The Acute Effects of Short and Long Durations of Plank Training on Endothelial Function
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Isometric Contractions and the Plank Same Length Muscles Worked
Isometric Contractions and the Plank If you've ever seen a mime trying to escape his invisible box, you've seen a playful example of an isometric contraction. Isometric exercises are strength-training exercises that involve the contraction of a muscle against an immovable resistance. While the mime's resistance is imaginary, you use the floor for resistance when doing an isometric plank. The isometric plank exercise provides core stability, improves posture and protects your lower back. Same Length “Iso” means same and “metric” means length, so isometric literally means “same length.” The static tension of isometric exercise strengthens the muscles at the same length -- in the position in which they are held. This can be beneficial when rehabilitating an injured joint or as a technique to improve fluid movement by overcoming weaknesses within a range of motion. It's also a good exercise technique for training the core muscles, which often must remain stable as your arms and legs move. Because isometric exercises don't move the joint through a full range of motion, you should hold isometric contractions in various positions and at varying angles to obtain maximum benefit. Muscles Worked To safely maintain the plank pose, you have to pull your belly button up toward your spine. This action, called abdominal hollowing, activates the deeper, stabilizing muscles of the core. The muscles that benefit most from an isometric plank are the transverse abdominis, obliques, rectus abdominis and erector spinae. Depending on the position you hold, the plank pose may also strengthen muscles in your wrists, arms, shoulders, chest, feet, legs and buttocks. -

Naval Special Warfare Physical Training Guide
Naval Special Warfare Physical Training Guide DISCLAIMER: Preparation for this training can be equally strenuous. You should consult a physician before you begin any strenuous exer- cise program, such as the one described here, or any diet modification, especially if you have or suspect that you may have heart disease, high blood pressure, diabetes, or any other adverse medical conditions. If you feel faint or dizzy at any time while performing any portion of this training program, stop immediately and seek medical evaluation. The United States Government and any service member or civilian employed by the United States Government disclaims any liability, personal or professional, resulting from the misapplication of any training procedure, technique, or guidance described in this guide. he Naval Special Warfare This guide provides infor- sit-ups as they are necessary TPhysical Training Guide mation about the type of train- for success at BUD/S. Cross- is designed to assist anyone ing required to properly pre- training such as cycling, who wants to improve his fit- pare for the rigors of BUD/S, rowing and hiking is useful to ness in order to take and pass and it offers a tailorable 26- rehabilitate an injury, to add the Physical Screening Test week training plan that should variety or to supplement your (PST) and succeed at Basic help a person with average basic training. Underwater Demolition/SEAL fitness prepare for training Work to improve your (BUD/S). and avoid injury. weakest areas. If you are a Most of your cardio- solid runner but a weak swim- vascular exercise should mer, don’t spend all your time General Training Guidelines focus on running and running just because you are Your workouts should be swimming, and your good at it. -

An Examination of Thigh Muscle Activations in Bridge-Plank Exercises Performed on Different Grounds
Çınarlı FS, Ölmez SB, Namaldı S, Karanfil E, Güllü K, Soylu AR. An Examination of Thigh Muscle Activations in Bridge-Plank Exercises Performed on Different Grounds. Turk J Physiother Rehabil. 2020; 31(2):156-162. doi: 10.21653/tjpr.547050 AN EXAMINATION OF THIGH MUSCLE ACTIVATIONS IN BRIDGE-PLANK EXERCISES PERFORMED ON DIFFERENT GROUNDS ORIGINAL ARTICLE ISSN: 2651-4451 • e-ISSN: 2651-446X ABSTRACT Purpose: The study aimed to examine hamstring-quadriceps muscle activations of the supine bridge and reverse plank exercises that are performed for both improving the overall body strength Turkish Journal of and contributing to the treatment in the process following an injury on different grounds. Physiotherapy and Methods: Ten participants (four males and six females, age=26.70±3.02 years) without regular Rehabilitation sports habits were included in the study. Bilateral supine bridge and bilateral reverse plank exercises were practiced randomly on stable and unstable grounds. In the study, muscle activation 2020 31(2)156-162 values of vastus medialis (VM), vastus lateralis (VL), biceps femoris (BF) and semitendinosus (SEM) muscles of the participants were examined. Along with the muscle activation that occurred during the exercise, hamstring (BF+SEM)/quadriceps (VM+VL) ratio was also determined (H:Q). 1 Fahri Safa ÇINARLI, MSc Results: The lowest co-activation ratio (most balanced H:Q activation) was observed on stable Sevim Beyza ÖLMEZ, MSc, PT2 ground bridge exercise (5.83±4.04), and the largest co-activation ratio (hamstring dominant Seda NAMALDI, MSc, PT3 activation) was observed on stable ground plank exercise (8.84±6.60). No significant difference Ecem KARANFİL, MSc, PT3 was found between exercises at H:Q co-activation ratio (p>0.05). -

COSH Phase 2 Workouts
! (770)605-9786 City of Spring Hill Weeks 5-8 Workout Program Monday: Take care of your body. It’s the only one you have to live in. *If you wear a fitness tracker move 10,000 steps daily. That’s the equivalent of 5 miles* At the Office: The holidays are fast approaching! Don’t let this get in the way of your health. Drinking water throughout the day can help curb cravings and keep you feeling full longer. Commit to drinking one gallon per day and divide it up to drink 20 oz. every 1.5-2 hours. At the Gym/Home: *For distance measurement you can run .25 miles on a treadmill or think of running the length of 4 football fields* Other suggestions: map out a mile route with your car or download an app that tracks the distance you run! 1 Round 100 Walking Lunges (100 per each leg) 25 Squat Jumps 100 Bodyweight Goblet Squats (WEIGHTED SQUATS FOR ADVANCED) 50 Jumping Jacks (STAR JUMPS FOR ADVANCED) 100 Push Ups (Drop to knees when needed) 25 Burpees 100 Toe Touches (HOLD WEIGHT FOR ADVANCED) Run 1 Mile for time (ADVANCED- RUN 2 MILES AS FAST AS YOU CAN FOR TIME) (TRY TO BEAT TIME EACH WEEK) Exercise Tip: For a goblet squat, the feet are just slightly hip-width apart. Just like a regular squat, for a goblet squat you want to pretend you are sitting back in a chair and don’t let your knees pass over your front toes. Hold a weight or weighed object (gallon of water, textbook, etc.) in front of you chest or let weight hang between your legs. -

Sports Biomechanics an Electromyographic Comparison of a Modified Version of the Plank with a Long Lever and Posterior Tilt Vers
This article was downloaded by: [Auckland University of Technology] On: 05 August 2014, At: 19:42 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Sports Biomechanics Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rspb20 An electromyographic comparison of a modified version of the plank with a long lever and posterior tilt versus the traditional plank exercise Brad J. Schoenfelda, Bret Contrerasb, Gul Tiryaki-Sonmeza, Jeffrey M. Willardsonc & Fabio Fontanad a Department of Health Sciences, CUNY Lehman College, Bronx, NY, USA b Sport Performance Research Institute New Zealand, AUT University, Auckland, New Zealand c Kinesiology and Sports Studies Department, Eastern Illinois University, Charleston, IL, USA d School of Health, Physical Education, and Leisure Services, University of Northern Iowa, Cedar Falls, IA, USA Published online: 05 Aug 2014. To cite this article: Brad J. Schoenfeld, Bret Contreras, Gul Tiryaki-Sonmez, Jeffrey M. Willardson & Fabio Fontana (2014): An electromyographic comparison of a modified version of the plank with a long lever and posterior tilt versus the traditional plank exercise, Sports Biomechanics, DOI: 10.1080/14763141.2014.942355 To link to this article: http://dx.doi.org/10.1080/14763141.2014.942355 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. -

FOUNDATIONS of GROUP EXERCISE Produced in Cooperation with the American Council on Exercise Copyright© 2016 American Council on Exercise®
FOUNDATIONS OF GROUP EXERCISE Produced in Cooperation with the American Council on Exercise Copyright© 2016 American Council on Exercise® Printed in the United States of America. All rights reserved. Except for use in a review, the reproduction or utilization of this work in any form or by any electronic, mechanical, or other means, now known or hereafter invented, including xerography, photocopying, and recording, and in any information retrieval system, is forbidden without the written consent of the American Council on Exercise. ACE, ACE IFT, ACE Integrated Fitness Training, and American Council on Exercise are registered trademarks of the American Council on Exercise. Other product names used herein are for identification purpose only and may be trademarks of their respective companies. ABCD Distributed by: American Council on Exercise 4851 Paramount Dr. San Diego, CA 92123 (858) 576-6500 FAX (858) 576-6564 ACEfitness.org Author: American Council on Exercise Technical Editor: Jessica Matthews Project Editor: Daniel J. Green Art Director: Karen McGuire Production: Nancy Garcia C16-004 The YMCA and the American Council on Exercise (ACE) have teamed up to enhance community health. ACE is fueled by the passion of more than 58,000 health and wellness professionals worldwide, and the YMCA reaches more than 22 million members in 10,000 communities nationwide. The partnership created by our two organizations is a natural fit, and one that will allow us to more effectively address the health of our nation from multiple angles. ACE, a nonprofit that has helped to provide science-based education to professionals since 1985, will now offer YMCA Foundations of Group Exercise and YMCA Foundations of Strength and Conditioning courses for the YMCA certifications. -
Exercise: the Plank
2013 Exercise: The Plank Boot Camp & Military Fitness Institute 12/2/2013 Boot Camp & Military Exercise: The Plank Fitness Institute EXERCISE: THE PLANK CONTENTS Page 1.0 Introduction 2 2.0 History 2 3.0 What is the Plank? 2 4.0 The Muscles Behind the Movement 2 5.0 Why the Plank? 3 6.0 The Plank in the Military 3 7.0 Performing the Front Plank 3 8.0 Building-up to the Front Plank 3 9.0 Practical Tips 4 10.0 Variations of the Plank 4 11.0 Population Averages 6 12.0 Record Breakers 6 13.0 References 7 Through Deeds Not Words - 1 - (c) 2013 Boot Camp & Military Exercise: The Plank Fitness Institute 1.0 Introduction The plank is a simple, effective abdominal strengthening exercise that an individual can do almost anywhere. Exercisers will encounter the plank in a wide range of workouts, including outdoor fitness, fitness boot camps, military fitness, mixed martial arts, yoga and Pilates. Proper form is essential to preventing injury and maximising the exercise's benefits. You may think that the core muscles are only the ones in your stomach. In fact, the core is made up of all the muscles that connect the upper and lower body, including those of the stomach, lower back, hips and buttocks. These muscles are essential for supporting the spine, aiding good posture, and almost every movement. By strengthening the core muscles you will not only be on a fast track to a flatter stomach but will also improve the effectiveness of, almost, any exercise you do. -

A Comparison of the Plank and Perfect Plank Using Electromyography
A COMPARISON OF THE PLANK AND PERFECT PLANK USING ELECTROMYOGRAPHY MATTHEW R. IVERS Bachelor of Science in Exercise Science Capital University December 2015 Submitted in partial fulfillment of requirements for the degree MASTER OF EDUCATION IN EXERCISE SCIENCE At CLEVELAND STATE UNIVERSITY May 4th 2017 We hereby approve this thesis for Matthew R. Ivers Candidate for the Master of Education in Exercise Science degree for the Department of Health and Human Performance and CLEVELAND STATE UNIVERSITY’s College of Graduate Studies by ________________________________________________ Thesis Chairperson, Dr. Kenneth Sparks ________________________________________________ Department & Date ________________________________________________ Thesis Committee Member, Dr. Douglas Wadja ________________________________________________ Department & Date ________________________________________________ Thesis Committee Member, Dr. Emily Kullman ________________________________________________ Department & Date ________________________________________________ Associate Dean of Student Services, Dr. Kristine Still ________________________________________________ Department & Date Date of Defense: May 4th, 2017 ii AKNOWLEDGEMENT I would like to thank my professors for their support throughout this process. To Dr. Sparks, Dr. Wadja, and Dr. Kullman, thank you guys for the support and guidance throughout the process. I could not have done this without you. To Paul Synenkyj, thank you for the opportunity to collaborate on this project. I believe that this is -

Time Crunch Workout Guide
TIME CRUNCH WORKOUT GUIDE WWW.KAYJONES.COM We all know how important it is to move your body and get in regular exercise…. but life gets busy. Things pop up all of the time. It’s all too easy to move your workout to “tomorrow.” And in reality, that’s what most of us end up doing. FACT: Missing workouts and failing to follow through on commitments to yourself doesn’t feel very good. IT DOESN’T HAVE TO BE THAT WELCOME! WAY. THERE IS A SOLUTION. Thank you for downloading your copy Inside you’ll find results-driven workouts that will fit into even the busiest schedule … and for of the Time Crunch ALL fitness levels! Workout Guide! TIME CRUNCH WORKOUT GUIDE 1 We’ve kept the workouts simple, which means all you’ll need is a workout mat, the stopwatch/timer on your phone, a water bottle, and a towel. E These workouts might not take a lot of time, but they WILL help you achieve serious results. Not just in terms of helping you become stronger and fitter, but in building M your confidence, and grooving a fitness habit that can last a lifetime. O In fact, I created this ebook (in part) to help you uncover one of the most important keys to fitness: C CONSISTENCY! “NOT ENOUGH TIME” L IS NOT AN EXCUSE TO SKIP YOUR WORKOUTS. E A little intentional movement (aka exercise) every day will do more for your fitness and your results than an occasional workout marathon. W That’s not even mentioning all of the incredible health and energy benefits. -

Comparison of Physical Parameters of the Individuals Who Have
Journal of Education and Training Studies Vol. 6, No. 12; December 2018 ISSN 2324-805X E-ISSN 2324-8068 Published by Redfame Publishing URL: http://jets.redfame.com Comparison of Physical Parameters of the Individuals Who Have Received NASM-OPT Model & EMS Training in Combination With Traditional Fitness Training Applications Regularly as Personal Training (PT) for 20 Weeks Türker Bıyıklı Correspondence: Türker Bıyıklı, Nisantasi University Physical Education and Sports School, İstanbul, Turkey. Received: October 10, 2018 Accepted: October 23, 2018 Online Published: October 29, 2018 doi:10.11114/jets.v6i12.3673 URL: https://doi.org/10.11114/jets.v6i12.3673 Abstract In the study, it is aimed to determine whether there is any improvement in the physical performance development of the individuals, who have made exercise with OPT MODEL -EMS mix. and traditional PT models within the 20-week exercise program. In the study, pre-test, posttest, experimental screening by pattern methods are used. Study groups consist of 30 individuals, who are healthy and voluntary, continuing the fitness centers in Netherlands (OPT-EMS; n=30) and in Turkey (PT; n=30). After the data obtained is entered in computer environment; the arithmetic means (X), standard deviations (ss) of the research groups are taken and the Paired Samples t-test is applied for the differences between the pre-test and posttest. Significance level is examined at p<0.05 level. When the study findings are examined, statistically significant differences are observed in the push-up, squat, crunch, plank and Max Vo2 performance measurements of the participants in 20-week OPT-EMS group (p<0.05). -
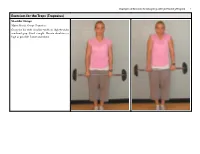
Exercises for the Traps (Trapezius) Shoulder Shrugs Major Muscle Group: Trapezius Grasp the Bar with Shoulder-Width Or Slightly Wider Overhand Grip
Examples of Exercises for Designing a Weight Training Program 1 Exercises for the Traps (Trapezius) Shoulder Shrugs Major Muscle Group: Trapezius Grasp the bar with shoulder-width or slightly wider overhand grip. Stand straight. Elevate shoulders as high as possible. Lower and repeat. Examples of Exercises for Designing a Weight Training Program 2 Lower Pulley Row to Neck Major Muscle Group: Trapezius Other Muscles Worked: Biceps, Middle back, Shoulders Sit at a seated row station and grab the ends of the rope using a palm-down grip. Sit with your knees slightly bent and your back straight. Do not lean back — your back should be almost completely ver- tical. Pull the rope back and up to neck height. Your elbows should be out, away from your sides. Return slowly to the starting position. Dumbbell Incline Shoulder Raise Major Muscle Group: Trapezius Sit down on an incline bench with the dumbbells resting on your lower thigh. Kick the weights to your shoulders and lean back. Position the dumbbells above your shoulders with your elbows extended. Raise your shoulders toward the dumbbells as high as possible. Lower shoulders to bench and repeat. Examples of Exercises for Designing a Weight Training Program 3 Upright Row Major Muscle Group: Trapezius Other Muscle Worked: Biceps, Shoulders Standing upright, grasp a barbell with your hands about shoulder-width apart. Let the bar hang straight down in front of you. Keep your body and wrists straight. Pull the bar straight up toward your chin, keeping it close to your body. Lower slowly to the starting position. Keep your back straight, making sure not to swing. -

Recommended Exercise Routine
Getting Physically Prepared for the Naval Academy Physical education is an important part of the program at the Naval Academy. To ensure that you are physically prepared for Plebe Summer, you are encouraged to start a program designed to help develop cardiovascular endurance and upper body and core strength. We have provided you with a sample program at the back of this pamphlet and a workout chart. Listed below are a few examples of some of the physical requirements of Plebe Summer to help you prepare for the types of activities in which you will be participating: 90 minutes, five days per week of strenuous physical calisthenics to increase cardio- respiratory fitness, muscular strength, and endurance, flexibility and confidence. Runs up to 4.5 miles at a 7-8-minute per mile pace, interval and sprint training. Obstacle and endurance courses that test balancing, leaping, climbing and team building skills. Hand to Hand training that incorporates martial arts, boxing, and wrestling. Climbing Wall training that involves upper body muscular strength and endurance, team building, and acclimatization to heights. It is imperative that you begin the recommended exercise routine, or one similar to it, NOW! Some common injuries historically seen during Plebe Summer, such as shin splints and minor foot, leg and back injuries related to being out of shape, can be prevented by your preparation beforehand. Upon arrival, a Physical Readiness Test (PRT) will be administered to determine whether a Midshipman meets the minimum standards of physical fitness for Plebe physical training. Failure to pass this test will result in assignment to a remedial program.