Specializations of Joints Between Vertebrae A. Atla
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Comparing the Injectate Spread and Nerve
Journal name: Journal of Pain Research Article Designation: Original Research Year: 2018 Volume: 11 Journal of Pain Research Dovepress Running head verso: Baek et al Running head recto: Ultrasound-guided GON block open access to scientific and medical research DOI: http://dx.doi.org/10.2147/JPR.S17269 Open Access Full Text Article ORIGINAL RESEARCH Comparing the injectate spread and nerve involvement between different injectate volumes for ultrasound-guided greater occipital nerve block at the C2 level: a cadaveric evaluation In Chan Baek1 Purpose: The spread patterns between different injectate volumes have not yet been investigated Kyungeun Park1 in ultrasound-guided greater occipital nerve (GON) block at the C2 level. This cadaveric study Tae Lim Kim1 was undertaken to compare the spread pattern and nerve involvements of different volumes of Jehoon O2 dye using this technique. Hun-Mu Yang2,* Materials and methods: After randomization, ultrasound-guided GON blocks with 1 or 5 mL dye solution were performed at the C2 level on the right or left side of five fresh cadavers. The Shin Hyung Kim1,* suboccipital regions were dissected, and nerve involvement was investigated. 1 Department of Anesthesiology and Results: Ten injections were successfully completed. In all cases of 5 mL dye, we observed the Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University deeply stained posterior neck muscles, including the suboccipital triangle space. The suboccipital College of Medicine, Seoul, Republic and third occipital nerves, in addition to GONs, were consistently stained when 5-mL dye was 2 of Korea; Department of Anatomy, used in all injections (100%). Although all GONs were successfully stained in the 1-mL dye Yonsei University College of Medicine, Seoul, Republic of Korea cases, three of five injections (60%) concomitantly stained the third occipital nerves. -

Shoulder Anatomy & Clinical Exam
MSK Ultrasound - Spine - Incheon Terminal Orthopedic Private Clinic Yong-Hyun, Yoon C,T-spine Basic Advanced • Medial branch block • C-spine transforaminal block • Facet joint block • Thoracic paravertebral block • C-spine intra-discal injection • Superficial cervical plexus block • Vagus nerve block • Greater occipital nerve block(GON) • Third occipital nerve block(TON) • Hydrodissection • Brachial plexus(1st rib level) • Suboccipital nerve • Stellate ganglion block(SGB) • C1, C2 nerve root, C2 nerve • Brachial plexus block(interscalene) • Recurrent laryngeal nerve • Serratus anterior plane • Cervical nerve root Cervical facet joint Anatomy Diagnosis Cervical facet joint injection C-arm Ultrasound Cervical medial branch Anatomy Nerve innervation • Medial branch • Same level facet joint • Inferior level facet joint • Facet joint • Dual nerve innervation Cervical medial branch C-arm Ultrasound Cervical nerve root Anatomy Diagnosis • Motor • Sensory • Dermatome, myotome, fasciatome Cervical nerve root block C-arm Ultrasound Stallete ganglion block Anatomy Injection Vagus nerve Anatomy Injection L,S-spine Basic Advanced • Medial branch block • Lumbar sympathetic block • Facet joint block • Lumbar plexus block • Superior, inferior hypogastric nerve block • Caudal block • Transverse abdominal plane(TAP) block • Sacral plexus block • Epidural block • Hydrodissection • Interlaminal • Pudendal nerve • Transforaminal injection • Genitofemoral nerve • Superior, inferior cluneal nerve • Rectus abdominal sheath • Erector spinae plane Lumbar facet -

A Case Report of an Enlarged Suboccipital Nerve with Cutaneous Branch
Open Access Case Report DOI: 10.7759/cureus.2933 A Case Report of an Enlarged Suboccipital Nerve with Cutaneous Branch Sasha Lake 1 , Joe Iwanaga 2 , Rod J. Oskouian 3 , Marios Loukas 4 , R. Shane Tubbs 5 1. Anatomical Studies, St. George's, St. George, GRD 2. Medical Education and Simulation, Seattle Science Foundation, Seattle, USA 3. Neurosurgery, Swedish Neuroscience Institute, Seattle, USA 4. Anatomical Sciences, St. George's University, St. George's, GRD 5. Neurosurgery, Seattle Science Foundation, Seattle, USA Corresponding author: Joe Iwanaga, [email protected] Abstract Variations of the suboccipital nerve are infrequently reported. This nerve derived from the C1 spinal nerve is usually a small branch that primarily innervates the short suboccipital muscles. During the routine dissection of the occipital region in an adult cadaver, a vastly enlarged left-sided suboccipital nerve was identified. The nerve innervated the short suboccipital muscles and overlying semispinalis capitis in normal fashion. However, it continued cranially to end in the overlying skin of the occiput. Although not normally thought to have a cutaneous branch, recalcitrant occipital neuralgia might be due to such a variant branch. Future studies are necessary to further elucidate this proposed pathomechanism. Categories: Neurology, Pathology Keywords: suboccipital nerve, c1 nerve, occiput cutaneous innervation, sensory suboccipital nerve Introduction The suboccipital nerve is the dorsal ramus of C1. This nerve is found between the skull and atlas and within the suboccipital triangle. Here, it is positioned between the posterior arch of the atlas and vertebral artery bordering the nerve inferiorly and superiorly, respectively [1]. The suboccipital nerve innervates the rectus capitis posterior major and minor, obliquus capitis superior, obliquus capitis inferior, and semispinalis capitis. -
Comparing the Injectate Spread and Nerve
Journal name: Journal of Pain Research Article Designation: Original Research Year: 2018 Volume: 11 Journal of Pain Research Dovepress Running head verso: Baek et al Running head recto: Ultrasound-guided GON block open access to scientific and medical research DOI: http://dx.doi.org/10.2147/JPR.S17269 Open Access Full Text Article ORIGINAL RESEARCH Comparing the injectate spread and nerve involvement between different injectate volumes for ultrasound-guided greater occipital nerve block at the C2 level: a cadaveric evaluation In Chan Baek1 Purpose: The spread patterns between different injectate volumes have not yet been investigated Kyungeun Park1 in ultrasound-guided greater occipital nerve (GON) block at the C2 level. This cadaveric study Tae Lim Kim1 was undertaken to compare the spread pattern and nerve involvements of different volumes of Jehoon O2 dye using this technique. Hun-Mu Yang2,* Materials and methods: After randomization, ultrasound-guided GON blocks with 1 or 5 mL dye solution were performed at the C2 level on the right or left side of five fresh cadavers. The Shin Hyung Kim1,* suboccipital regions were dissected, and nerve involvement was investigated. 1Department of Anesthesiology and For personal use only. Results: Ten injections were successfully completed. In all cases of 5 mL dye, we observed the Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University deeply stained posterior neck muscles, including the suboccipital triangle space. The suboccipital College of Medicine, Seoul, Republic and third occipital nerves, in addition to GONs, were consistently stained when 5-mL dye was 2 of Korea; Department of Anatomy, used in all injections (100%). -

SŁOWNIK ANATOMICZNY (ANGIELSKO–Łacinsłownik Anatomiczny (Angielsko-Łacińsko-Polski)´ SKO–POLSKI)
ANATOMY WORDS (ENGLISH–LATIN–POLISH) SŁOWNIK ANATOMICZNY (ANGIELSKO–ŁACINSłownik anatomiczny (angielsko-łacińsko-polski)´ SKO–POLSKI) English – Je˛zyk angielski Latin – Łacina Polish – Je˛zyk polski Arteries – Te˛tnice accessory obturator artery arteria obturatoria accessoria tętnica zasłonowa dodatkowa acetabular branch ramus acetabularis gałąź panewkowa anterior basal segmental artery arteria segmentalis basalis anterior pulmonis tętnica segmentowa podstawna przednia (dextri et sinistri) płuca (prawego i lewego) anterior cecal artery arteria caecalis anterior tętnica kątnicza przednia anterior cerebral artery arteria cerebri anterior tętnica przednia mózgu anterior choroidal artery arteria choroidea anterior tętnica naczyniówkowa przednia anterior ciliary arteries arteriae ciliares anteriores tętnice rzęskowe przednie anterior circumflex humeral artery arteria circumflexa humeri anterior tętnica okalająca ramię przednia anterior communicating artery arteria communicans anterior tętnica łącząca przednia anterior conjunctival artery arteria conjunctivalis anterior tętnica spojówkowa przednia anterior ethmoidal artery arteria ethmoidalis anterior tętnica sitowa przednia anterior inferior cerebellar artery arteria anterior inferior cerebelli tętnica dolna przednia móżdżku anterior interosseous artery arteria interossea anterior tętnica międzykostna przednia anterior labial branches of deep external rami labiales anteriores arteriae pudendae gałęzie wargowe przednie tętnicy sromowej pudendal artery externae profundae zewnętrznej głębokiej -

Bilateral Variation of the Suboccipital Region Musculature
S Journal of O p s e s n Acce Anatomy and Physiological Studies CASE REPORT Bilateral Variation of the Suboccipital Region Musculature AR Dickerson*, CL Fisher PhD Center for Anatomical Sciences, University of North Texas Health Science Center, Fort Worth, Texas, USA Abstract Dissection of the posterior cervical and suboccipital regions of an embalmed 81-year-old male cadaver revealed bilateral variations in the muscular anatomy, including two accessory muscles lying deep to the semispinalis capitis on each side, as well as a bilateral doubling of the rectus capitis posterior major muscle. These two sets of anatomical variations have little to no previous documentation in the literature. The accessory muscle bands were observed to have unique relationships with the greater occipital nerve on each side. This case report describes the findings in detail and examines their precedent in the literature. The suboccipital region has been implicated in the etiology of cervicogenic pain, headaches, and occipital neuralgia. Variations in the muscular anatomy have the potential to create structural interactions with vascular and neurologic structures in the area. Anatomic variations like those reported here should be considered in the diagnosis and treatment of pain and other conditions of the suboccipital region. Keywords: Anatomic Variation, Suboccipital, Accessory Muscle, Greater Occipital Nerve, Rectus capitis posterior major muscle Background leading us to believe that we had encountered accessory muscles that had been previously unreported. The muscles This case report describes variation of the musculature in the were delicate and located in a region often removed to expose suboccipital region observed during dissection of an embalmed the suboccipital region just beneath, so we postulate that the 81-year-old male cadaver. -

The Suboccipital Cavernous Sinus
The suboccipital cavernous sinus Kenan I. Arnautovic, M.D., Ossama Al-Mefty, M.D., T. Glenn Pait, M.D., Ali F. Krisht, M.D., and Muhammad M. Husain, M.D. Departments of Neurosurgery and Pathology, University of Arkansas for Medical Sciences, and Laboratory Service, Veterans Administration Medical Center, Little Rock, Arkansas The authors studied the microsurgical anatomy of the suboccipital region, concentrating on the third segment (V3) of the vertebral artery (VA), which extends from the transverse foramen of the axis to the dural penetration of the VA, paying particular attention to its loops, branches, supporting fibrous rings, adjacent nerves, and surrounding venous structures. Ten cadaver heads (20 sides) were fixed in formalin, their blood vessels were perfused with colored silicone rubber, and they were dissected under magnification. The authors subdivided the V3 into two parts, the horizontal (V3h) and the vertical (V3v), and studied the anatomical structures topographically, from the superficial to the deep tissues. In two additional specimens, serial histological sections were acquired through the V3 and its encircling elements to elucidate their cross-sectional anatomy. Measurements of surgically and clinically important features were obtained with the aid of an operating microscope. This study reveals an astonishing anatomical resemblance between the suboccipital complex and the cavernous sinus, as follows: venous cushioning; anatomical properties of the V3 and those of the petrouscavernous internal carotid artery (ICA), namely their loops, branches, supporting fibrous rings, and periarterial autonomic neural plexus; adjacent nerves; and skull base locations. Likewise, a review of the literature showed a related embryological development and functional and pathological features, as well as similar transitional patterns in the arterial walls of the V3 and the petrous-cavernous ICA. -

Ponticulus Posticus of Atlas Vertebrae: an Incidental Finding in Malaysian
BMJ Case Reports: first published as 10.1136/bcr-2017-220851 on 21 August 2017. Downloaded from Images in… Ponticulus posticus of atlas vertebrae: an incidental finding in Malaysian orthodontic patients Preethy Mary Donald,1 Sumanth Kumbargere Nagraj,1 Renjith George Pallivathukkal,2 Abdul Rashid Bin Ismail3 1Department of Oral Medicine DESCRIPTION surgical significance during treatment of atlan- and Oral Radiology, Faculty Ponticulus posticus is a normal anatomical variant to-axial stability for fixation of atlas. During inter- of Dentistry,, Melaka-Manipal of atlas vertebrae (C1) and resides in the posterior vention of cervical vertebrae, insertion of surgical Medical College, Melaka, arch of atlas in relation to vertebral artery. It is an screws can cause injury to vertebral artery and Malaysia incidental finding visualised from lateral cepha- suboccipital nerve if the surgeon is not aware of 2Department of Oral Pathology, the so-called bony anomaly. This in turn can cause Faculty of Dentistry, Melaka- lograms taken for routine orthodontic treatment Manipal Medical College, purpose. Ponticulus posticus in Latin means ‘little reduced blood circulation and headache in future. Melaka, Malaysia posterior bridge’. Other synonyms for ponticulus Expert surgeons in such cases have recommended 3Department of Community are arcuate foramen, kimerle anomaly, retroar- to use a modified screw trajectory to avoid piercing Dentistry, Faculty of Dentistry, ticular foramen and retocondylar foramen.1 An the vertebral artery and closely related structures. Melaka-Manipal Medical overall incidence of ponticulus posticus has been Casual movements like flexion and extension of College, Melaka, Malaysia reported to be 16.7%. Literature reveals a higher neck or continuous trauma in persons with arcuate incidence in females compared with males and this foramen can compress and restrict movement of Correspondence to anomaly was age independent.2 vertebral artery. -

Back Muscle Table Proximal Attachment Distal Attachment Muscle Innervation Main Actions Blood Supply Muscle Group (Origin) (Insertion)
Robert Frysztak, PhD. Structure of the Human Body Loyola University Chicago Stritch School of Medicine BACK MUSCLE TABLE PROXIMAL ATTACHMENT DISTAL ATTACHMENT MUSCLE INNERVATION MAIN ACTIONS BLOOD SUPPLY MUSCLE GROUP (ORIGIN) (INSERTION) Serratus posterior inferior Spinous processes of T11–L2 Inferior aspect of ribs 9–12 Ventral rami of lower thoracic nerves Depresses ribs Posterior intercostal arteries Intermediate back Ligamentum nuchae, spinous Serratus posterior superior Superior aspect of ribs 2–4 Ventral rami of upper thoracic nerves Elevates ribs Posterior intercostal arteries Intermediate back processes of C7–T3 Iliocostalis : angles of lower ribs, Cervical portions: occipital, deep cervical transverse processes cervical, and vertebral arteries Posterior sacrum, iliac crest, Longissimus: between tubercles and Thoracic portions: dorsal branches sacrospinous ligament, supraspinous angles of ribs, transverse processes Extends and laterally bends vertebral Erector spinae Dorsal rami of each region of posterior intercostal, subcostal, Sacrospinalis ligament, spinous processes of lower of thoracic and cervical vertebrae, column and head and lumbar arteries lumbar and sacral vertebrae mastoid process Sacral portions: dorsal branches of Spinalis: spinous processes of upper lateral sacral arteries thoracic and midcervical vertebrae Cervical portions: occipital, deep cervical, and vertebral arteries Interspinales (cervical, thoracic, Thoracic portions: dorsal branches Spinous process Adjacent spinous process Dorsal rami of spinal nerves -

DNM 皮膚神經調節技術工作坊dermo Neuro Modulating Workshop
DNM 皮膚神經調節技術工作坊 Dermo Neuro Modulating Workshop 【課程簡介】 Diane Jacobs 治療師於 2005 年提出『DermoNeuroModulation』(DNM:皮膚神經調節 技術)這套將神經理論與實作並用的治療方法,多年來,Diane Jacobs 透過對於皮膚、神經解剖 學的持續鑽研,於 2010 年向加拿大聖約翰大學的 CPA 大會發表了該方法的研究結果。 皮膚神經調節(DNM)是一種處理人體神經組織的徒手手法,透過這項特殊的手法進行神經系 統的處理,以針對疼痛和動作輸出方面等症狀做全面性的調節。 Diane Jacobs 開始於 2007 年將這個結合理論與徒手治療的方法進行教學與推廣,並且撰寫 了一本治療手冊《Dermo Neuro Modulating: Manual Treatment for Peripheral Nerves and Especially Cutaneous Nerves》,將 DNM 方法指導給全世界的物理治療師與按摩治療師,包含 加拿大,美國,歐洲及巴西……等地,教學與治療方式廣受好評。 2018 年,本協會特別邀請皮膚神經調節技術(DNM)創始人 Diane Jacobs 來台演講,Diane Jacobs 是一位於加拿大執業多年,擁有極豐富講課經驗的物理治療師。本次為台灣學員帶來這個 為期三天半的小型實作工作坊,本工作坊以見微知著的方式,首先以一個晚上的基礎理論課程介 紹 DNM 的學理背景,帶領學員為後續三日的課程做好準備,並且在為期三天的實作課程當中, 一一爬梳各部位的神經解剖,並由此做為切入點,進一步將神經解剖知識、疼痛控制理論、體感 覺系統相互串聯,透過大量實際操作各部位的手法,與臨床治療的運用相結合。 本工作坊將深入探討神經解剖、體感覺系統(somatosensory system)及疼痛科學與臨床實 作結合的重要課題。以小型精緻的實作工作坊方式,引領學員經由大量的徒手治療手法練習,理 解如何在臨床上透過對於腦部、皮膚、脊髓、神經動力學、疼痛和傷害感受的差異性、以及非特 定效應(non-specific effects)與疼痛抑制調節(descending modulation)等疼痛科學的知識,來 重新建立臨床治療上的策略與手法。 臺灣應用復健協會特別邀請 Diane Jacobs 來臺 開授此精緻的小班制實作工作坊 ,讓臺灣的專業 人士不需出國,也能學習這項獨特的知識技術, 與國際接軌! 本課程講師亦提供上課資料供學員以隨身 碟存取,期望每位與會學員都能有最佳的 學習效果! 【上課時間與地點】 2018 年 4 月 27 日(五):晚間 3 小時基礎理論課程 2018 年 4 月 28 日(六)、4 月 30 日(一)、5 月 1 日(二):徒手實際操作課程 台北市青少年發展處 六樓大研討室 【學分認證】 台灣復健醫學會 繼續教育學分積分申請中 中華民國物理治療師公會全國聯合會 繼續教育學分積分申請中 中華民國職能治療師公會全國聯合會 繼續教育學分積分申請中 台灣運動傷害防護學會 繼續教育時數申請中 ※ 以上各專業實際積分點數將依各認證單位回函即時更新於課程官網上。 【課程表】 Date Time Course DAY 0: 3 小時基礎理論課程 4/27 (Fri.) 6:00 pm - 9:00 pm The three hour lecture covers the essential topics, it is prerequisite to the practical lab workshop. DAY1: DORSAL RAMI OF NECK, -
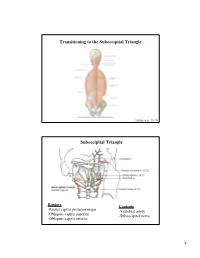
Dry Lab-Weyrich
Transitioning to the Suboccipital Triangle Syllabus p. 14-15 Suboccipital Triangle Borders Contents -Rectus capitis posterior major -Vertebral artery -Obliquus capitis superior -Suboccipital nerve -Obliquus capitis inferior 1 Innervation of the Suboccipital Region Suboccipital (C1) – innervates suboccipital muscles Greater occipital (C2) – supplies posterior scalp C3 – supplies small area of lower scalp Blood Supply to the Suboccipital Region Occipital artery 2 A 29 year old man suffers from a stroke. A dissecting vertebral artery contributed to his stroke. This may in part be due to the course of the vertebral artery as it approaches the suboccipital triangle, which is bordered by the following muscles: 100% A. Obliquus capitis superior, Obliquus capitis inferior, rectus capitis minor B. Obliquus capitis superior, rectus capitis minor, rectus capitis major C. Obliquus capitis superior, Obliquus capitis inferior, rectus capitis major D. Obliquus capitis superior, semispinalis cervicus, rectus capitis major 0% 0% 0% 0% E. Obliquus capitis inferior, rectus capitis minor, rectus capitis major A. Obliquus B. capitis Obliquus s... Obliquus capitis s... capitis Obliquus supe... capitis Obliquus supe... capitis inferio.. Osteology • Back -Gray’s pp. 26-47 -Gray’s dissector, pp. 3-9 3 Osteologic Landmarks (Back) Scapula (posterior) 4 The Vertebral Column Normal Curvatures of the Vertebral Column 5 Abnormal Curvatures of the Vertebral Column A 42 year old male goes running for one hour and subsequently complains of lower back pain and disoriented equilibrium. After a superficial examination of the back, you conclude that the runner is suffering from one of the following: 100% A. Lordosis B. Scoliosis C. Right side winged scapula D. -

Landmarks for the Identification of the Cutaneous Nerves of the Occiput
Clinical Anatomy 20:235–238 (2007) ORIGINAL COMMUNICATION Landmarks for the Identification of the Cutaneous Nerves of the Occiput and Nuchal Regions R. SHANE TUBBS,* E. GEORGE SALTER, JOHN C. WELLONS III, JEFFREY P. BLOUNT, AND W. JERRY OAKES Pediatric Neurosurgery, Children’s Hospital, Birmingham, Alabama Although surgical procedures are often performed over the posterior head and neck, surgical landmarks for avoiding the cutaneous nerves in this region are surprisingly lacking in the literature. Twelve adult cadaveric specimens under- went dissection of the cutaneous nerves overlying the posterior head and neck, and mensuration was made between these structures and easily identifi- able surrounding bony landmarks. All specimens were found to have a third occipital nerve (TON), lesser occipital nerve (LON), and greater occipital nerve (GON), and we found that the TON was, on average, 3 mm lateral to the external occipital protuberance (EOP). Small branches were found to cross the midline and communicate with the contralateral TON inferior to the EOP in the majority of sides. The mean diameter of the main TON trunk was 1.3 mm. This trunk became subcutaneous at a mean of 6 cm inferior to the EOP. The GON was found to lie at a mean distance of 4 cm lateral to the EOP. On all but three sides, a small medial branch was found that ran medially from the GON to the TON *1 cm superior to a horizontal line drawn through the EOP. The GON was found to pierce the semispinalis capitis muscle on average 2 cm superior to the intermastoid line. The mean diameter of the GON was 3.5 mm.