280156-Eng.Pdf (1.803Mb)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Rcdf Projects in Yumbe District, Uganda
Rural Communications Development Fund (RCDF) RCDF PROJECTS IN YUMBE DISTRICT, UGANDA MAP O F YU M B E SH O W IN G S UB C O U NT IE S N Midigo Kei Apo R omo gi Yum be TC Kuru D rajani Od ravu 3 0 3 6 Km s UCC Support through the RCDF Programme Uganda Communications Commission Plot 42 -44, Spring road, Bugolobi P.O. Box 7376 Kampala, Uganda Tel: + 256 414 339000/ 312 339000 Fax: + 256 414 348832 E-mail: [email protected] Website: www.ucc.co.ug 1 Table of Contents 1- Foreword……………………………………………………………….……….………..…..…....….…3 2- Background…………………………………….………………………..…………..….….……………4 3- Introduction………………….……………………………………..…….…………….….…………...4 4- Project profiles……………………………………………………………………….…..…….……...5 5- Stakeholders’ responsibilities………………………………………………….….…........…12 6- Contacts………………..…………………………………………….…………………..…….……….13 List of tables and maps 1- Table showing number of RCDF projects in Yumbe district………….………..….5 2- Map of Uganda showing Yumbe district………..………………….………...………….14 10- Map of Yumbe district showing sub counties………..……………………………….15 11- Table showing the population of Yumbe district by sub counties……..…...15 12- List of RCDF Projects in Yumbe district…………………………………….………...…16 Abbreviations/Acronyms UCC Uganda Communications Commission RCDF Rural Communications Development Fund USF Universal Service Fund MCT Multipurpose Community Tele-centre PPDA Public Procurement and Disposal Act of 2003 POP Internet Points of Presence ICT Information and Communications Technology UA Universal Access MoES Ministry of Education and Sports MoH Ministry of Health DHO District Health Officer CAO Chief Administrative Officer RDC Resident District Commissioner 2 1. Foreword ICTs are a key factor for socio-economic development. It is therefore vital that ICTs are made accessible to all people so as to make those people have an opportunity to contribute and benefit from the socio-economic development that ICTs create. -

Education and Fragility in Northern Uganda CARE
American Institutes for Research Academy for Educational Development Aga Khan Foundation Education and Fragility in Northern Uganda CARE Discovery Channel Global Education Fund Education Development Center Howard University International Reading Association The Joseph P. Kennedy, Jr. Foundation Produced by: Juárez and Associates, Inc. American Institutes for Research under the EQUIP1 LWA Michigan State University By: Meredith McCormac, Principal Author Judy A. Benjamin, PhD, Contributor Sesame Workshop October 2008 Save the Children Federation, USA University of Pittsburgh U.S. Agency for International Development World Education Cooperative Agreement No. GDG-A-00-03-00006-00 Districts Affected by Conflict Source: Allen and Schomerus (2006), originally obtained from UN OCHA Education and Fragility in Northern Uganda TABLE OF CONTENTS Acknowledgements ............................................................................................................ 1 Executive Summary ...........................................................................................................2 1.0 Introduction ..................................................................................................................3 2.0 The Conflict and Root Causes of Fragility in Northern Uganda .................................4 2.1 Root Causes ............................................................................................................4 2.2 Historical Background ............................................................................................4 -

World Bank Document
Public Disclosure Authorized ENVIRONMENTAL AND SOCIAL MANAGEMENT AND MONITORING PLAN Public Disclosure Authorized Public Disclosure Authorized Ministry of Energy and Mineral Development Rural Electrification Agency ENERGY FOR RURAL TRANSFORMATION PHASE III GRID INTENSIFICATION SCHEMES PACKAGED UNDER WEST NILE, NORTH NORTH WEST, AND NORTHERN SERVICE TERRITORIES Public Disclosure Authorized JUNE, 2019 i LIST OF ABBREVIATIONS AND ACRONYMS CDO Community Development Officer CFP Chance Finds Procedure DEO District Environment Officer ESMP Environmental and Social Management and Monitoring Plan ESMF Environmental Social Management Framework ERT III Energy for Rural Transformation (Phase 3) EHS Environmental Health and Safety EIA Environmental Impact Assessment ESMMP Environmental and Social Mitigation and Management Plan GPS Global Positioning System GRM Grievance Redress Mechanism MEMD Ministry of Energy and Mineral Development NEMA National Environment Management Authority OPD Out Patient Department OSH Occupational Safety and Health PCR Physical Cultural Resources PCU Project Coordination Unit PPE Personal Protective Equipment REA Rural Electrification Agency RoW Right of Way UEDCL Uganda Electricity Distribution Company Limited WENRECO West Nile Rural Electrification Company ii TABLE OF CONTENTS LIST OF ABBREVIATIONS AND ACRONYMS ......................................................... ii TABLE OF CONTENTS ........................................................................................ iii EXECUTIVE SUMMARY ....................................................................................... -
Usaid's Malaria Action Program for Districts
USAID’S MALARIA ACTION PROGRAM FOR DISTRICTS GENDER ANALYSIS MAY 2017 Contract No.: AID-617-C-160001 June 2017 USAID’s Malaria Action Program for Districts Gender Analysis i USAID’S MALARIA ACTION PROGRAM FOR DISTRICTS Gender Analysis May 2017 Contract No.: AID-617-C-160001 Submitted to: United States Agency for International Development June 2017 USAID’s Malaria Action Program for Districts Gender Analysis ii DISCLAIMER The authors’ views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development (USAID) or the United States Government. June 2017 USAID’s Malaria Action Program for Districts Gender Analysis iii Table of Contents ACRONYMS ...................................................................................................................................... VI EXECUTIVE SUMMARY ................................................................................................................... VIII 1. INTRODUCTION ...........................................................................................................................1 2. BACKGROUND ............................................................................................................................1 COUNTRY CONTEXT ...................................................................................................................3 USAID’S MALARIA ACTION PROGRAM FOR DISTRICTS .................................................................6 STUDY DESCRIPTION..................................................................................................................6 -

WHO UGANDA BULLETIN February 2016 Ehealth MONTHLY BULLETIN
WHO UGANDA BULLETIN February 2016 eHEALTH MONTHLY BULLETIN Welcome to this 1st issue of the eHealth Bulletin, a production 2015 of the WHO Country Office. Disease October November December This monthly bulletin is intended to bridge the gap between the Cholera existing weekly and quarterly bulletins; focus on a one or two disease/event that featured prominently in a given month; pro- Typhoid fever mote data utilization and information sharing. Malaria This issue focuses on cholera, typhoid and malaria during the Source: Health Facility Outpatient Monthly Reports, Month of December 2015. Completeness of monthly reporting DHIS2, MoH for December 2015 was above 90% across all the four regions. Typhoid fever Distribution of Typhoid Fever During the month of December 2015, typhoid cases were reported by nearly all districts. Central region reported the highest number, with Kampala, Wakiso, Mubende and Luweero contributing to the bulk of these numbers. In the north, high numbers were reported by Gulu, Arua and Koti- do. Cholera Outbreaks of cholera were also reported by several districts, across the country. 1 Visit our website www.whouganda.org and follow us on World Health Organization, Uganda @WHOUganda WHO UGANDA eHEALTH BULLETIN February 2016 Typhoid District Cholera Kisoro District 12 Fever Kitgum District 4 169 Abim District 43 Koboko District 26 Adjumani District 5 Kole District Agago District 26 85 Kotido District 347 Alebtong District 1 Kumi District 6 502 Amolatar District 58 Kween District 45 Amudat District 11 Kyankwanzi District -

UGANDA: Epidemics; Final Report No. MDRUG010
Final report UGANDA: Epidemics Emergency appeal n° MDRUG010 GLIDE n° EP-2008-000101-UGA 1 September 2009 Period covered by this Final Report: 10 July to 9 December 2008 Appeal target: CHF 947,079 Final Appeal coverage: 16%; <click here to go directly to the final financial report or here to view the contact details> Appeal history: • This Emergency Appeal was initially launched on 10 July 2008 for CHF 947,079 (USD 910,653 or EUR 586,427) for 6 months to assist 425,095 beneficiaries (85,019 households). • CHF 273,059 was initially allocated from the Federation’s Disaster Relief Emergency Fund (DREF) to support the National Society in responding by URCS WatSan Officer tries out the efficiency of a hand washing delivering assistance. facility in Agoro IDP camp Summary: This operation was implemented over 6 months starting July 2008 and completed by December 2008. During this period the Uganda Red Cross Society (URCS) was involved in key activities in collaboration with other implementing partners as well as the Government of Uganda. These interventions contributed to the containment of the cholera outbreaks in Mbale, Manafwa, Pallisa, Tororo and Butaleja by August 2008 with a cumulative total number of cases registered during the epidemic standing at 535 with 31 deaths (CFR 5.9 percent). However, case management and community mobilization and/or sensitization continued until December 2008 when predisposing factors (environmental hygiene conditions) were all improved. Besides the cholera interventions, the heightened control activities against hepatitis E contributed to a marked reduction in infection rates and mortality whereby, by 22 March 2009, only 51 suspected new cases with one death were registered in the 20 affected sub-counties in Kitgum district. -

Funding Going To
% Funding going to Funding Country Name KP‐led Timeline Partner Name Sub‐awardees SNU1 PSNU MER Structural Interventions Allocated Organizations HTS_TST Quarterly stigma & discrimination HTS_TST_NEG meetings; free mental services to HTS_TST_POS KP clients; access to legal services PrEP_CURR for KP PLHIV PrEP_ELIGIBLE Centro de Orientacion e PrEP_NEW Dominican Republic $ 1,000,000.00 88.4% MOSCTHA, Esperanza y Caridad, MODEMU Region 0 Distrito Nacional Investigacion Integral (COIN) PrEP_SCREEN TX_CURR TX_NEW TX_PVLS (D) TX_PVLS (N) TX_RTT Gonaives HTS_TST KP sensitization focusing on Artibonite Saint‐Marc HTS_TST_NEG stigma & discrimination, Nord Cap‐Haitien HTS_TST_POS understanding sexual orientation Croix‐des‐Bouquets KP_PREV & gender identity, and building Leogane PrEP_CURR clinical providers' competency to PrEP_CURR_VERIFY serve KP FY19Q4‐ KOURAJ, ACESH, AJCCDS, ANAPFEH, APLCH, CHAAPES, PrEP_ELIGIBLE Haiti $ 1,000,000.00 83.2% FOSREF FY21Q2 HERITAGE, ORAH, UPLCDS PrEP_NEW Ouest PrEP_NEW_VERIFY Port‐au‐Prince PrEP_SCREEN TX_CURR TX_CURR_VERIFY TX_NEW TX_NEW_VERIFY Bomu Hospital Affiliated Sites Mombasa County Mombasa County not specified HTS_TST Kitui County Kitui County HTS_TST_NEG CHS Naishi Machakos County Machakos County HTS_TST_POS Makueni County Makueni County KP_PREV CHS Tegemeza Plus Muranga County Muranga County PrEP_CURR EGPAF Timiza Homa Bay County Homa Bay County PrEP_CURR_VERIFY Embu County Embu County PrEP_ELIGIBLE Kirinyaga County Kirinyaga County HWWK Nairobi Eastern PrEP_NEW Tharaka Nithi County Tharaka Nithi County -

Kampala, Uganda; Telephone: (256-414) 7060000 Fax: (256-414) 237553/230370; E-Mail: [email protected]; Website
2014 NPHC - Main Report National Population and Housing Census 2014 Main Report 2014 NPHC - Main Report This report presents findings from the National Population and Housing Census 2014 undertaken by the Uganda Bureau of Statistics (UBOS). Additional information about the Census may be obtained from the Uganda Bureau of Statistics (UBOS), Plot 9 Colville Street, P.O. box 7186 Kampala, Uganda; Telephone: (256-414) 7060000 Fax: (256-414) 237553/230370; E-mail: [email protected]; Website: www.ubos.org. Cover Photos: Uganda Bureau of Statistics Recommended Citation Uganda Bureau of Statistics 2016, The National Population and Housing Census 2014 – Main Report, Kampala, Uganda 2014 NPHC - Main Report FOREWORD Demographic and socio-economic data are The Bureau would also like to thank the useful for planning and evidence-based Media for creating awareness about the decision making in any country. Such data Census 2014 and most importantly the are collected through Population Censuses, individuals who were respondents to the Demographic and Socio-economic Surveys, Census questions. Civil Registration Systems and other The census provides several statistics Administrative sources. In Uganda, however, among them a total population count which the Population and Housing Census remains is a denominator and key indicator used for the main source of demographic data. resource allocation, measurement of the extent of service delivery, decision making Uganda has undertaken five population and budgeting among others. These Final Censuses in the post-independence period. Results contain information about the basic The most recent, the National Population characteristics of the population and the and Housing Census 2014 was undertaken dwellings they live in. -
Final Project Report Bridging Gaps in Development and Emergency For
1110 Vermont Avenue NW, Suite 500 Washington, DC 20005 USA [email protected] www.hotosm.org Final Project Report Bridging Gaps in Development and Emergency for the Refugee Crisis in East Africa April 2018 - May 2019 Author(s): Humanitarian OpenStreetMap Team (HOT) Date of Report: May 31, 2019 Table of Contents 1. Acknowledgements 2 2. Executive Summary 3 3. Final Progress Report 4 4. Lessons Learned 19 5. Risk Mitigation 30 6. Output Indicators 31 7. Media Coverage 33 8. Conclusions 36 1 1. Acknowledgements This project, “Bridging Gaps in Development and Emergency for the Refugee Crisis in East Africa”, submitted in response to the 2017 call for proposals by the World Bank’s Development Data Group (DECDG) and the Global Partnership for Sustainable Development Data (GPSDD), is supported by the World Bank’s Trust Fund for Statistical Capacity Building (TFSCB) with financing from the United Kingdom's Department for International Development (DFID), the Government of Korea, and the Department of Foreign Affairs and Trade of Ireland. Special thanks and recognition to the local governments, refugee and host communities and organizations who collaborated with the HOT team through the duration of this project; the success and impact of our activities could have not been possible without their full support and participation in the mission: Action Against Hunger, Arua District Local Government, Bidibidi Refugee Settlement, Catholic Relief Services, Danish Refugee Council, Food and Agriculture Organization, Finnish Refugee Council, Hoima District -

Women's Civic Engagement in Nebbi and Yumbe Districts
WOMEN’S CIVIC ENGAGEMENT IN NEBBI AND YUMBE DISTRICTS BASELINE STUDY REPORT Conducted by: Dr. Alfred Lakwo and Wilfred Cwinyaai Agency For Accelerated Regional Development (AFARD), Nebbbi Funded by: Delegation of European Commission in Uganda (Grant # DCI-NSAPVD/2008/169-745) MAY 2009 ACKNOWLEDGEMENT This study was conducted under the “Engendering Decentralized Poverty Resources Management Project” (Grant # DCI‐NSAPVD/2008/169‐745) being funded in partnership by European Commission in Uganda and the Agency For Accelerated Regional Development (AFARD). AFARD is indebted to various district local government staffs in Nebbi for the efforts invested in discussing the data collection framework and also to all the data collectors especially the Community Development Officers located in the various local governments. Finally, we are also grateful to the district officials from both Nebbi and Yumbe for their wilful and active participation in the feedback meeting that shaped this report but particularly the ways forward. AFARD, however, takes full responsibility for the views and errors expressed herein. Dr. Alfred Lakwo Programme Director Nebbi, Tuesday, 05 May 2009 This document has been produced with the financial assistance of the European Union. The contents of this document are the sole responsibility of AFARD and can under no circumstances be regarded as reflecting the position of the European Union. 1 | Engendering Decentralized Poverty Resources Management Project Baseline Study Report, May 2009 ACRONYMS AFARD = Agency for Accelerated -

YUMBE DISTRICT Family Planning Costed Implementation Plan 2018/19 - 2022/23
REPUBLIC OF UGANDA YUMBE DISTRICT Family Planning Costed Implementation Plan 2018/19 - 2022/23 OCTOBER 2018 YUMBE DISTRICT LOCAL GOVERNMENT ii iii This District Family Planning Costed Implementation Plan has been made possible with the technical support from the Ministry of Health and the United Nations Population Fund through Yumbe District Health Office. This project was funded under the UNFPA Supplies Programme and UK aid from the UK government. Published by: Yumbe District Local Government Ownership: Reproduction of this plan for educational or other non-commercial purposes is authorized without permission from the Yumbe District Local Government, provided the source is fully acknowledged. Preferred Citation: Yumbe District (2018). District Family Planning Costed Implementation Plan, 2018/19-2022/23. Yumbe, Uganda Copies available from: Yumbe District Health Office iv Table of Contents List of Tables v List of Figures v FOREWORD vi PREFACE vii ACKNOWLEDGMENT viii ACRONYMS ix EXECUTIVE SUMMARY x SECTION ONE: INTRODUCTION AND BACKGROUND 1 1.1 Introduction 1 1.2 Background 2 1.3 SWOT Analysis for Family Planning Services 17 1.4 Process of Developing the District FP CIP 18 SECTION TWO: THE CASE FOR YUMBE DISTRICT FP COSTED IMPLEMENTATION PLAN 19 2.1 Introduction 20 2.2 Demand Creation 20 2.3 Access to Service Delivery and Yumbe District Family Planning Uptake 20 2.4 Contraceptive Security 20 2.5 Policy and Enabling Environment 21 2.6 Financing 21 2.7 Stewardship, Management and Accountability 21 SECTION THREE: DISTRICT STRATEGIC PRIORITIES -
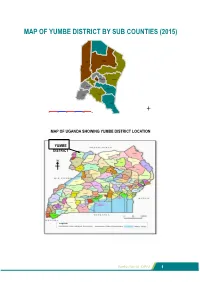
Map of Yumbe District by Sub Counties (2015)
MAP OF YUMBE DISTRICT BY SUB COUNTIES (2015) Kerwa Midigo Kei Kochi Apo Yumbe Town Council Romogi Kuru Lodonga Kululu Odravu Drajini Ariwa l km 538 1076 1614 2152 2690 MAP OF UGANDA SHOWING YUMBE DISTRICT LOCATION YUMBE DISTRICT PB Yumbe District DDP2 Yumbe District DDP2 1 YUMBE DISTRICT Vision “An improved Community from a Peasant to a Modern and Prosperous District within the National Planning Continuum of 30 years” Mission Statement “To serve the community through coordinated delivery of services which focus on National and Local priorities and contribute to the improvement in the quality of life of the people” Theme “Enhancing the Districts’ effort for Sustainable Wealth Creation, through Employment and Inclusive Growth for improved livelihood of the population” 2 Yumbe District DDP2 Yumbe District DDP2 3 FORWARD The Yumbe District Second Development Planning process was premised on the overall national vision and theme of the National Plan especially the focus on “Strengthening Uganda’s Competitiveness for Sustainable Wealth Creation, Employment and Inclusive Growth”. Effort was made to identify and specify inter-sectoral linkages, synergies and complementarities where sectors are categorized as Primary growth, complementary, social services and enabling sectors. The task of making the plan was a concerted effort of many stakeholders, both political and technical. Development concerns and priorities were generated right from the Lower Local Councils, especially the villages upwards to the district level. From the villages, these priorities were then refined and forwarded to the Parishes were they were incorporated into the Parish Investment Plan and forwarded to Sub-Counties with feedback linkages to the Villages.