Global HIV Prevention Study to Stop Early After Viiv Healthcare's Long
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Corporate Governance
Strategic report Governance and remuneration Financial statements Investor information Corporate Governance In this section Chairman’s Governance statement 78 The Board 80 Corporate Executive Team 83 Board architecture 85 Board roles and responsibilities 86 Board activity and principal decisions 87 Our purpose, values and culture 90 The Board’s approach to engagement 91 Board performance 94 Board Committee information 96 Our Board Committee reports 97 Section 172 statement 108 Directors’ report 109 GSK Annual Report 2020 77 Chairman’s Governance statement In last year’s Governance statement, I explained that our primary Education and focus on Science objective for 2020 was to ensure there was clarity between the Given the critical importance of strengthening the pipeline, Board and management on GSK’s execution of strategy and its the Board has benefitted from devoting a higher proportion of operational priorities. We have aligned our long-term priorities its time in understanding the science behind our strategy and of Innovation, Performance and Trust powered by culture testing its application. It is important that the Board has a and agreed on the metrics to measure delivery against them. working understanding of the key strategic themes upon The Board’s annual cycle of meetings ensures that all major which our R&D strategy is based. These themes have been components of our strategy are reviewed over the course complemented by Board R&D science thematic deep dives. of the year. Our focus was on the fundamentals of our strategy: human The COVID-19 pandemic impacted and dominated all our genetics, the immune system and AI and ML, as well as to lives for the majority of 2020. -

Long-Acting Cabotegravir: the Future of HIV Prep
Long-Acting Injectable Cabotegravir: the Future of HIV PrEP? Brian R. Wood, MD Associate Professor of Medicine University of Washington Mountain West AIDS Education & Training Center June 4, 2020 Disclosures No conflicts of interest or relationships to disclose. Will be discussing an investigational antiretroviral. Full HPTN 083 study results not yet available. Will be reviewing data from a preliminary DSMB analysis today. See press release and webinar: https://www.hptn.org/news-and-events/announcements/cab- la-proves-be-highly-effective-prevention-hiv-acquisition Outline • General notes about cabotegravir • News from the phase 3 PrEP trial (and why it’s a big deal) • Questions, concerns, and next steps for long-acting PrEP What is Cabotegravir? Cabotegravir (CAB) • Investigational integrase strand transfer inhibitor • Potential infrequent dosing and parenteral administration - Oral half-life: 40 hours - Parenteral nanosuspension (IM, SC) half-life: 21-50 days - Median time from discontinuation to undetectable plasma level (IM, SC): 43-66 weeks • Metabolized by UGT1A1 (main pathway) & UGT1A9 - Minimal CYP metabolism; likely few drug interactions • Relatively low barrier to resistance Aidsinfo.nih.gov/drugs Injectable Long-Acting Cabotegravir Image courtesy of Dr. Raphael Landovitz, UCLA What is the HPTN 083 Trial and What’s the Big News? HPTN 083 A Phase 2b/3 Double Blind Safety and Efficacy Study of Injectable Cabotegravir Compared to Daily Oral TDF/FTC, for Pre-Exposure Prophylaxis in HIV-Uninfected Cisgender Men and TranHPTNsgender Women wh o 083have Sex wi thSites Men – Phase 2b/3 Target enrollment: 4,500 HIV- uninfected cisgender men and transgender 45 Sites in 8 Countrieswomen who have sex with men and who are at risk of HIV acquisition Primary outcome: HIV Prevention effectiveness of cabotegravir compared to daily oral TDF/FTC United States India Vietnam Thailand Peru Brazil South Argentina Africa ClinicalTrials.gov Identifier: NCT02720094 Slide courtesy of Dr. -

PEDIARIX Is a Vaccine
HIGHLIGHTS OF PRESCRIBING INFORMATION • If Guillain-Barré syndrome occurs within 6 weeks of receipt of a prior These highlights do not include all the information needed to use vaccine containing tetanus toxoid, the decision to give PEDIARIX should PEDIARIX safely and effectively. See full prescribing information for be based on potential benefits and risks. (5.2) PEDIARIX. • The tip caps of the prefilled syringes contain natural rubber latex which may cause allergic reactions. (5.3) PEDIARIX [Diphtheria and Tetanus Toxoids and Acellular Pertussis • Syncope (fainting) can occur in association with administration of Adsorbed, Hepatitis B (Recombinant) and Inactivated Poliovirus injectable vaccines, including PEDIARIX. Procedures should be in place Vaccine], Suspension for Intramuscular Injection to avoid falling injury and to restore cerebral perfusion following Initial U.S. Approval: 2002 syncope. (5.4) • If temperature ≥105°F, collapse or shock-like state, or persistent, ----------------------------- INDICATIONS AND USAGE ---------------------------- PEDIARIX is a vaccine indicated for active immunization against diphtheria, inconsolable crying lasting ≥3 hours have occurred within 48 hours after tetanus, pertussis, infection caused by all known subtypes of hepatitis B virus, receipt of a pertussis-containing vaccine, or if seizures have occurred and poliomyelitis. PEDIARIX is approved for use as a 3-dose series in infants within 3 days after receipt of a pertussis-containing vaccine, the decision born of hepatitis B surface antigen (HBsAg)-negative mothers. PEDIARIX to give PEDIARIX should be based on potential benefits and risks. (5.5) may be given as early as 6 weeks of age through 6 years of age (prior to the • For children at higher risk for seizures, an antipyretic may be 7th birthday). -

LATTE Study Oral Cabotegravir + Rilpivirine Versus Efavirenz + 2 NRTI’S LATTE Study: Design
Oral Cabotegravir + Rilpivirine versus Efavirenz + 2 NRTI’s LATTE Study Oral Cabotegravir + Rilpivirine versus Efavirenz + 2 NRTI’s LATTE Study: Design Study Design: CAB 10 mg CAB 10 mg + 2 NRTI’s + RPV 25 mg • BacKground: Phase 2b, (n = 60) (n = 52) randoMized, partially blinded study done at Multiple centers CAB 30 mg CAB 30 mg in the U.S. and Canada + 2 NRTI’s + RPV 25 mg (n = 60) (n = 51) • Inclusion Criteria (n = 244) - Age ≥18 years - Antiretroviral-naïve CAB 60 mg CAB 60 mg - HIV RNA >1,000 copies/ML + 2 NRTI’s + RPV 25 mg - CD4 count >200 cells/MM3 (n = 61) (n = 53) - CrCl >50 ML/Min - No hepatitis B Efavirenz 600 mg Efavirenz 600 mg - No significant transaMinitis + 2 NRTI’s + 2 NRTI’s (n = 62) (n = 46) 24-week lead-in phase Source: Margolis DA, et al. Lancet Infect Dis. 2015;15:1145-55. Oral Cabotegravir + Rilpivirine versus Efavirenz + 2 NRTI’s LATTE Study: Results Cabotegravir + 2NRTIs Cabotegravir + Rilpivirine Efavirenz + 2NRTIs Induction* Maintenance* 100 80 86 82 76 74 71 60 63 40 HIV RNA <50 copies/mL (%) <50 copies/mL HIV RNA 20 156/181 46/62 149/181 44/62 137/181 39/62 0 Week 24 Week 48 Week 96 *Cabotegravir data is composite of all cabotegravir doses Source: Margolis DA, et al. Lancet Infect Dis. 2015;15:1145-55. Oral Cabotegravir + Rilpivirine versus Efavirenz + 2 NRTI’s LATTE Study: Results 100 Induction* Maintenance 80 60 Cabotegravir 10 mg + Rilpivirine 40 Cabotegravir 30 mg + Rilpivirine HIV RNA <40 copies/mL HIV RNA 20 Cabotegravir 60 mg + Rilpivirine Efavirenz 600 mg + 2NRTIs 0 0 12 24 36 48 60 72 84 96 Treatment Week *During induction phase cabotegravir administered with investigator chosen 2NRTIs Source: Margolis DA, et al. -

Final Attendee List
Jennifer Abnet GlaxoSmithKline I GlaxoSmithKline I Jane Arboleda APRN Guardant I Molly Benson Sanjiv Agarwala MD Puma Biotechnology I Cancer Expert Now I Joe Arminger AbbVie I Seth Berkowitz LCSW, Manmeet Ahluwalia MD, CCLS MBA Patricia Armstrong The Leukemia & Lymphoma Miami Cancer Institute I Novartis I Society V Steve Albers Kim Arnold APRN CPNP Barry Berman MD, MS Alexion V CPHON Florida Cancer Specialists I Servier Pharmaceuticals I Maritza Alencar DNP, Tizano Bernard MBA, APRN, BMTCN Sheila Arrington MSN, Cancer Care Centers of Miami Cancer Institute V APRN, NP-C, AOCN Brevard I Puma Biotechnology I Carmen Allen MSIT Ana Mari Bernardini Pharmavoxx V Shannon Ashmon Novartis Oncology I Eisai, Inc I Luly Almeida Bernard Berry MBA Incyte Corporation I Sarah Ashton MS AstraZeneca Pharmaceuticals Guardant Health I I Talat Almukhtar MD Orlando Health Cancer Melissa Austin Jason Bever Institute I Cancer Care Centers of Oncopeptides I Brevard I Beatrice Alvarado Roberts Amy Bignon MD Garland Avera Doyle Caris Life Sciences I University of Florida I Jazz Pharmaceuticals I Nadeem Bilani MD Tadeu Ambros MD Francie Babcock Cleveland Clinic I FCS I AMAG Pharmaceuticals/Covis I Angela Bilik RN BSN Douglas Anderson AstraZeneca I Incyte Corporation I Craig Bailey Astra Zeneca I Jamie Bilsky BS Blesson Andrews Genentech V Genentech I Kevin Barr Daiichi Sankyo I Rohit Bishnoi MD Ollie Annum PharmD University of Florida I BHMCR I Leonard Bennett PharmD EMD Serono I Brady Blackman Susmitha Apuri MD MorphoSys I Florida Cancer Specialists I Michael Bennett As of 4-22-21 Kimberly Blandon RN MSN Rick Breitenstein Memorial Cancer Institute I Apellis Pharmaceuticals I Denise Capo Karyopharm Therapeutics I Taryn Boiteau GlaxoSmithKline I Amanda Bridges Florida Society of Clinical Heidi Caravetta Tracy Bonds RN, BSN, Oncology I Exelixis, Inc. -

GLAXOSMITHKLINE LLC V. TEVA PHARMACEUTICALS USA, INC
Case: 18-1976 Document: 111 Page: 1 Filed: 10/02/2020 United States Court of Appeals for the Federal Circuit ______________________ GLAXOSMITHKLINE LLC, SMITHKLINE BEECHAM (CORK) LIMITED, Plaintiffs-Appellants v. TEVA PHARMACEUTICALS USA, INC., Defendant-Cross-Appellant ______________________ 2018-1976, 2018-2023 ______________________ Appeals from the United States District Court for the District of Delaware in No. 1:14-cv-00878-LPS-CJB, Chief Judge Leonard P. Stark. ______________________ Decided: October 2, 2020 ______________________ JUANITA ROSE BROOKS, Fish & Richardson, PC, San Diego, CA, argued for plaintiffs-appellants. Also represented by MICHAEL ARI AMON, CRAIG E. COUNTRYMAN, JONATHAN ELLIOT SINGER; ELIZABETH M. FLANAGAN, MICHAEL J. KANE, WILLIAM WOODFORD, Minneapolis, MN; DOUGLAS E. MCCANN, Wilmington, DE. WILLIAM M. JAY, Goodwin Procter LLP, Washington, DC, argued for defendant-cross-appellant. Also represented by JAIME ANN SANTOS; ELAINE BLAIS, J. Case: 18-1976 Document: 111 Page: 2 Filed: 10/02/2020 2 GLAXOSMITHKLINE LLC v. TEVA PHARMACEUTICALS USA, INC. ANTHONY DOWNS, ROBERT FREDERICKSON, III, CHRISTOPHER T. HOLDING, ALEXANDRA LU, LANA S. SHIFERMAN, DARYL L. WIESEN, Boston, MA; IRA J. LEVY, New York, NY. HANSJORG SAUER, Biotechnology Innovation Organization, Washington, DC, for amicus curiae Biotechnology Innovation Organization. Also represented by MELISSA A. BRAND; BRIAN PAUL BARRETT, Eli Lilly and Company, Indianapolis, IN. MICHAEL N. KENNEDY, Covington & Burling LLP, Washington, DC, for amicus curiae Pharmaceutical Research and Manufacturers of America. Also represented by STEVEN JOHN WINKELMAN; DAVID EVAN KORN, Pharmaceutical Research and Manufacturers Association of America, Washington, DC. ANDREW CURTIS NICHOLS, Winston & Strawn LLP, Washington, DC, for amicus curiae Association for Accessible Medicines. Also represented by GEORGE C. -

Declarations of Interest Thorax: First Published As 10.1136/Thoraxjnl-2016-209333.476 on 15 November 2016
Declarations of interest Thorax: first published as 10.1136/thoraxjnl-2016-209333.476 on 15 November 2016. Downloaded from KF Rabe reports financial for support for consultancy work P297 LUNG-FUNCTION PROFILE BEFORE AND AFTER THE from AstraZeneca, Chiesi, Novartis, MSD and GlaxoSmithKline, FIRST MODERATE TO SEVERE EXACERBATION DURING and grants from Altana, Novartis, AstraZeneca, MSD and THE WISDOM STUDY Nycomed. F Maltais reports financial support from Boehringer Ingelheim 10.1136/thoraxjnl-2016-209333.476 during the conduct of the study and, outside of the submitted work, financial support from Boehringer Ingelheim and GlaxoS- E Wouters, outside of the submitted work, reports personal fees mithKline for attendance at advisory boards, financial support from AstraZeneca, GlaxoSmithKline, Novartis, Takeda, Pfizer from Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca and and Boehringer Ingelheim, and grants from AstraZeneca, GlaxoS- Novartis for speaking activities, and research support from Boeh- mithKline and Novartis. ringer Ingelheim, GlaxoSmithKline, AstraZeneca, Nycomed and H Magnussen received funding from Almirall, AstraZeneca, Novartis. Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Merck, Novar- tis, Takeda and Roche to conduct clinical studies, and has spoken at meetings and is a member of advisory boards for these and P295 EFFICACY AND SAFETY OF TIOTROPIUM/OLODATEROL other companies. IN PATIENTS WITH COPD BY ATS CATEGORY R Rodriguez-Roisin reports personal fees from AstraZeneca, Boehringer Ingelheim, Mylan, Pearl Therapeutics, Takeda, Teva 10.1136/thoraxjnl-2016-209333.474 and Ferrer, and grants and personal fees from Menarini and Almirall. F Maltais reports financial support from Boehringer Ingelheim K Tetzlaff and S Bell are employees of Boehringer Ingelheim during the conduct of the study and, outside of the submitted Pharma GmbH & Co. -
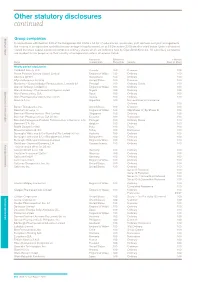
Other Statutory Disclosures Continued
Other statutory disclosures continued Strategic reportGroup companies Governance & remuneration Financial statements In accordance with Section 409 of the Companies Act 2006 a full list of subsidiaries, associates, joint ventures and joint arrangements, the country of incorporation and effective percentage of equity owned, as at 31 December 2015 are disclosed below. Unless otherwise stated the share capital disclosed comprises ordinary shares which are indirectly held by GlaxoSmithKline plc. All subsidiary companies are resident for tax purposes in their country of incorporation unless otherwise stated. Country of Effective % % Held by Name incorporation Ownership Security Class of Share Wholly owned subsidiaries 1506369 Alberta ULC Canada 100 Common 100 Action Potential Venture Capital Limited England & Wales 100 Ordinary 100 Adechsa GmbH Switzerland 100 Ordinary 100 Affymax Research Institute United States 100 Common 100 Alenfarma – Especialidades Farmaceuticas, Limitada (iv) Portugal 100 Ordinary Quota 100 Allen & Hanburys Limited (iv) England & Wales 100 Ordinary 100 Allen & Hanburys Pharmaceutical Nigeria Limited Nigeria 100 Ordinary 100 Allen Farmaceutica, S.A. Spain 100 Ordinary 100 Allen Pharmazeutika Gesellschaft m.b.H. Austria 100 Ordinary 100 Aners S.A (iv) Argentina 100 Non-endorsable Nominative Ordinary 100 Barrier Therapeutics, Inc. United States 100 Common 100 Beecham Group p l c England & Wales 100 20p Shares 'A'; 5p Shares B 100 Beecham Pharmaceuticals (Pte) Limited Singapore 100 Ordinary 100 Beecham Pharmaceuticals S.A (iv) (vi) Ecuador 100 Nominative 100 Beecham Portuguesa-Produtos Farmaceuticos e Quimicos, Lda Portugal 100 Ordinary Quota 100 Beecham S.A. (iv) Belgium 100 Ordinary 100 Biddle Sawyer Limited India 100 Equity 100 Biovesta Ilaçlari Ltd. Sti. Turkey 100 Nominative 100 Burroughs Wellcome & Co (Australia) Pty Limited (iv) (vi) Australia 100 Ordinary 100 Burroughs Wellcome & Co (Bangladesh) Limited Bangladesh 100 Ordinary 100 Burroughs Wellcome International Limited England & Wales 100 Ordinary 100 Caribbean Chemical Company, Ltd. -

(KPIC) PPO and Out-Of- Area Indemnity (OOA) Drug Formulary with Specialty Drug Tier
Kaiser Permanente Insurance Company (KPIC) PPO and Out-of- Area Indemnity (OOA) Drug Formulary with Specialty Drug Tier This Drug Formulary was updated: September 1, 2021 NOTE: This drug formulary is updated often and is subject to change. Upon revision, all previous versions of the drug formulary are no longer in effect. This document contains information regarding the drugs that are covered when you participate in the California Nongrandfathered PPO and Out-of- Area Indemnity (OOA) Health Insurance Plans with specialty drug tier offered by Kaiser Permanente Insurance Company (KPIC) and fill your prescription at a MedImpact network pharmacy. Access to the most current version of the Formulary can be obtained by visiting kp.org/kpic-ca-rx-ppo-ngf. For help understanding your KPIC insurance plan benefits, including cost sharing for drugs under the prescription drug benefit and under the medical benefit, please call 1-800-788-0710 or 711 (TTY) Monday through Friday, 7a.m. to 7p.m. For help with this Formulary, including the processes for submitting an exception request and requesting prior authorization and step therapy exceptions, please call MedImpact 24 hours a day, 7 days a week, at 1-800-788-2949 or 711 (TTY). For cost sharing information for the outpatient prescription drug benefits in your specific plan, please visit: kp.org/kpic-ca-rx-ppo-ngf. For help in your preferred language, please see the Kaiser Permanente Insurance Company Notice of Language Assistance in this document. KPIC PPO NGF Table of Contents Informational Section................................................................................................................................2 -

Glaxosmithkline Plc Annual Report for the Year Ended 31St December 2000
GlaxoSmithKline 01 GlaxoSmithKline plc Annual Report for the year ended 31st December 2000 Contents Report of the Directors 02 Financial summary 03 Joint statement by the Chairman and the Chief Executive Officer 05 Description of business 29 Corporate governance 37 Remuneration report 47 Operating and financial review and prospects 69 Financial statements 70 Directors’ statements of responsibility 71 Report by the auditors 72 Consolidated statement of profit and loss 72 Consolidated statement of total recognised gains and losses 74 Consolidated statement of cash flow 76 Consolidated balance sheet 76 Reconciliation of movements in equity shareholders’ funds 77 Company balance sheet 78 Notes to the financial statements 136 Group companies 142 Principal financial statements in US$ 144 Financial record 153 Investor information 154 Shareholder return 156 Taxation information for shareholders 157 Shareholder information 158 Share capital 160 Cross reference to Form 20-F 162 Glossary of terms The Annual Report was approved by the Board 163 Index of Directors on 22nd March 2001 and published on 12th April 2001. Contact details 02 GlaxoSmithKline Financial summary 2000 1999 Increase Business performance £m £m CER % £ % Sales 18,079 16,164 9 12 Trading profit 5,026 4,378 12 15 Profit before taxation 5,327 4,708 11 13 Earnings/Net income 3,697 3,222 13 15 Earnings per Ordinary Share 61.0p 52.7p 14 16 Total results Profit before taxation 6,029 4,236 Earnings/Net income 4,154 2,859 Earnings per Ordinary Share 68.5p 46.7p Business performance: results exclude merger items and restructuring costs; 1999 sales and trading profit exclude the Healthcare Services businesses which were disposed of in 1999. -

Antivirals: HIV –Cabotegravir/Rilpivirine (Cabenuva) Medical Policy No
Antivirals: HIV –Cabotegravir/rilpivirine (Cabenuva) Medical policy no. 12.10.99.AB-1 Effective Date: June 1, 2021 Related medical policies: • 12.10.99 Antivirals- HIV Combinations • 12.10.99.AA Antivirals – HIV: emtricitabine-tenofovir (Descovy) Note: New-to-market drugs included in this class based on the Apple Health Preferred Drug List (AHPDL) are non-preferred and subject to this prior authorization (PA) criteria. Non-preferred agents in this class require an inadequate response or documented intolerance due to severe adverse reaction or contraindication to at least ONE preferred regimen. If a drug within this policy receives a new indication approved by the Food and Drug Administration (FDA), medical necessity for the new indication will be determined on a case-by-case basis following FDA labeling. To see the list of the current AHPDL, please visit: https://www.hca.wa.gov/assets/billers-and-providers/apple-health-preferred-drug-list.xlsx Before authorization of Cabenuva will be approved, documentation from TheraCom specialty pharmacy showing the patient has been established on Vocabria must be included. Documentation must include patient’s name, patient’s date of birth, NDC, quantity/days supply, and date patient received the medication. TheraCom Pharmacy contact information: TheraCom Mailing Address: TheraCom VIIV Specific Team numbers (Used to locate TheraCom in e-Prescribing systems) Phone: 1-844-276-6299 TheraCom Fax: 1-833-904-1881 345 International Blvd Ste 200 Brooks, KY 40109 Background: Human immunodeficiency virus (HIV) is a single-stranded RNA retrovirus that attacks the immune system, specifically CD4+ T-helper cells, causing a progressive decrease in CD4+ T cell count and increased susceptibility of a person to infections. -

ESG Performance Summary 2020 About This Report
ESG Performance Summary 2020 About this report In this report: Trust is one of our three long-term priorities Our commitments 1 and is essential to how we achieve our purpose, Data summary 2 drive long-term growth and add value for society SASB index 17 United Nations Global Compact and our shareholders. Communication on Progress 20 Global Reporting Initiative We have 13 commitments that support About our reporting guidelines 25 our Trust priority and drive progress in the This document provides a comprehensive Assurance report 30 key areas where we can make a significant summary of environmental, social and Public policies available online 32 impact, and ensure that we are running our governance (ESG) data from across our business in a responsible way. business. This complements our wider reporting on responsible business in our These commitments seek to address Annual Report where we report progress In our Annual Report: the most material topics relevant to on our 13 Trust commitments and in the Stakeholder engagement our stakeholders and to our business, responsible business pages of gsk.com. Progress against our Trust commitments and are designed to help us respond Climate change resilience (TCFD) to challenges and opportunities within our industry and society more broadly. Other online reporting: They contribute to many of the UN Materiality assessment Sustainable Development Goals, and Human rights as a science-led, global healthcare Sustainable Development Goals company, our biggest contribution is Political advocacy towards Goal 3: ensure healthy lives Patient group funding and promote well-being for all at all ages. Trade association memberships Charitable grant contributions Cautionary statement Criteria for working with Public Policy Groups See page 32 of this document for the cautionary statement regarding forward-looking statements.