Heart Rate Variability As an Independent Predictor for 8-Year
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Heart Rate Variability
Heart Rate Variability Jason Moore Elite HRV EliteHRV.com EliteHRV.com EliteHRV.com EliteHRV.com EliteHRV.com Start with the big picture. With the big picture in mind, drill into the details. EliteHRV.com The Bigger Picture of Human Health • Your body and mind (and symbiotic organisms) versus the world • The world is stressful EliteHRV.com Environmental Societal Mental Digestive STRESS Physical Structural Social *Not an exhaustive list Emotional EliteHRV.com The Bigger Picture of Human Health • Adaptive biological organisms • Health issues occur when: • Acute stress exceeds chronic adaptation • or • A strong/chronic mismatch between our genes and our environment EliteHRV.com Why Heart Rate Variability (HRV)? HRV can non-invasively measure the body’s response to stress, and with enough data, its capacity to tolerate stress. • Systemic, big picture metric • Was expensive, now cheap and accessible • Short, frequent measurements open new doors EliteHRV.com HRV 101 • Temporal variation in heart beats • Requires high degree of accuracy • Many algorithms/calculations EliteHRV.com HRV 101 – Autonomic Nervous System Sympathetic Parasympathetic Nervous System (SNS) Nervous System (PSNS) ● Controls stimulation of ● Controls stimulation of “fight-or-flight” stress “rest-and-digest” activities response essential for recovery ● Needed for short term ● Needed for long term survival survival ● Associated with stress EliteHRV.com EliteHRV.com HRV In The Research • Decades of research • 20,000+ studies in PubMed • Increasing rapidly • Still a lot to learn EliteHRV.com In 778 athletes, HRV indices of ANS activity show strong correlation with selection for Olympic games for the Italian team Can the use of a single integrated unitary autonomic index provide early clues for eventual eligibility for olympic games? Daniela Lucini, Roberto Sala, Antonio Spataro, Mara Malacarne, Manuela Benzi, Stefano Tamorri, Massimo Pagani https://link.springer.com/article/10.1007/s00421-018-3822-2 EliteHRV.com HRV indexes worry in individuals spanning the non- clinical to clinical spectrum. -
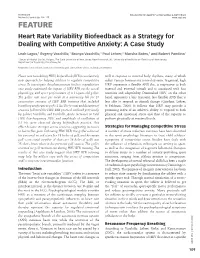
FEATURE Heart Rate Variability Biofeedback As a Strategy for Dealing with Competitive Anxiety: a Case Study
Biofeedback ©Association for Applied Psychophysiology & Biofeedback Volume 36, Issue 3, pp. 109–115 www.aapb.org FEATURE Heart Rate Variability Biofeedback as a Strategy for Dealing with Competitive Anxiety: A Case Study Leah Lagos,1 Evgeny Vaschillo,1 Bronya Vaschillo,1 Paul Lehrer,2 Marsha Bates,1 and Robert Pandina1 1 Center of Alcohol Studies, Rutgers, The State University of New Jersey, New Brunswick, NJ; 2University of Medicine and Dentistry of New Jersey, Department of Psychiatry, Piscataway, NJ Keywords: biofeedback, heart rate variability, golf, competitive stress, optimal performance Heart rate variability (HRV) biofeedback (BFB) is a relatively well in response to internal body rhythms, many of which new approach for helping athletes to regulate competitive reflect various homeostatic control systems. In general, high stress. To investigate this phenomenon further, a qualitative HRV represents a flexible ANS that is responsive to both case study examined the impact of HRV BFB on the mood, internal and external stimuli and is associated with fast physiology, and sport performance of a 14-year-old golfer. reactions and adaptability. Diminished HRV, on the other The golfer met once per week at a university lab for 10 hand, represents a less transient, less flexible ANS that is consecutive sessions of HRV BFB training that included less able to respond to stimuli change (Giardino, Lehrer, breathing at a frequency of 0.1 Hz. The format and duration of & Feldman, 2000). It follows that HRV may provide a sessions followed the HRV BFB protocol outlined previously promising index of an athlete’s ability to respond to both by Lehrer, Vaschillo, and Vaschillo. -

Heart Rate Variability (HRV) Biofeedback: a New Training Approach for Operator's Performance Enhancement
A Service of Leibniz-Informationszentrum econstor Wirtschaft Leibniz Information Centre Make Your Publications Visible. zbw for Economics Sutarto, Auditya Purwandini; Wahab, Muhammad Nubli Abdul; Nora Mat Zin Article Heart Rate Variability (HRV) biofeedback: A new training approach for operator's performance enhancement Journal of Industrial Engineering and Management (JIEM) Provided in Cooperation with: The School of Industrial, Aerospace and Audiovisual Engineering of Terrassa (ESEIAAT), Universitat Politècnica de Catalunya (UPC) Suggested Citation: Sutarto, Auditya Purwandini; Wahab, Muhammad Nubli Abdul; Nora Mat Zin (2010) : Heart Rate Variability (HRV) biofeedback: A new training approach for operator's performance enhancement, Journal of Industrial Engineering and Management (JIEM), ISSN 2013-0953, OmniaScience, Barcelona, Vol. 3, Iss. 1, pp. 176-198, http://dx.doi.org/10.3926/jiem.v3n1.p176-198 This Version is available at: http://hdl.handle.net/10419/188419 Standard-Nutzungsbedingungen: Terms of use: Die Dokumente auf EconStor dürfen zu eigenen wissenschaftlichen Documents in EconStor may be saved and copied for your Zwecken und zum Privatgebrauch gespeichert und kopiert werden. personal and scholarly purposes. Sie dürfen die Dokumente nicht für öffentliche oder kommerzielle You are not to copy documents for public or commercial Zwecke vervielfältigen, öffentlich ausstellen, öffentlich zugänglich purposes, to exhibit the documents publicly, to make them machen, vertreiben oder anderweitig nutzen. publicly available on the internet, or to distribute or otherwise use the documents in public. Sofern die Verfasser die Dokumente unter Open-Content-Lizenzen (insbesondere CC-Lizenzen) zur Verfügung gestellt haben sollten, If the documents have been made available under an Open gelten abweichend von diesen Nutzungsbedingungen die in der dort Content Licence (especially Creative Commons Licences), you genannten Lizenz gewährten Nutzungsrechte. -

Heart Rate Variability in Patients with Cirrhosis: a Systematic Review and Meta-Analysis
medRxiv preprint doi: https://doi.org/10.1101/2021.01.20.21249506; this version posted January 20, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Heart Rate Variability in Patients with Cirrhosis: A Systematic Review and Meta-analysis Tope Oyelade1* ([email protected]), Gabriele Canciani2, Gabriele Carbone2, Jaber Alqahtani3,4, Kevin Moore1, Ali R. Mani1. 1. Institute for Liver and Digestive Health, Division of Medicine, University College London, London NW3 2PF, UK. 2. School of Medicine, La Sapienza University, Rome 00185, Italy. 3. Respiratory Medicine, Division of Medicine, University College London, London NW3 2PF, UK. 4. Department of Respiratory Care, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia. * Corresponding Author NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice. medRxiv preprint doi: https://doi.org/10.1101/2021.01.20.21249506; this version posted January 20, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Abstract: Background: Cirrhosis is associated with abnormal autonomic function and regulation of cardiac rhythm. Measurement of heart rate variability (HRV) provides an accurate and non-invasive measurement of autonomic function as well as liver disease severity currently calculated using the MELD, UKELD, or ChildPugh scores. -
Heart Rate Variability Analysis System
Heart Rate Variability Analysis System Clinical Information VERSION 3.O. SA - 3000P Clinical Manual Clinical 3000P CONTENTS 1. ABOUT SA-3000P------------------------------------------------------------------------------------4 VER.3.0. 2. HRV, ITS BACKGROUND INFORMATION 2.1. HRV, ITS DEFINITION----------------------------------------------------------------------------------6 2.2. GENERATION OF HRV--------------------------------------------------------------------------------7 2.3. HISTORY OF HRV---------------------------------------------------------------------------------------9 2.4. ABOUT THE TASK FORCE--------------------------------------------------------------------------10 2.5. STRESS AND AUTOMNOMIC NERVOUS SYSTEM------------------------------------------11 2.6. THE MEANING OF DEPRESSED HRV-----------------------------------------------------------12 3. METHODOLOGY AND TERMINOLOGY OF HRV ANALYSIS 3.1. METHODOGOLY----------------------------------------------------------------------------------------14 3.2. TERMINOLOGY-----------------------------------------------------------------------------------------16 3.2.1. Time Domain parameters---------------------------------------------------------------------------16 3.2.1.1 SDNN 2 3.2.1.2 SDNN Index 3.2.1.3. RMS-SD 3.2.2. Frequency Domain Parameters----------------------------------------------------------------17 3.2.2.1. Total Power (TP) 3.2.2.2. Very Low Frequency (VLF) 3.2.2.3. Low Frequency (LF) 3.2.2.4. High Frequency (HF) 3.2.2.5. LF/HF Ratio 3.2.2.6. Normalized Low Frequency -
How to Stimulate Your Vagus Nerve for Better Mental Health Adapted from - January 21, 2017 Jordan Fallis
How to Stimulate Your Vagus Nerve for Better Mental Health Adapted from - January 21, 2017 Jordan Fallis “By developing an understanding of the workings of your vagus nerve, you may find it possible to work with your nervous system rather than feel trapped when it works against you.” — Dr. Arielle Schwartz, Clinical Psychologist Stimulating my vagus nerve has played a key role in the management of my mental health over the years. What exactly is the vagus nerve? The vagus nerve is the longest nerve in your body. It connects your brain to many important organs throughout the body, including the gut (intestines, stomach), heart and lungs. In fact, the word "vagus" means “wanderer” in Latin, which accurately represents how the nerve wanders all over the body and reaches various organs. The vagus nerve is also a key part of your parasympathetic “rest and digest” nervous system. It influences your breathing, digestive function and heart rate, all of which can have a huge impact on your mental health. But what you really need to pay special attention to is the "tone" of your vagus nerve. Vagal tone is an internal biological process that represents the activity of the vagus nerve. Increasing your vagal tone activates the parasympathetic nervous system, and having higher vagal tone means that your body can relax faster after stress. In 2010, researchers discovered a positive feedback loop between high vagal tone, positive emotions, and good physical health. In other words, the more you increase your vagal tone, the more your physical and mental health will improve, and vice versa (5). -

Heart Rate Variability and Decision-Making: Autonomic Responses in Making Decisions
brain sciences Article Heart Rate Variability and Decision-Making: Autonomic Responses in Making Decisions Giuseppe Forte 1,* , Matteo Morelli 1 and Maria Casagrande 2,* 1 Department of Psychology, Sapienza University of Rome, 00185 Rome, Italy; [email protected] 2 Department of Dynamic, Clinical Psychology and Health Studies, Sapienza University of Rome, 00185 Rome, Italy * Correspondence: [email protected] (G.F.); [email protected] (M.C.) Abstract: Decision-making is one of the most crucial cognitive processes in daily life. An adaptable, rapid, and flexible decision requires integration between brain and body. Heart rate variability (HRV) indexes this brain–body connection and appears to be related to cognitive performance. However, its relationship with decision-making is poorly analyzed. This study investigates the relationship between HRV and the decision-making process, assessed through the Iowa Gambling Task (IGT). One hundred and thirty healthy university students (mean age = 23.35 ± 2.50) participated in the study. According to IGT performance, they were divided into high decision-makers (n = 79) and low decision-makers (n = 51). Heart rate variability was measured in the resting, reactivity (i.e., during IGT), and recovery phases. Higher vagally mediated HRV (vmHRV; indexed in frequency domain measures) was evidenced in good decision-makers in the resting, reactivity, and recovery phases. During the task, a higher vagal modulation after a first evaluation was highlighted in good decision-makers. In conclusion, HRV proves to be a valid index of inhibitory circuit functioning in the prefrontal cortex. The relationship with cognitive functions was also confirmed, considering the ability to inhibit disadvantageous responses and make better decisions. -

Heart Rate Variability in Cirrhosis Liver
HEART RATE VARIABILITY IN CIRRHOSIS LIVER Dissertation Submitted to THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY in partial fulfillment of the regulations for the award of the degree of D.M (GASTROENTEROLOGY) BRANCH – IV DEPARTMENT OF MEDICAL GASTROENTEROLOGY GOVT. STANLEY MEDICAL COLLEGE & HOSPITAL THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI, INDIA. AUGUST 2009 CERTIFICATE This is to certify that the dissertation entitled “HEART RATE VARIABILITY IN CIRRHOSIS LIVER” is the bonafide original work of Dr. S. ARAVINDH in partial fulfillment of the requirements for D.M (GASTROENTEROLOGY) BRANCH – IV Examination of the Tamilnadu Dr. M.G.R. Medical University to be held in August 2009. The period of study was from June 2007 to December 2008. Dr. J. MOHANASUNDARAM, M.D., Ph.D, DNB, Prof. V. JAYANTHI , M.D.,D.M, DEAN Professor & Head Govt. Stanley Medical College & Hospital, Department of Medical Gastroenterology Chennai-600 001. Govt. Stanley Medical College Chennai-600 001. ACKNOWLEDGEMENT I express my profound gratitude to Dr. J. MOHANASUNDARAM, M.D., Ph.D, DNB, Dean of Government Stanley Medical College and Hospital, Chennai–600001 for permitting me to use all the needed resources for this dissertation work. I sincerely express my grateful thanks to Prof V. JAYANTHI, M.D., D.M., Professor and Head, Department of Medical Gastroenterology, Stanley Medical College for her unstinted support and advice rendered throughout my study. I thank her for being a constant source of encouragement, inspiration, not only in this study but in all my professional endeavors. I express my gratitude to Prof. Balasubramaniam, M.D., Head of Dept, and Assistant Professor, Dr. -

The Prognostic Correlation of Heart Rate Variability at Diagnosis with Survival of Patients with Hepatocellular Carcinoma
diagnostics Article The Prognostic Correlation of Heart Rate Variability at Diagnosis with Survival of Patients with Hepatocellular Carcinoma 1,† 2, 1,† 1 Ana-Maria Ciurea , Dan Ionut, Gheonea *, Michael Schenker , Alina Maria Mehedint, eanu , Georgică Costinel Târtea 3,4,* and Cristin Constantin Vere 2 1 Department of Oncology, University of Medicine and Pharmacy of Craiova, 200349 Craiova, Romania; [email protected] (A.-M.C.); [email protected] (M.S.); [email protected] (A.M.M.) 2 Department of Gastroenterology, University of Medicine and Pharmacy of Craiova, 200349 Craiova, Romania; [email protected] 3 Department of Physiology, University of Medicine and Pharmacy of Craiova, 200349 Craiova, Romania 4 Department of Cardiology, Emergency County Hospital of Craiova, 200642 Craiova, Romania * Correspondence: [email protected] (D.I.G.); [email protected] (G.C.T.); Tel.: +4-0351-443-500 (D.I.G.) † These authors contributed equally to this work. Abstract: Background: Heart rate variability (HRV) indices have been shown to be associated with prognosis in various types of cancer. This study aims to assess the ability of these indices to predict survival in hepatocellular carcinoma (HCC) patients after diagnosis. Methods: We retrospectively collected data from 231 patients diagnosed with HCC between January 2014 and March 2018. The baseline clinical-pathological variables and HRV indices (extracted from Holter electrocardiogram recordings) were analyzed. Results: Univariate and multivariate analyses were performed to identify the predictive value of the above factors for overall survival (OS). The univariate analysis revealed Citation: Ciurea, A.-M.; Gheonea, that an age > 60 years, hepatitis C, portal vein involvement (thrombosis), a tumor size > 5 cm, D.I.; Schenker, M.; Mehedint,eanu, A.M.; Târtea, G.C.; Vere, C.C. -

Signal Processing Methods for Heart Rate Variability
Signal Processing Methods for Heart Rate Variability Gari D. Clifford St. Cross College Supervised by Prof. L. Tarassenko Michaelmas Term, 2002 This thesis is submitted to the Department of Engineering Science, University of Oxford, in fulfilment of the requirements for the degree of Doctor of Philosophy. This thesis is entirely my own work, and except where otherwise stated, describes my own research. Signal Processing Methods For Heart Rate Variability Analysis Gari D. Clifford St Cross College Doctor of Philosophy Michaelmas term 2002 Heart rate variability (HRV), the changes in the beat-to-beat heart rate calculated from the electrocar- diogram (ECG), is a key indicator of an individual’s cardiovascular condition. Assessment of HRV has been shown to aid clinical diagnosis and intervention strategies. However, the variety of HRV estima- tion methods and contradictory reports in this field indicate that there is a need for a more rigorous investigation of these methods as aids to clinical evaluation. This thesis investigates the development of appropriate HRV signal processing techniques in the context of pilot studies in two fields of potential application, sleep and head-up tilting (HUT). A novel method for characterising normality in the ECG using both timing information and morpho- logical characteristics is presented. A neural network, used to learn the beat-to-beat variations in ECG waveform morphology, is shown to provide a highly sensitive technique for identifying normal beats. Fast Fourier Transform (FFT) based frequency-domain HRV techniques, which require re-sampling of the inherently unevenly sampled heart beat time-series (RR tachogram) to produce an evenly sampled time series, are then explored using a new method for producing an artificial RR tachogram. -

Utilizing Heart Rate Variability As an Indicator of Post-Traumatic Stress Disorder (PTSD)
Proceedings of the 2017 International Symposium on Human Factors and Ergonomics in Health Care 249 Utilizing Heart Rate Variability as an Indicator of Post-Traumatic Stress Disorder (PTSD) Carolina Rodriguez-Paras, Farzan Sasangohar Texas A&M University, College Station, Texas, USA Heart rate variability (HRV) is the natural beat to beat variations that occur within subsequent heart beats, modulated by the autonomic nervous system (ANS), which is composed of the parasympathetic and sympathetic nervous systems (Acharya, Joseph, Kannathal, Lim, & Suri, 2006). The sympathetic nervous system (“fight or flight” response), occurs due to stress, heart disease, or exercise. The parasympathetic nervous system (“rest or digest” response), is responsible for the internal organs and their functions. Decreased activity in parasympathetic, or increased activity in the sympathetic nervous system results in cardiac acceleration, with the opposite being true for cardiac deceleration. These changes are reflected in the normal R-R (peak-to-peak) intervals occurring in the QRS complex which represents the deflections in electrocardiogram (ECG) model of heart beat (Acharya et al., 2006). Several methods exist to analyze HRV, dependent on the length of the time interval (short or long), and of the type of analysis (e.g. time domain, frequency domain, or geometric methods) (Task Force of the European Society of Cardiology, 1996). Changes in the autonomic nervous system are reflected in the frequency domain analysis, which indicate cardiovascular functionality and autonomic regulation. Low frequency (0.04 – 0.15 Hz) corresponds to sympathetic activity, while high frequency (0.15 – 0.4 Hz) is associated with parasympathetic activity (Acharya et al., 2006). -

Relationship of Heart Rate Variability to Parasympathetic Effect
Relationship of Heart Rate Variability to Parasympathetic Effect Jeffrey J. Goldberger, MD; Sridevi Challapalli, MD; Roderick Tung, MD; Michele A. Parker, MS; Alan H. Kadish, MD Background—Baroreflex-mediated parasympathetic stimulation has variable effects on heart rate variability (HRV). We postulated that a quadratic function would describe the relationship between HRV and parasympathetic effect better than a linear function. Methods and Results—Twenty-nine normal volunteers (15 women; mean age 39Ϯ12 years) were studied after -adrenergic blockade with intravenous propranolol. Five-minute ECG recordings were made during graded infusions of phenylephrine and nitroprusside to achieve baroreflex-mediated increases and decreases in parasympathetic effect, respectively. Time- and frequency-domain measures of HRV were calculated from the R-R interval tachograms. The R-R interval and the vagal-sympathetic effect (VSEϭR-R interval/intrinsic R-R interval) were used as indices of parasympathetic effect. The data were fit to both quadratic and linear models. In each case, the quadratic model (with a negative coefficient for the squared term) was superior to the linear model. There was some evidence that age influenced the responsiveness of the HRV parameters with changing parasympathetic effect, although the regression analysis was significant only in the models for MSSD (PϽ0.03) and pNN50 (PϽ0.001). Conclusions—The relationship between HRV and parasympathetic effect is best described by a function in which there is an ascending limb where HRV increases as parasympathetic effect increases until it reaches a plateau level; HRV then decreases as parasympathetic effect increases. Because there is marked interindividual variation in this relationship, differences in HRV between individuals may reflect differences in this relationship and/or differences in autonomic effects.