A Review of Oculoplastic Photography: a Guide for Clinician Photographers
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Beyond Snapshots: How to Take That Fancy Dslr Camera Off Auto and Photograph Your Life Like a Pro Pdf, Epub, Ebook
BEYOND SNAPSHOTS: HOW TO TAKE THAT FANCY DSLR CAMERA OFF AUTO AND PHOTOGRAPH YOUR LIFE LIKE A PRO PDF, EPUB, EBOOK Rachel Devine, Peta Mazey | 224 pages | 14 Jun 2012 | Watson-Guptill Publications | 9780817435806 | English | New York, United States Beyond Snapshots: How to Take That Fancy DSLR Camera Off Auto and Photograph Your Life Like a Pro PDF Book If you tend to shoot indoors, you may want to consider also investing in a faster lens. Although it is not the first photography book I have read, I still feel like I learned a lot. If you're just starting out, you don't want to spend thousands of dollars on a camera and lenses you might never use. This is from the 'situations' section where I present 5-minute primers for common situations. They're quick and easy to master, and once you know them, you'll never forget them. While it has many of the same features as its predecessor the D , including a They consist of a camera body to which interchangeable lenses can be added. The touch-screen is clear and bright, and the layout of the menus and options available makes things simple to navigate. You heard that right! The Sony Cyber-shot RX10 IV is a premium super-zoom all-in-one bridge camera with a megapixel 1- inch sensor and a long-range mm equivalent zoom, all packed into a robust, ergonomic body. Silhouettes are all about shape and contrast, so pay special attention to these details. I'd never thought about taking shots after the sun has set. -

The Musk Duck Photography Special
The Musk Duck Photography Special Compiled by Ian Ashton November 2020 Chaffinch 1977 UK England, Mamiya SLR and 135mm prime lens with extension tubes. Ian Ashton Here we are in November 2020 and most of Birdlife Ballarat’s planned syllabus meetings and outings have been cancelled including this year’s photography competition due to the Pandemic. I was to give a talk back in June, it was titled, ‘How times have changed’, an old-fashioned slide show. So, in place of that and to acknowledge that some of our members are not just bird watchers, this Musk Duck photography special was conceived. Birdlife Ballarat does not have a dedicated photography group, but many members do own cameras. It may be that in these uncertain times some members have contemplated buying a camera or upgrading their equipment or their knowledge. I thought it would be good to share some ideas and techniques. Left, my very first SLR was a Mamiya 500 like this one. The 500 related to the shutter speed, 1,500th of a second. My present camera can take photos at 1,4000th Of a second. Times and technology have changed. MD Photo Special Birdwatching and bird photography do not always sit well together, but of course most birdwatchers enjoy seeing photographs of birds. At one end we have the birdwatcher and at the other end the photographer and between these two ends there are as many combinations of the two as you can imagine. The best bird photographers know their subject and can have immense amounts of knowledge and patience to achieve the outcome they are aiming for. -
Megaplus Conversion Lenses for Digital Cameras
Section2 PHOTO - VIDEO - PRO AUDIO Accessories LCD Accessories .......................244-245 Batteries.....................................246-249 Camera Brackets ......................250-253 Flashes........................................253-259 Accessory Lenses .....................260-265 VR Tools.....................................266-271 Digital Media & Peripherals ..272-279 Portable Media Storage ..........280-285 Digital Picture Frames....................286 Imaging Systems ..............................287 Tripods and Heads ..................288-301 Camera Cases............................302-321 Underwater Equipment ..........322-327 PHOTOGRAPHIC SOLUTIONS DIGITAL CAMERA CLEANING PRODUCTS Sensor Swab — Digital Imaging Chip Cleaner HAKUBA Sensor Swabs are designed for cleaning the CLEANING PRODUCTS imaging sensor (CMOS or CCD) on SLR digital cameras and other delicate or hard to reach optical and imaging sur- faces. Clean room manufactured KMC-05 and sealed, these swabs are the ultimate Lens Cleaning Kit in purity. Recommended by Kodak and Fuji (when Includes: Lens tissue (30 used with Eclipse Lens Cleaner) for cleaning the DSC Pro 14n pcs.), Cleaning Solution 30 cc and FinePix S1/S2 Pro. #HALCK .........................3.95 Sensor Swabs for Digital SLR Cameras: 12-Pack (PHSS12) ........45.95 KA-11 Lens Cleaning Set Includes a Blower Brush,Cleaning Solution 30cc, Lens ECLIPSE Tissue Cleaning Cloth. CAMERA ACCESSORIES #HALCS ...................................................................................4.95 ECLIPSE lens cleaner is the highest purity lens cleaner available. It dries as quickly as it can LCDCK-BL Digital Cleaning Kit be applied leaving absolutely no residue. For cleaing LCD screens and other optical surfaces. ECLIPSE is the recommended optical glass Includes dual function cleaning tool that has a lens brush on one side and a cleaning chamois on the other, cleaner for THK USA, the US distributor for cleaning solution and five replacement chamois with one 244 Hoya filters and Tokina lenses. -

Photographers Guide to the Nikon Coolpix P600 Ebook
PHOTOGRAPHERS GUIDE TO THE NIKON COOLPIX P600 PDF, EPUB, EBOOK Alexander S White | 424 pages | 01 Jun 2014 | White Knight Press | 9781937986254 | English | none Photographers Guide to the Nikon Coolpix P600 PDF Book Software Manuals Firmware Software. Moreover, I enjoy landscape photography with my Nikon camera. Sign in. Step 1 Tripod Mount. Although your device does not support this download service, it can be used to view download information. Disappointingly the P still doesn't support the RAW file format, something that all of its main competitors offer, and a prosumer feature that frankly we'd expect on this class of camera. And mostly all apps are accessible from Android to iPhone users. Necessary Always Enabled. We've combed through the options and selected our two favorite cameras in this class. The book explains all shooting modes, menus, functions, and controls of this superzoom camera in clear language, accompanied by more than illustrations and sample photographs. Baby Blues Mobile Lightroom Presets. Just list the features most important to you like 4k video, fully automatic mode, etc. Nikon retain ownership of the Manual and all copies thereof and all related intellectual property rights, and reserves all rights not expressly granted to you under this Agreement. Cancel: I did not complete this guide. The shutter release, zoom lever and power button are in the same locations as on the P, as is the same customisable Function button. This camera has a 35x optical zoom lens with macro capability. Not to mention, it has high-quality features and allows you to add a creative spin to your photography. -
Tiny Bridge Camera That's Simple, Fun and Connected
Tiny bridge camera that’s simple, fun and connected Effortlessly capture beautiful detail with this versatile 45x zoom mini-bridge camera. Superb photos and HD movies are a breeze to shoot and share with Smart Auto, easy connectivity and fun creative modes. • A tiny, bridge-style camera that’s easy to carry and Product Range use with a big 45x zoom to capture distant detail • Enjoy exceptional images of your best memories, PowerShot SX60 HS thanks to 20.0 Megapixels, DIGIC 4+ and Intelligent PowerShot SX540 HS Image Stabilizer PowerShot SX430 IS • Connect to your smart device with Wi-Fi and NFC for easy sharing or back up of your creations and remote PowerShot SX60 HS shooting • Point and shoot for fantastic results using Smart Auto and fun creative modes. Add a date stamp to your memories • Record superb HD movies (720p) with one touch of a button, while a Dynamic Image Stabilizer keeps PowerShot SX540 HS footage steady * Wi-Fi connectivity and features vary by model and region. PowerShot SX430 IS Technical Specifications IMAGE SENSOR SHOOTING Type 1/2.3 type CCD Modes Smart Auto (32 scenes detected), Program AE, Live View [14] Effective Pixels Approx. 20.0M Control, Portrait, Face Self-Timer, Low Light (5.0MP), Monochrome, Fish-eye Effect, Toy Camera Effect, Effective / Total Pixels Approx. 20.5M Miniature Effect, Super Vivid, Poster Effect, Fireworks, Long Shutter IMAGE PROCESSOR Photo Effects My Colors (My Colors Off, Vivid, Neutral, Sepia, Black & Type DIGIC 4+ White, Positive Film, Lighter Skin Tone, Darker Skin Tone, Vivid Blue, Vivid Green, Vivid Red, Custom Color) LENS Drive modes Single, Continuous, Self-Timer Focal Length 4.3 – 193.5 mm (35 mm equivalent: 24 – 1080 mm) Continuous Shooting Approx. -
How Digital Cameras Capture Light
1 Open Your Shutters How Digital Cameras Capture Light Avery CirincioneLynch Eighth Grade Project Paper Hilltown Cooperative Charter School June 2014 2 Cover image courtesy of tumblr.com How Can I Develop This: Introduction Imagine you are walking into a dark room; at first you can't see anything, but as your pupils begin to dilate, you can start to see the details and colors of the room. Now imagine you are holding a film camera in a field of flowers on a sunny day; you focus on a beautiful flower and snap a picture. Once you develop it, it comes out just how you wanted it to so you hang it on your wall. Lastly, imagine you are standing over that same flower, but, this time after snapping the photograph, instead of having to developing it, you can just download it to a computer and print it out. All three of these scenarios are examples of capturing light. Our eyes use an optic nerve in the back of the eye that converts the image it senses into a set of electric signals and transmits it to the brain (Wikipedia, Eye). Film cameras use film; once the image is projected through the lens and on to the film, a chemical reaction occurs recording the light. Digital cameras use electronic sensors in the back of the camera to capture the light. Currently, there are two main types of sensors used for digital photography: the chargecoupled device (CCD) and complementary metaloxide semiconductor (CMOS) sensors. Both of these methods convert the intensity of the light at each pixel into binary form, so the picture can be displayed and saved as a digital file (Wikipedia, Image Sensor). -
WCPHA Newsletter March 2016
WCPHA Newsletter March 2016 Next meeting (at the library again this month) The next WCPHA meeting will be held in the Terry Salman Library 4575 Clancy Loranger Way Vancouver, BC V5Y 2M4 (off 33rd Ave between Cambie and Main) on Wednesday 2nd March 2016 starting at 7:15 pm. Secretary’s Message AGM Please note that our AGM will be held at the May meeting. Formal notice will follow but please advise me if you have any items for the agenda. VANCOUVER CAMERA SHOW. Sunday April 24th 2016 at the usual Cameron Centre location in Burnaby. Siggi or Brigitte will be pleased to reserve you a table 604 941-0300 or [email protected] BRIDGE CAMERAS The Minolta article below introduces a series of digital bridge cameras— for people who wanted a big, expensive and showy hunk of plastic—without interchangeable lenses. However the bridge camera was introduced two decades earlier for 35mm film. It joined the Kodak Disk and the APS formats of that period as a near disaster. It did not sell. At the next meeting I will bring one of these and a mess of accessories—it was supposed to become a “system” camera. If you have one, bring it along for show and tell. THE COLLECTOR Minolta Cameras Part Two. APS format cameras Minolta also invested heavily in APS (Advanced Photo System) film-format cameras, most notably with the Vectis line of SLR cameras beginning in 1996. APS later proved to be a technological dead end, as the cameras did not sell as hoped. Digital photography was entering the marketplace, and Minolta eventually discontinued all APS camera production. -

700 $400 $400 $200 $400 $400
BLACK FRIDAY From November 29 to December 5, 2019 SALE Best DSLR Camera BONUS Mount Adapter EF-EOS R $ o 4K Value 130 + D W PE ITH IP U Q E N O VR I V T IB C RA DU o TION RE o EOS RP Body D3500 / AF-P 18-55 VR + AF-P 70-300 VR The mirrorless EOS RP – the lightest and Reg. 99 99 Easy to use as a point and 99 1699 most compact full-frame EOS camera to date. 99 Reg. 999 shoot with DSLR quality. Works $ includes a 26.2 MP CMOS sensor, the World’s $ seamlessly with compatible 1299 Save 400 fastest autofocus, 4K video, and our powerful 599 Save 400 smart phone. Built-in bluetooth DIGIC 8 processor. plus compact and durable. BONUS AF-S NIKKOR 50mm f/1.8 G 4K Value $249 Best Mirrorless CSC Enthusiast o EOS M50 / 15-45mm IS STM D750 Body 99 99 Nikon’s entry level full-frame DSLR 6.5 o Reg. 1099 24.1 MP CMOS (APS-C) sensor. 99 Reg. 2299 FPS top shutter rate. Weather and dust 99 Improved Dual Pixel CMOS AF, Eye sealing for tougher conditions. Higher ISO $ $ 699 Save 400 Detection AF. 4K UHD 24p and HD 1599 Save 700 for low light photography. Includes tilting 120p for slow motion. vari-angle LCD. Best Full Frame Camera Expert BONUS FTZ Mount Adapter 4K Value $329 o Lumix ZS60 Z 6 Body The Nikon Z 6 is a 24.5 MP full-frame 99 mirrorless camera that features a new Reg. -

How to Choose the Right Camera Choosing the Best Camera Could Be Difficult As There Are Numerous Options Available in the Market with a Slew of Features
C O V E r S t O r Y How to Choose the Right Camera Choosing the best camera could be difficult as there are numerous options available in the market with a slew of features. Usually, people look for long zoom and high megapixels, but there are many other key specs that you should look for - Ashok Pandey rom sensors to focal length, light sensitivity to shortest and longest focal lengths. Thus, when the spec is types of view-finders, there’s a lot of to check listed as 18-55mm f3.5-5.6 that means the widest aperture in cameras than mega-pixels. Here we decipher is f3.5 at 18mm and f5.6 at 55mm. As aperture size Fsome of the features in digital cameras and how increases, the area of sharpness in front of and behind the to determine what’s right for you. subject increases. The area of sharpness is called depth of Sensor size - This refers to the dimensions of the array the field. Since wider apertures let in more light and give of photo-receptors that create the pixels that become an you more control over depth of field, wider is better. image. Bigger sensors produce better photo quality. The Resolution - Typically referred as megapixels, the bigger the sensor, the bigger the camera, larger lens and MP number tells you how many pixels the camera uses more space for supporting electronics. Larger sensors are to produce an image. Every modern camera has more also more expensive to make, so the cameras are pricier. -

COOLPIX P950 Bridge Camera Packs an Incredible 83X Optical Zoom (2000 Mm RECOMMENDED ACCESSORIES Equivalent) Into a Robust Body
REACH FURTHER The COOLPIX P950 bridge camera packs an incredible 83x optical zoom (2000 mm RECOMMENDED ACCESSORIES equivalent) into a robust body. Whether you’re at the airshow or on safari, you can shoot more and miss less. FEATURES Incredible zoom The focal length range of 24–2000 mm takes you to the heart of every scene. The 166x Dynamic Fine Zoom digitally extends the upper zoom limit to an incredible 4000 mm.1 Fast NIKKOR lens DOT SIGHT DF-M1 The bright NIKKOR lens with f/2.8 maximum aperture delivers great results. Super ED glass helps reduce distortion at high zoom. RAW image capture The COOLPIX P950 supports RAW (NRW) image capture, so you can edit with high-quality files. Vari-angle TFT LCD monitor BLUETOOTH® REMOTE CONTROL You can tilt and twist the large LCD monitor in almost any direction. Or you can use the ML-L7 clear 2359k-dot OLED electronic viewfinder. Thrilling 4K superzoom movies Easily record stereo 4K/UHD 30p footage, or Full HD (1080p) video at frame rates of up to 60p. Movie Manual mode lets you adjust key exposure settings while filming: ideal in changing light. In-camera time-lapse Record magical time-lapse movies of approx. 10 seconds duration. Perfect for showing skyscapes, star trails, or plants opening in a forest glade. ME-W1 WIRELESS MICROPHONE Accessory ready Mount Nikon Speedlights and mics on the full-size hot shoe. Or try Nikon’s DF-M1 Dot Sight, a foldable scope that helps you track even fast-flying birds and keep them in the centre of the frame. -
1 Depth of Field / Aperture Depth of Field Refers to the Range of Distance
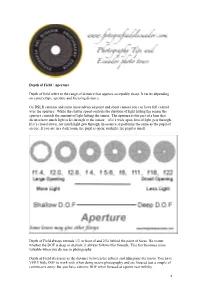
Depth of Field / Aperture Depth of field refers to the range of distance that appears acceptably sharp. It varies depending on camera type, aperture and focusing distance. On DSLR cameras and some more advanced point and shoot camera you can have full control over the aperture. While the shutter speed controls the duration of light hitting the sensor the aperture controls the amount of light hitting the sensor. The aperture is the part of a lens that dictates how much light is let through to the sensor – if it’s wide open, lots of light gets through. If it’s closed down, not much light gets through. In essence, it performs the same as the pupil of an eye. If you are in a dark room, the pupil is open; sunlight, the pupil is small. Depth of Field always extends 1/3 in front of and 2/3s behind the point of focus. No matter whether the DOF is deep or shallow, it always follows this formula. This fact becomes more valuable when you do macro photography. Depth of Field decreases as the distance between the subject and film plane decreases. You have VERY little DOF to work with when doing macro photography and are focused just a couple of centimeters away, but you have extreme DOF when focused at a point near infinity. 1 Different lenses can have different apertures – for example, a cheaper lens may only open to f4.0, not letting in as much light as a more expensive lens that will open to f1.6 or more. -
Challenge Accepted
Florida’s Outlook On the dental Laboratory profession 3rd Quarter 2018 www.fdla.net Challenge Accepted Focus_3rd2018.indd 1 7/3/2018 2:26:31 PM By M. reed Cone, dMd, MS, Cdt, FACp 1 Digital Dental Photography: Techniques and Tips for the Laboratory Technician t first glance, the world of digital dental photography may seem overwhelming and intimidating, especially for those individuals without much experience behind the camera. Fortunately, all that is necessary to begin making excellent photographs are a few pieces of inexpensive equipment, a handful of core skills, a little practice and just a bit of imagination. than a point and shoot model or a prosumer/ Photographic Equipment bridge camera with a zoom lens permanently fixed Camera Body in place (Figure 1). A DSLR camera will provide greater flexibility and control over the settings The first piece of equipment that needs to be as well as allow for a wider variety of lenses and acquired is the camera body. There are several flash accessories to be attached. To achieve the brands to choose from, and the most popular highest resolution possible, a camera body with Figure 1 (above) are Canon, Nikon, and Sony. The company which a full-frame sensor should be selected for dental Camera Types: makes the camera is not very important since most photography. Not only is the rendering of color Introductory level point contemporary digital cameras today are capable exceptionally accurate, but the final image on a and shoot, advanced of producing high-quality images. The type of full-frame sensor camera does not suffer from the beginner level prosumer/ camera matters more, and it is important to spend cropping that occurs with the diminutive APS-C bridge, and professional sensor format cameras (Figure 2).