HANNA LAMPELA ACADEMIC DISSERTATION To be publicly discussed, with the permission of the Faculty of Medicine, University of Helsinki, in the Niilo Hallman Auditorium, Children’s Hospital, on 1st of March 2013, at 12 noon. Helsinki 2013 Supervisor Docent Mikko Pakarinen Pediatric Surgery Pediatric Transplantation Surgery Children’s Hospital University of Helsinki Finland Reviewers Docent Tarja Ruuska Pediatrics Tampere University Hospital Tampere, Finland Docent Paulina Salminen Gastrointestinal Surgery Turku University Hospital Turku, Finland Opponent Professor Mark Davenport Paediatric Surgery King’s College Hospital London, UK ISBN 978-952-10-8592-5 (paperback) ISBN 978-952-10-8593-2 (PDF) http://ethesis.helsinki.fi Unigrafia Oy Helsinki 2013 “And if I have the gift of prophecy, and know all mysteries and all knowledge; and if I have all faith, so as to remove mountains, but have not love, I am nothing.” 1. Corinthians 13:2 CONTENTS ABSTRACT 6 LIST OF ORIGINAL PUBLICATIONS 8 ABBREVIATIONS 9 INTRODUCTION 10 REVIEW OF THE LITERATURE 11 History 11 Early descriptions 11 Development of operative techniques 11 Classifications 13 Epidemiology 14 Incidence 14 Seasonality 14 Etiology 14 Isolated BA 14 Congenital BA 15 Diagnosis 16 Symptoms and screening 16 Diagnostic tools and differential -

Stent Placement for Benign Esophageal Leaks, Perforations, and Fistulae: a Clinical Prediction Rule for Successful Leakage Control
Original article Stent placement for benign esophageal leaks, perforations, and fistulae: a clinical prediction rule for successful leakage control Authors Emo E. van Halsema1,WouterF.W.Kappelle2,BasL.A.M.Weusten3, Robert Lindeboom4, Mark I. van Berge Henegouwen5,PaulFockens1, Frank P. Vleggaar2, Manon C. W. Spaander6,JeaninE.vanHooft1 Institutions Scan this QR-Code for the authorʼs interview. 1 Department of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands 2 Department of Gastroenterology and Hepatology, University Medical Center Utrecht, the Netherlands 3 Department of Gastroenterology and Hepatology, St Antonius Hospital, Nieuwegein, the Netherlands 4 Department of Clinical Epidemiology and Biostatistics, Academic Medical Center, Amsterdam, the Netherlands ABSTRACT 5 Department of Surgery, Academic Medical Center, Background and study aims Sealing esophageal leaks by Amsterdam, the Netherlands stent placement allows healing in 44%– 94% of patients. 6 Department of Gastroenterology and Hepatology, Weaimedtodevelopapredictionruletopredictthechance Erasmus University Medical Center, Rotterdam, the of successful stent therapy. Netherlands Patients and methods In this multicenter retrospective cohort study, patients with benign upper gastrointestinal submitted 26.4.2017 leakage treated with stent placement were included. We accepted after revision 26.7.2017 used logistic regression analysis including four known clini- cal predictors of stent therapy outcome. The model per- Bibliography formance to predict successful stent therapy was evaluated DOI https://doi.org/10.1055/s-0043-118591 in an independent validation sample. Published online: 21.9.2017 | Endoscopy 2018; 50: 98–108 Results We included etiology, location, C-reactive protein, © Georg Thieme Verlag KG Stuttgart · New York and size of the leak as clinical predictors. The model was es- ISSN 0013-726X timated from 145 patients (derivation sample), and 59 pa- tients were included in the validation sample. -

Diagnosis and Treatment of Acute Appendicitis
Di Saverio et al. World Journal of Emergency Surgery (2020) 15:27 https://doi.org/10.1186/s13017-020-00306-3 REVIEW Open Access Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines Salomone Di Saverio1,2*, Mauro Podda3, Belinda De Simone4, Marco Ceresoli5, Goran Augustin6, Alice Gori7, Marja Boermeester8, Massimo Sartelli9, Federico Coccolini10, Antonio Tarasconi4, Nicola de’ Angelis11, Dieter G. Weber12, Matti Tolonen13, Arianna Birindelli14, Walter Biffl15, Ernest E. Moore16, Michael Kelly17, Kjetil Soreide18, Jeffry Kashuk19, Richard Ten Broek20, Carlos Augusto Gomes21, Michael Sugrue22, Richard Justin Davies1, Dimitrios Damaskos23, Ari Leppäniemi13, Andrew Kirkpatrick24, Andrew B. Peitzman25, Gustavo P. Fraga26, Ronald V. Maier27, Raul Coimbra28, Massimo Chiarugi10, Gabriele Sganga29, Adolfo Pisanu3, Gian Luigi de’ Angelis30, Edward Tan20, Harry Van Goor20, Francesco Pata31, Isidoro Di Carlo32, Osvaldo Chiara33, Andrey Litvin34, Fabio C. Campanile35, Boris Sakakushev36, Gia Tomadze37, Zaza Demetrashvili37, Rifat Latifi38, Fakri Abu-Zidan39, Oreste Romeo40, Helmut Segovia-Lohse41, Gianluca Baiocchi42, David Costa43, Sandro Rizoli44, Zsolt J. Balogh45, Cino Bendinelli45, Thomas Scalea46, Rao Ivatury47, George Velmahos48, Roland Andersson49, Yoram Kluger50, Luca Ansaloni51 and Fausto Catena4 Abstract Background and aims: Acute appendicitis (AA) is among the most common causes of acute abdominal pain. Diagnosis of AA is still challenging and some controversies on its management are still present among