(Or Proton-Activated) Receptor - GPR4 and OGR1 in Intestinal Inflammation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Edinburgh Research Explorer
Edinburgh Research Explorer International Union of Basic and Clinical Pharmacology. LXXXVIII. G protein-coupled receptor list Citation for published version: Davenport, AP, Alexander, SPH, Sharman, JL, Pawson, AJ, Benson, HE, Monaghan, AE, Liew, WC, Mpamhanga, CP, Bonner, TI, Neubig, RR, Pin, JP, Spedding, M & Harmar, AJ 2013, 'International Union of Basic and Clinical Pharmacology. LXXXVIII. G protein-coupled receptor list: recommendations for new pairings with cognate ligands', Pharmacological reviews, vol. 65, no. 3, pp. 967-86. https://doi.org/10.1124/pr.112.007179 Digital Object Identifier (DOI): 10.1124/pr.112.007179 Link: Link to publication record in Edinburgh Research Explorer Document Version: Publisher's PDF, also known as Version of record Published In: Pharmacological reviews Publisher Rights Statement: U.S. Government work not protected by U.S. copyright General rights Copyright for the publications made accessible via the Edinburgh Research Explorer is retained by the author(s) and / or other copyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associated with these rights. Take down policy The University of Edinburgh has made every reasonable effort to ensure that Edinburgh Research Explorer content complies with UK legislation. If you believe that the public display of this file breaches copyright please contact [email protected] providing details, and we will remove access to the work immediately and investigate your claim. Download date: 02. Oct. 2021 1521-0081/65/3/967–986$25.00 http://dx.doi.org/10.1124/pr.112.007179 PHARMACOLOGICAL REVIEWS Pharmacol Rev 65:967–986, July 2013 U.S. -

GPR4 Deficiency Alleviates Intestinal Inflammation in a Mouse Model of Acute Experimental Colitis
GPR4 deficiency alleviates intestinal inflammation in a mouse model of acute experimental colitis The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters. Citation Sanderlin, Edward J. et al. “GPR4 Deficiency Alleviates Intestinal Inflammation in a Mouse Model of Acute Experimental Colitis.” Biochimica et Biophysica Acta (BBA)- Molecular Basis of Disease 1863, 2 (February 2017): 569–584 © 2016 Elsevier B.V. As Published http://dx.doi.org/10.1016/J.BBADIS.2016.12.005 Publisher Elsevier Version Author's final manuscript Citable link http://hdl.handle.net/1721.1/117655 Terms of Use Creative Commons Attribution-NonCommercial-NoDerivs License Detailed Terms http://creativecommons.org/licenses/by-nc-nd/4.0/ HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Biochim Manuscript Author Biophys Acta. Manuscript Author Author manuscript; available in PMC 2018 February 01. Published in final edited form as: Biochim Biophys Acta. 2017 February ; 1863(2): 569–584. doi:10.1016/j.bbadis.2016.12.005. GPR4 Deficiency Alleviates Intestinal Inflammation in a Mouse Model of Acute Experimental Colitis Edward J. Sanderlin1,*, Nancy R. Leffler1,*, Kvin Lertpiriyapong2,*, Qi Cai3, Heng Hong3, Vasudevan Bakthavatchalu4, James G. Fox4, Joani Zary Oswald5, Calvin R. Justus1, Elizabeth A. Krewson5, Dorcas O’Rourke2, and Li V. Yang1,5,# 1Department of Internal Medicine, Brody School of Medicine, East Carolina University 2Department of Comparative Medicine, Brody School of Medicine, East Carolina University 3Department of Pathology, Brody School of Medicine, East Carolina University 4Division of Comparative Medicine, Massachusetts Institute of Technology 5Department of Anatomy and Cell Biology, Brody School of Medicine, East Carolina University Abstract GPR4 is a proton-sensing G protein-coupled receptor that can be activated by extracellular acidosis. -

Multi-Functionality of Proteins Involved in GPCR and G Protein Signaling: Making Sense of Structure–Function Continuum with In
Cellular and Molecular Life Sciences (2019) 76:4461–4492 https://doi.org/10.1007/s00018-019-03276-1 Cellular andMolecular Life Sciences REVIEW Multi‑functionality of proteins involved in GPCR and G protein signaling: making sense of structure–function continuum with intrinsic disorder‑based proteoforms Alexander V. Fonin1 · April L. Darling2 · Irina M. Kuznetsova1 · Konstantin K. Turoverov1,3 · Vladimir N. Uversky2,4 Received: 5 August 2019 / Revised: 5 August 2019 / Accepted: 12 August 2019 / Published online: 19 August 2019 © Springer Nature Switzerland AG 2019 Abstract GPCR–G protein signaling system recognizes a multitude of extracellular ligands and triggers a variety of intracellular signal- ing cascades in response. In humans, this system includes more than 800 various GPCRs and a large set of heterotrimeric G proteins. Complexity of this system goes far beyond a multitude of pair-wise ligand–GPCR and GPCR–G protein interactions. In fact, one GPCR can recognize more than one extracellular signal and interact with more than one G protein. Furthermore, one ligand can activate more than one GPCR, and multiple GPCRs can couple to the same G protein. This defnes an intricate multifunctionality of this important signaling system. Here, we show that the multifunctionality of GPCR–G protein system represents an illustrative example of the protein structure–function continuum, where structures of the involved proteins represent a complex mosaic of diferently folded regions (foldons, non-foldons, unfoldons, semi-foldons, and inducible foldons). The functionality of resulting highly dynamic conformational ensembles is fne-tuned by various post-translational modifcations and alternative splicing, and such ensembles can undergo dramatic changes at interaction with their specifc partners. -

1 Supplemental Material Maresin 1 Activates LGR6 Receptor
Supplemental Material Maresin 1 Activates LGR6 Receptor Promoting Phagocyte Immunoresolvent Functions Nan Chiang, Stephania Libreros, Paul C. Norris, Xavier de la Rosa, Charles N. Serhan Center for Experimental Therapeutics and Reperfusion Injury, Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts 02115, USA. 1 Supplemental Table 1. Screening of orphan GPCRs with MaR1 Vehicle Vehicle MaR1 MaR1 mean RLU > GPCR ID SD % Activity Mean RLU Mean RLU + 2 SD Mean RLU Vehicle mean RLU+2 SD? ADMR 930920 33283 997486.5381 863760 -7% BAI1 172580 18362 209304.1828 176160 2% BAI2 26390 1354 29097.71737 26240 -1% BAI3 18040 758 19555.07976 18460 2% CCRL2 15090 402 15893.6583 13840 -8% CMKLR2 30080 1744 33568.954 28240 -6% DARC 119110 4817 128743.8016 126260 6% EBI2 101200 6004 113207.8197 105640 4% GHSR1B 3940 203 4345.298244 3700 -6% GPR101 41740 1593 44926.97349 41580 0% GPR103 21413 1484 24381.25067 23920 12% NO GPR107 366800 11007 388814.4922 360020 -2% GPR12 77980 1563 81105.4653 76260 -2% GPR123 1485190 46446 1578081.986 1342640 -10% GPR132 860940 17473 895885.901 826560 -4% GPR135 18720 1656 22032.6827 17540 -6% GPR137 40973 2285 45544.0809 39140 -4% GPR139 438280 16736 471751.0542 413120 -6% GPR141 30180 2080 34339.2307 29020 -4% GPR142 105250 12089 129427.069 101020 -4% GPR143 89390 5260 99910.40557 89380 0% GPR146 16860 551 17961.75617 16240 -4% GPR148 6160 484 7128.848113 7520 22% YES GPR149 50140 934 52008.76073 49720 -1% GPR15 10110 1086 12282.67884 -
Supplementary Data, Ms Iring Et Al. Re-Revised
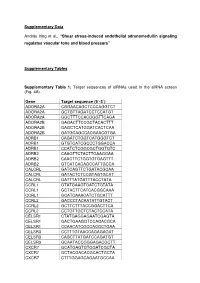
Supplementary Data András Iring et al., “Shear stress-induced endothelial adrenomedullin signaling regulates vascular tone and blood pressure” Supplementary Tables Supplementary Table 1. Target sequences of siRNAs used in the siRNA screen (Fig. 4A). Gene Target sequence (5´-3´) ADORA2A CGGAACAGCTCCCAGGTCT ADORA2A GCTGTTAGATCCTCCATGT ADORA2A GGCTTTCCACGGGTTCAGA ADORA2B GAGACTTCCGCTACACTTT ADORA2B GAGCTCATGGATCACTCAA ADORA2B GATGCAGCCACGAACGTGA ADRB1 CAGATCTGGTCATGGGTCT ADRB1 GTGTCATCGCCCTGGACCA ADRB1 CCATCTCGGCGCTGGTGTC ADRB2 CAAGTTCTACTTGAAGGAA ADRB2 CAACTTCTGGTGTGAGTTT ADRB2 GTCATCACAGCCATTGCCA CALCRL GATCAGTTCTGATACGCAA CALCRL GATACTCTCCGTAGTGCAT CALCRL GATTTATGATTTACCTATA CCRL1 GTATGAAGTGATCTGTATA CCRL1 GCTACTTCATCACGGCAAA CCRL1 GCATCAAACATCTGCATTT CCRL2 GACCCTACAATATTGTACT CCRL2 GCTTCTTTACCGGACTTCA CCRL2 CCTGTTGCTCTACTCCATA CELSR1 CTATGAGGAGAATCGAGTA CELSR1 GACTGAAGGTCCAGACGCA CELSR1 CCAACATCGCCACGCTGAA CELSR3 CCTTTGTAACCAGAGAGAT CELSR3 CAGCTTATGATCCAGATGT CELSR3 GCAATACCGGGAGACGCTT CXCR7 GCATGAGTGTGGATCGCTA CXCR7 GCTACGACACGCACTGCTA CXCR7 CTTTGGAGCAGAATGCCAA 2 ELTD1 CTCTTCTAATTCAACTCTT ELTD1 CAAGTTTATTACTAATGAT ELTD1 GTACCATACAGCTATAGTA FZD1 GTAACCAATGCCAAACTTT FZD1 GATTAGCCACCGAAATAAA FZD1 CAGTGTTCCGCCGAGCTCA FZD2 CGCTTTGCGCGCCTCTGGA FZD2 GACATGCAGCGCTTCCGCT FZD2 CGCACTACACGCCGCGCAT FZD4 GTATGTGCTATAATATTTA FZD4 CCATTGTCATCTTGATTAT FZD4 CCAACATGGCAGTGGAAAT FZD5 GGATTTAAGGCCCAGTTTA FZD5 GACCATAACACACTTGCTT FZD5 CAAGTGATCCTGGGAAAGA FZD6 GCATTGTATCTCTTATGTA FZD6 GTGCTTACTGAGTGTCCAA FZD6 CCAATTACTGTTCCCAGAT FZD8 CCATCTGCCTAGAGGACTA -

Can GPR4 Be a Potential Therapeutic Target for COVID-19?
HYPOTHESIS AND THEORY published: 21 January 2021 doi: 10.3389/fmed.2020.626796 Can GPR4 Be a Potential Therapeutic Target for COVID-19? Li V. Yang 1,2*, Karen A. Oppelt 3, Mary Jane Thomassen 1, Mona A. Marie 1, Shayan Nik Akhtar 2 and Justin D. McCallen 1 1 Department of Internal Medicine, Brody School of Medicine, East Carolina University, Greenville, NC, United States, 2 Department of Anatomy and Cell Biology, Brody School of Medicine, East Carolina University, Greenville, NC, United States, 3 Department of Comparative Medicine, Brody School of Medicine, East Carolina University, Greenville, NC, United States Coronavirus disease 19 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first emerged in late 2019 and has since rapidly become a global pandemic. SARS-CoV-2 infection causes damages to the lung and other organs. The clinical manifestations of COVID-19 range widely from asymptomatic infection, mild respiratory illness to severe pneumonia with respiratory failure and death. Autopsy studies demonstrate that diffuse alveolar damage, inflammatory cell infiltration, edema, proteinaceous exudates, and vascular thromboembolism in the Edited by: Zisis Kozlakidis, lung as well as extrapulmonary injuries in other organs represent key pathological International Agency for Research on findings. Herein, we hypothesize that GPR4 plays an integral role in COVID-19 Cancer (IARC), France pathophysiology and is a potential therapeutic target for the treatment of COVID-19. Reviewed by: GPR4 is a pro-inflammatory G protein-coupled receptor (GPCR) highly expressed in Sujit Pujhari, University of South Carolina, vascular endothelial cells and serves as a “gatekeeper” to regulate endothelium-blood United States cell interaction and leukocyte infiltration. -

Pharmacological Inhibition of GPR4 Remediates Intestinal Inflammation in a Mouse Colitis
bioRxiv preprint doi: https://doi.org/10.1101/533174; this version posted January 29, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Pharmacological inhibition of GPR4 remediates intestinal inflammation in a mouse colitis model Edward J. Sanderlina, Mona Mariea, Juraj Velcickyc, Pius Loetscherc, Li V. Yanga,b,* aDepartment of Internal Medicine, Brody School of Medicine, East Carolina University, USA bDepartment of Anatomy and Cell Biology, Brody School of Medicine, East Carolina University, USA cNovartis Institutes for BioMedical Research, CH-4002 Basel, Switzerland * Corresponding author: Li V. Yang, Ph.D., Department of Internal Medicine, Brody School of Medicine, East Carolina University, 600 Moye Blvd., Greenville, NC 27834, U.S.A. Email: [email protected]; Phone: +1-252-744-3419 bioRxiv preprint doi: https://doi.org/10.1101/533174; this version posted January 29, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Abstract Inflammatory bowel disease (IBD) is characterized by chronic, recurring inflammation of the digestive tract. Current therapeutic approaches are limited and include biologics and steroids such as anti-TNFα monoclonal antibodies and corticosteroids, respectively. Significant adverse drug effects can occur for chronic usage and include increased risk of infection in some patients. -

9Bdf85231de61d9e74d1273aa7
RESEARCH ARTICLE Characterization of Imidazopyridine Compounds as Negative Allosteric Modulators of Proton-Sensing GPR4 in Extracellular Acidification-Induced Responses Ayaka Tobo1, Masayuki Tobo1, Takashi Nakakura1, Masashi Ebara1, Hideaki Tomura1, Chihiro Mogi1, Dong-Soon Im2, Naoya Murata1, Atsushi Kuwabara1, Saki Ito3, Hayato Fukuda3, Mitsuhiro Arisawa3, Satoshi Shuto3,4, Michio Nakaya5, Hitoshi Kurose5, Koichi Sato1*, Fumikazu Okajima1* 1 Laboratory of Signal Transduction, Institute for Molecular and Cellular Regulation, Gunma University, Maebashi, Japan, 2 Laboratory of Pharmacology, College of Pharmacy, Pusan National University, Busan, Republic of Korea, 3 Faculty of Pharmaceutical Science, Hokkaido University, Sapporo, Japan, 4 Center for Research and Education on Drug Discovery, Hokkaido University, Sapporo, Japan, 5 Department of Pharmacology and Toxicology, Graduate School of Pharmaceutical Sciences, Kyushu University, Fukuoka, Japan OPEN ACCESS * [email protected] (FO); [email protected] (KS) Citation: Tobo A, Tobo M, Nakakura T, Ebara M, Tomura H, Mogi C, et al. (2015) Characterization of Imidazopyridine Compounds as Negative Allosteric Modulators of Proton-Sensing GPR4 in Extracellular Abstract Acidification-Induced Responses. PLoS ONE 10(6): e0129334. doi:10.1371/journal.pone.0129334 G protein-coupled receptor 4 (GPR4), previously proposed as the receptor for sphingosyl- phosphorylcholine, has recently been identified as the proton-sensing G protein-coupled Academic Editor: Chaoyang Xue, Rutgers University, UNITED -

Role of the G-Protein-Coupled Receptor GPR12 As High-Affinity Receptor for Sphingosylphosphorylcholine and Its Expression and Function in Brain Development
The Journal of Neuroscience, February 1, 2003 • 23(3):907–914 • 907 Role of the G-Protein-Coupled Receptor GPR12 as High-Affinity Receptor for Sphingosylphosphorylcholine and Its Expression and Function in Brain Development Atanas Ignatov,1* Julia Lintzel,1* Irm Hermans-Borgmeyer,1 Hans-Ju¨rgen Kreienkamp,2 Patrick Joost,3 Susanne Thomsen,3 Axel Methner,3 and H. Chica Schaller1 1Zentrum fu¨r Molekulare Neurobiologie Hamburg, 2Institut fu¨r Zellbiochemie und klinische Neurobiologie, and 3Klinik fu¨r Neurologie, Universita¨t Hamburg, D-20246 Hamburg, Germany Lysophospholipids are bioactive molecules influencing numerous cellular processes such as proliferation, differentiation, and motility. As extracellular ligands, they interact with specific members of the G-protein-coupled receptor family. We show in this paper that the lysophospholipidsphingosylphosphorylcholineisahigh-affinityligandfortheorphanG-protein-coupledreceptorGPR12.Heterologous expression of GPR12 in Chinese hamster ovary cells and in frog oocytes revealed a high-affinity interaction with sphingosylphosphoryl- choline in the nanomolar range. Blockade of its action by pertussis toxin was taken as evidence that GPR12 is coupled to an inhibitory G-protein. In the adult mouse brain, GPR12 was expressed in the limbic system. During mouse embryonal development, GPR12 tran- scripts were detected in the CNS, especially in areas where neuronal differentiation occurs. Consistent with this we found that cultures of embryonal cerebral cortical neurons responded to sphingosylphosphorylcholine with an increase in synaptic contacts. The GPR12- expressing hippocampal cell line HT22 reacted to sphingosylphophorylcholine with an increase in cell proliferation and cell clustering. Other receptors known to interact at nanomolar concentrations with sphingosylphosphorycholine were expressed neither in the devel- oping cerebral cortex nor in the HT22 cell line. -

Role of Ph Receptor GPR4 in Inflammatory Bowel Disease
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2018 The proton-activated receptor GPR4 modulates intestinal inflammation Wang, Yu ; de Vallière, Cheryl ; Imenez Silva, Pedro H ; Leonardi, Irina ; Gruber, Sven ; Gerstgrasser, Alexandra ; Melhem, Hassan ; Weber, Achim ; Leucht, Katharina ; Wolfram, Lutz ; Hausmann, Martin ; Krieg, Carsten ; Thomasson, Koray ; Boyman, Onur ; Frey-Wagner, Isabelle ; Rogler, Gerhard ; Wagner, Carsten A Abstract: BACKGROUND AND AIMS: During active inflammation tissue intraluminal intestinal pH is decreased in patients with inflammatory bowel disease (IBD). Acidic pH may play a role in IBD patho- physiology. Recently, proton sensing G-protein coupled receptors were identified, including GPR4, OGR1 (GPR68), and TDAG8 (GPR65). We investigated whether GPR4 is involved in intestinal inflammation. METHODS: The role of GPR4 was assessed in murine colitis models: chronic dextran sulphate sodium (DSS) administration and by crossbreeding into an IL-10 deficient background for development of sponta- neous colitis. Colitis severity was assessed by body weight, colonoscopy, colon length, histological score, cytokine mRNA expression, and myeloperoxidase (MPO) activity. In the spontaneous Il-10-/- colitis model, the incidence of rectal prolapse and characteristics of lamina propria leukocytes (LPLs) were an- alyzed. RESULTS: Gpr4-/- mice showed reduced body weight loss and histology score after induction of chronic DSS colitis. In Gpr4-/- /Il-10-/- double knock-outs the onset and progression of rectal prolapse were significantly delayed and mitigated compared to Gpr4+/+ /Il-10-/- mice. Double knock-out mice showed lower histology scores, MPO activity, CD4 + T-helper cell infiltration, IFN-, iNOS, MCP-1 (CCL2), CXCL1 and CXCL2 expression compared to controls. -

RT² Profiler PCR Array (384-Well Format) Mouse G Protein Coupled Receptors 384HT
RT² Profiler PCR Array (384-Well Format) Mouse G Protein Coupled Receptors 384HT Cat. no. 330231 PAMM-3009ZE For pathway expression analysis Format For use with the following real-time cyclers RT² Profiler PCR Array, Applied Biosystems® models 7900HT (384-well block), Format E ViiA™ 7 (384-well block); Bio-Rad CFX384™ RT² Profiler PCR Array, Roche® LightCycler® 480 (384-well block) Format G Description The Mouse G Protein Coupled Receptors 384HT RT² Profiler™ PCR Array profiles the expression of a comprehensive panel of 370 genes encoding the most important G Protein Coupled Receptors (GPCR). GPCR regulate a number of normal biological processes and play roles in the pathophysiology of many diseases upon dysregulation of their downstream signal transduction activities. As a result, they represent 30 percent of the targets for all current drug development. Developing drug screening assays requires a survey of which GPCR the chosen cell-based model system expresses, to determine not only the expression of the target GPCR, but also related GPCR to assess off-target side effects. Expression of other unrelated GPCR (even orphan receptors whose ligand are unknown) may also correlate with off-target side effects. The ligands that bind and activate the receptors on this array include neurotransmitters and neuropeptides, hormones, chemokines and cytokines, lipid signaling molecules, light-sensitive compounds, and odorants and pheromones. The normal biological processes regulated by GPCR include, but are not limited to, behavioral and mood regulation (serotonin, dopamine, GABA, glutamate, and other neurotransmitter receptors), autonomic (sympathetic and parasympathetic) nervous system transmission (blood pressure, heart rate, and digestive processes via hormone receptors), inflammation and immune system regulation (chemokine receptors, histamine receptors), vision (opsins like rhodopsin), and smell (olfactory receptors for odorants and vomeronasal receptors for pheromones). -

Introduction
GPCR Introduction G protein-coupled receptors (GPCRs) are the GPCRs Super-Family largest family of transmembrane receptors and are 375 GPCR Drug Targets, 225 with Known Ligands, 150 Orphan Targets responsible for the transduction of a diverse range of extracellular signals. The range of physiological processes mediated by GPCRs makes them one GRM7 GRM8 GLUTAMATE (15) SECRETIN GRM2 FZD7 TAS1R3 FZD2 of the most important classes of proteins for drug (15) GRM4 GRM3 TAS1R1FZD1 GLP2R GIPR GRM6 GRPC6A FRIZZED/TAS2 discovery. ADHESION GLP1R GCGR GRM5 FZD3 PTHR2 GRM1 (24) LEC1 VIPR2 PTHR1 (24) TAS1R2 FZD6 LEC2 TAS2R13 CELSR2PACAP FZD8 The study of GPCRs may involve ligand binding, G CRHR2 FZD5 TAS2R16 TAS2R14 CALCRL LEC3 VIPR1 CRHR1 CASR GABBR2 FZD10 TAS2R1 TAS2R10 EMR3EMR2 CELSR3 BAI2 CALCR FZD4 TAS2R5 TAS2R3 SCTR FZD9 protein activation, internalization, and downstream ETL BAI3 GPR60 TAS2R9 CELSR1 GHRHR GABBR1 GPR59 TAS2R8 TAS2R4 TAS2R7 EMR1 BAI1 SMOH CXCR3 second messenger events. Each step of the CXCR5 CCR11 CXCR2 CD97 SSTR1 SSTR3 CCR10 CCR6 SSTR5 CXCR1 GPR111 CXCR6 pathway offers an opportunity to exploit the full SSTR2 CCR9 GPR115 SSTR4 CCR7 GPR116 GPR112 GPR8 CCRL2 GPR113 GPR7 CXC3R1CCR8 therapeutic potential of targeting GPCRs. GPR110 CCR4 HE6 NTSR2 CCR1 TM7XN1 GPR114 NMU1R GPR54 GALR1 CCBP2 GHSR GALR2 RDC1 CCR3 GPR97 NPY1R XCR1 PPYR1 NMU2R MTLR MCHR1 GALR3 ADMR NPY2R AGTR1 TACR3 UR2R MCHR2 AGTRL1 AGTR2 CCR5 TAC3RL PrRP γ GPR26 BDKRB2 CCR2 GRM7 GRM8 GLUTAMATE (15) TACR1 TACR2 GRP72 OR1A1 SALPR OLFACTORY GPR15 NPFF1 NPY5R OR1D2 (388) GPTH2