Laws and Rules Booklet
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Evolution of Surgical Endodontics: Never and Always Prof. Marwan Abou-Rass DDS, MDS, Ph.D
The Evolution of Surgical Endodontics: Never and Always Prof. Marwan Abou-Rass DDS, MDS, Ph.D Introduction This paper came out of discussions with Hu-Friedy as we were developing new materials describing the Marwan Abou-Rass, or “MAR” microsurgical endodontic instrument line. Since I have been teaching, conducting research and performing microsurgical endodontics for many years, Hu-Friedy was interested in my perspective on the evolution of the specialty, and what the future might hold. I tried to fit it all in the sales brochure we were working on, but how can one compress decades of change into a few short paragraphs? Hence, we decided to make it a separate venture. Since graduating from dental school and completing my endodontic training, I have been immersed in university environments where dialog regarding best practices in endodontics can be collaborative, and sometimes heated -- because my academic and clinical peers are passionate about what we do. Throughout my career I have collaborated with many global peers who have combined innovation and critical thinking with willingness to risk being “wrong”. As a result, the profession has made significant advances for which we have all benefited. It is for them that I dedicate this paper. This paper outlines my perspective on how microsurgical endodontics has progressed over several decades, from its infancy in the 1940s, through developments which have shaped the practice today. I conclude with “educated guesses” regarding what the future may hold. I. The Influence of Oral Surgery Period In the 1940s, endodontic surgery was often performed by oral surgeons, adapting their methods and instruments used for oral surgery. -
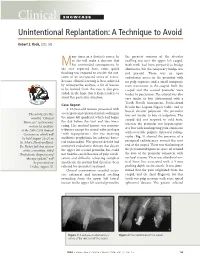
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -
CODA.Org: Accreditation Standards for Prosthodontics Programs
Commission on Dental Accreditation Accreditation Standards for Advanced Dental Education Programs in Prosthodontics Accreditation Standards for Advanced Dental Education Programs in Prosthodontics Commission on Dental Accreditation 211 East Chicago Avenue Chicago, Illinois 60611-2678 (312) 440-4653 www.ada.org/coda Copyright© 2020 Commission on Dental Accreditation All rights reserved. Reproduction is strictly prohibited without prior written permission. Prosthodontics Standards -2- Accreditation Standards for Advanced Dental Education Programs in Prosthodontics Document Revision History Date Item Action August 7, 2015 Accreditation Standards for Advanced Adopted Specialty Education Programs in Prosthodontics August 7, 2015 Revision to Policy on Reporting Program Adopted and Implemented Changes in Accredited Programs Adopted and Implemented August 7, 2015 Revised Policy on Enrollment Increases in Adopted and Implemented Advanced Dental Specialty Program Adopted and Implemented February 5, 2016 Revised Accreditation Status Definition Adopted and Implemented Implemented February 5, 2016 Revised Policy on Program Changes Revised Policy on Enrollment Increases in February 5, 2016 Advanced Dental Specialty Programs Accreditation Standards for Advanced July 1, 2016 Specialty Education Programs in Prosthodontics August 5, 2016 Revised Policy on Program Changes Adopted and Implemented August 5, 2016 Revised Policy n Enrollment Increases in Adopted and Advanced Dental Specialty Programs Implemented August 5, 2016 Revised Standard 6, Research Adopted -
And Picked up By
s:recoil of President the effect of a singleAot '`Shooting at taped melons t 'dt:iVen away from:the, rifle •„eotion. We. analyse previous •er film by cri and failure of t 41,60,0h* „4., Alvaro-z)` .clit6h) Aze .listed here is meant, to indicate content' is the work of k, The tests of a hypothesis by L.W. 4 whia the report to yen fOr: your el-Lab:it*. flents. of article on the- .p ygic's 'of,the problem to 1 for physicists. i...1e 0 distribute port to studentsOf't sport after been considered, and after ort version e Phyttics Today article well, picked up by Ahis Material strictly confidential at#this time. -t 1970 ,eastrertypy aer,the Report of the aarran C-laission on Der busheid ow, that s;lerpky, Dbmwrneadaltion of,Proidont Irisready bas booth. question of the number nairaiwoulse ~U. & looked Itsettelt 11101.4. .001-410411sWer the sate fired. If shots oar from two dIffc-rent directions, notion is *nigh* mast ha* isemmitia4 /21110‘ shit ligpeleals,heme boom a conspiracy. Critics of the Whrren hour: have drawn from the treat, es this Dr...46 J4 IMOOWN401161C, 41, 0MOOtkagainst the Commission's conclusions from the principal physical ph ysiclat adlimarelegists 100004 of the assassination, a 25-second color film taken by amateur photographer &simony lbw** hit* a projarte3044 is. Uproar* given a sale& that deratiom as that of the RweJwwtillow At a shoot* , the ducks fall 404,4,0011,the sat detailed study yet published of this and other photographs of martini s. athwart if someone is shot, advise eat strelmealoWthe of rersiX will* 047 400 ,,,igio.empoggiaamien is ALE &mood* ew Xnllss, by Haver/oral philosophy professor toward - the (Page Deseahasis added) • ' • 1 . -
Lessons Unlearned—The Gun Lobby and the Siren Song of Anti
Lessons Unlearned The Gun Lobby and the Siren Song of Anti-Government Rhetoric Violence Policy Center April 2010 The Violence Policy Center (VPC) is a national non-profit educational organization that conducts research and public education on violence in America and provides information and analysis to policymakers, journalists, advocates, and the general public. This report was authored by VPC Executive Director Josh Sugarmann and VPC Policy Analyst Marty Langley. The study was funded in part with the support of the David Bohnett Foundation, The Joyce Foundation, and the Public Welfare Foundation. Past studies released by the VPC include: ! Target: Law Enforcement—Assault Weapons in the News (February 2010) ! Black Homicide Victimization in the United States: An Analysis of 2007 Homicide Data (January 2010) ! When Men Murder Women—An Analysis of 2007 Homicide Data (September 2009) ! Law Enforcement and Private Citizens Killed by Concealed Handgun Permit Holders—An Analysis of News Reports, May 2007 to April 2009 (July 2009) ! Indicted: Types of Firearms and Methods of Gun Trafficking from the United States to Mexico as Revealed in U.S. Court Documents (April 2009) ! Iron River: Gun Violence and Illegal Firearms Trafficking on the U.S.-Mexico Border (March 2009) ! Youth Gang Violence and Guns: Data Collection in California (February 2009) ! “Big Boomers”—Rifle Power Designed Into Handguns (December 2008) ! American Roulette: Murder-Suicide in the United States (April 2008) ! An Analysis of the Decline in Gun Dealers: 1994 to 2007 (August -

The Catchiest Disease “Hesitation Marks” Embodies a Ruined Man Many a Personal Downfall in This Album by Max Robison Contributing Writer Especially
Tuesday, Features Sept. 10, 2013 11 “Get to Know a Retriever” Meet Arash Fallah, a student driven to succeed at UMBC have been mentoring me club wrestling team but I would really like to see I really look up to their the team be elevated to a andhumility, I’ve learned grace, aclass lot from. and formal collegiate level. Beverage choice that’s wisdom.is extremely Farrah intelligent,Daham is indicative of your onetrustworthy, of my role models.nuanced She personality? characteristics I admire in anda person. beautiful. Those are Pepsi,Keep Calmit’s sweet and and_________? dark. What is your favorite COURTESY ARASH FALLAH part about UMBC? RelaxHow has UMBC helped Arash Fallah rides a carousel at Whatever you want to you achieve success? Pentagon mall. With little exception, there importance of failure BY DAVID POZNANSKY doare atfew UMBC, obstacles you keepingcan do. It’s taught me the Contributing Writer you from pursuing your understanding that few passions. andadvantages success. comeAs well from as Name, Major, Year? taking a position of conceit. Sports team you’d be most excited to see play a measured impact by Arash Fallah, History and live? I’veapplying learned the lessonshow to of make tact. PoliticalFrom? Science, 2015 Potomac, Maryland challenge myself by taking LosWhat Angeles sport Lakers or activity It’s also encouraged me to Do you have any should UMBC compete in than merely coasting role models? What on a collegiate level? difficultthrough college.courses rather characteristics of theirs do you admire? have such an outstanding [email protected] I think it’s great that we There are two people who The catchiest disease “Hesitation Marks” embodies a ruined man many a personal downfall in this album BY MAX ROBISON Contributing Writer especially. -

On Emerging Clinical Dental Specialties and Recognition Ronald S Brown*
Brown. Int J Pathol Clin Res 2015, 1:1 ISSN: 2469-5807 International Journal of Pathology and Clinical Research Commentary: Open Access On Emerging Clinical Dental Specialties and Recognition Ronald S Brown* Howard University College of Dentistry, USA *Corresponding author: Ronald S. Brown, DDS, MS, Howard University College of Dentistry, 600 W Street, NW, Rm. 406, Washington, DC 20059, USA, Tel: 202-806-0020, Fax: 202-806-0354, E-mail: [email protected] that I am an oral pathologist or oral surgeon, probably because Oral Keywords & Maxillofacial Surgery and Pathology are ADA-recognized dental Oral medicine, Emerging dental specialties, Specialty recognition specialties. It appears that patients, physicians, and even dentists do not understand the difference between these dental/oral disciplines. Commentary Oral Surgery’s main focus is the surgical management of oral and dental conditions, and Oral Pathology’s main focus is the microscopic Dentistry is mainly a surgical clinical profession and dental evaluation of oral, and dental conditions. There are a number of oral clinicians are primarily involved in the surgical management of medicine clinical areas of concern in which Oral Medicine residents oral diseases and conditions. There are a few American Dental are educated and trained, and none of the ADA-recognized clinical Association (ADA)-recognized non-surgical dental specialties such dental specialty residency programs provide education and training as Oral & Maxillofacial Pathology, Oral & Maxillofacial Radiology, [1]. Furthermore, many of these areas of concern particular to oral and Public Health Dentistry. These non-surgical dental specialties medicine clinicians, are not psychometrically evaluated by the are mainly supportive to the surgical dental specialties and general various ADA recognized clinical specialty boards. -

ADEX DENTAL EXAM SERIES: Fixed Prosthodontics and Endodontics
Developed by: Administered by: The American Board of The Commission on Dental Dental Examiners Competency Assessments ADEX DENTAL EXAM SERIES: Fixed Prosthodontics and Endodontics 2019 CANDIDATE MANUAL Please read all pertinent manuals in detail prior to attending the examination Copyright © 2018 American Board of Dental Examiners Copyright © 2018 The Commission on Dental Competency Assessments Ver 1.1- 2019 Exam Cycle Table of Contents Examination and Manual Overview 2 I. Examination Overview A. Manikin Exam Available Formats 4 B. Manikin Exam Parts 4 C. Endodontic and Prosthodontic Typodonts and Instruments 5 D. Examination Schedule Guidelines 6 1. Dates & Sites 6 2. Timely Arrival 6 E. General Manikin-Based Exam Administration Flow 7 1. Before the Exam: Candidate Orientation 7 2. Exam Day: Sample Schedule 7 3. Exam Day: Candidate Flow 8 F. Scoring Overview and Scoring Content 11 1. Section II. Endodontics Content 12 2. Section III. Fixed Prosthodontics Content 12 G. Penalties 13 II. Standards of Conduct and Infection Control A. Standards of Conduct 15 B. Infection Control Requirements 16 III. Examination Content and Criteria A. Endodontics Examination Procedures 19 B. Prosthodontics Examination Procedures 20 C. Endodontics Criteria 1. Anterior Endodontics Criteria 23 2. Posterior Endodontics Criteria 25 D. Prosthodontics Criteria 1. PFM Crown Preparation 27 2. Cast Metal Crown Preparation 29 3. Ceramic Crown Preparation 31 IV. Examination Forms A. Progress Form 34 See the Registration and DSE OSCE Manual for: • Candidate profile creation and registration • Online exam application process • DSE OSCE registration process and examination information / Prometric scheduling processes • ADEX Dental Examination Rules, Scoring, and Re-test processes 1 EXAMINATION AND MANUAL OVERVIEW The CDCA administers the ADEX dental licensure examination. -

Treatment of a Periodontic-Endodontic Lesion in a Patient with Aggressive Periodontitis
Hindawi Publishing Corporation Case Reports in Dentistry Volume 2016, Article ID 7080781, 9 pages http://dx.doi.org/10.1155/2016/7080781 Case Report Treatment of a Periodontic-Endodontic Lesion in a Patient with Aggressive Periodontitis Mina D. Fahmy,1 Paul G. Luepke,1 Mohamed S. Ibrahim,1,2 and Arndt Guentsch1,3 1 Department of Surgical Sciences, Marquette University School of Dentistry, Milwaukee, WI 53233, USA 2Department of Endodontics, Faculty of Dentistry, Mansoura University, Mansoura 35516, Egypt 3Center of Dental Medicine, Jena University Hospital, Friedrich-Schiller-University, An der Alten Post 4, 07743 Jena, Germany Correspondence should be addressed to Arndt Guentsch; [email protected] Received 7 March 2016; Revised 14 May 2016; Accepted 23 May 2016 Academic Editor: Stefan-Ioan Stratul Copyright © 2016 Mina D. Fahmy et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Case Description. This case report describes the successful management of a left mandibular first molar with acombined periodontic-endodontic lesion in a 35-year-old Caucasian woman with aggressive periodontitis using a concerted approach including endodontic treatment, periodontal therapy, and a periodontal regenerative procedure using an enamel matrix derivate. In spite of anticipated poor prognosis, the tooth lesion healed. This seca report also discusses the rationale behind different treatment interventions. Practical Implication. Periodontic-endodontic lesions can be successfully treated if dental professionals follow a concerted treatment protocol that integrates endodontic and periodontic specialties. General dentists can be the gatekeepers in managing these cases. -

Dental Clinic August 31, 2015
DOD SPACE PLANNING CRITERIA CHAPTER 320: DENTAL CLINIC AUGUST 31, 2015 Originating Component: Defense Health Agency Facilities Division Effective: August 31, 2015 Releasability: No Restrictions Purpose: This issuance: To provide space planning criteria guidance in support of planning, programming and budgeting for DoD Military Health System (MHS) facilities. DoD Space Planning Criteria Chapter 320: Dental Clinic August 31, 2015 TABLE OF CONTENTS SECTION 1: PURPOSE AND SCOPE ............................................................................................. 3 SECTION 2: OPERATING RATIONALE AND BASIS OF CRITERIA ........................................ 4 SECTION 3: PROGRAM DATA REQUIRED............................................................................... 11 3.1. Input Data Statements. ..................................................................................................... 11 SECTION 4: SPACE PLANNING CRITERIA .............................................................................. 12 4.1. FA1: Reception. .............................................................................................................. 12 4.2. FA2: General Dentistry. .................................................................................................. 13 4.3. FA3: Specialty Dentistry................................................................................................. 13 4.4. FA4: Dental Radiography. .............................................................................................. 15 -

Dental Implants Placement of Dental Implants Is a Procedure, Not an American Dental Association (ADA) Recognized Dental Specialty
Dental Implants Placement of dental implants is a procedure, not an American Dental Association (ADA) recognized Dental Specialty. Dental implants like all dental procedures require dental education and training. Implant therapy is a prosthodontic procedure with radiographic and surgical components. Using a dental implant to replace missing teeth is dictated by individual patient needs as determined by their dentist. An implant is a device approved and regulated by the FDA, which can provide support for a single missing tooth, multiple missing teeth, or all teeth in the mouth. The prosthodontic and the surgical part of implant care can each range from straightforward to complex. A General Dentist who is trained to place and restore implants may be the appropriate practitioner to provide care for dental implant procedures. This will vary depending on an individual clinician’s amount of training and experience. However, the General Dentist should know when care should be referred to a specialist (a Prosthodontist, a Periodontist or an Oral and Maxillofacial Surgeon). Practitioners should not try to provide care beyond their level of competence. Orthodontists may place and use implants to enable enhanced tooth movement. Some Endodontists may place an implant when a tooth can’t be successfully treated using endodontic therapy. Maxillofacial Prosthodontists may place special implants or refer for placement when facial tissues are missing and implants are needed to retain a prosthesis. General Dentists are experienced in restorative procedures, and many have been trained and know requirements for the dental implant restorations they provide. However, if a patient’s implant surgical procedure is beyond the usual practice of a dentist, this part of the care should be referred to another dentist that is competent in placement of implants. -

Periogram+/- Vol
Winter 2018 Vol. 1, Issue 1 Periogram+/- From the Desk of Periodontics Chair, Dr. Charles Sfeir Welcome to the first issue of Periogram+/- — the newsletter of the University of Pittsburgh School of Dental Medicine Periodontics and Preventive Dentistry Department. We hope this newsletter brings you current with our exciting developments and up-to-date on the successes of those in our program. We have some great things to share with you in this first issue— such as our newly implemented clinical practice model and our expanding translational research efforts. Our clinical model provides residents with— READ MORE ON PAGE 2 In this issue... Department Chair’s Message Program Director’s Welcome Faculty Focus: Dr. Satish Kumar A Practice-Based Residency Periodontics Research at Pitt Catching Up With 2016 Graduates Our Residency Program, In-Depth Dental Hygiene Program Update A Word from Residency Director, Dr. Kelly Bolden Williams Welcome to the first issue of PerioGram+/-, a newsletter designed to keep University of Pittsburgh School of Dental Medicine periodontics faculty, students and alumni up to date on all that is happening in our program. Our department has always been a great place to work where we can count on everyone to help and pitch in. I am glad to be a part of that and believe that, whether you are a faculty member, — READ MORE ON PAGE 2 Faculty Focus: Dr. Satish Kumar Recognized with an American Academy of Periodontology Outstanding Teaching and Mentor award, Dr. Satish Kumar credits family and mentors with his success. His experience at Pitt, he said, is as supportive as his time at the University of Southern California School of Dentistry, where he studied then taught.