A Microcomputed Tomographic Evaluation of Root Canal Morphology of Maxillary Second Premolars in a Pakistani Cohort
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Maxillary Premolars
Maxillary Premolars Dr Preeti Sharma Reader Oral & Maxillofacial Pathology SDC Dr. Preeti Sharma, Subharti Dental College, SVSU Premolars are so named because they are anterior to molars in permanent dentition. They succeed the deciduous molars. Also called bicuspid teeth. They develop from the same number of lobes as anteriors i.e., four. The primary difference is the well-formed lingual cusp developed from the lingual lobe. The lingual lobe is represented by cingulum in anterior teeth. Dr. Preeti Sharma, Subharti Dental College, SVSU The buccal cusp of maxillary first premolar is long and sharp assisting the canine as a prehensile or tearing teeth. The second premolars have cusps less sharp and function as grinding teeth like molars. The crown and root of maxillary premolar are shorter than those of maxillary canines. The crowns are little longer and roots equal to those of molars. Dr. Preeti Sharma, Subharti Dental College, SVSU As the cusps develop buccally and lingually, the marginal ridges are a little part of the occlusal surface of the crown. Dr. Preeti Sharma, Subharti Dental College, SVSU Maxillary second premolar Dr. Preeti Sharma, Subharti Dental College, SVSU Maxillary First Premolar Dr Preeti Sharma Reader Oral Pathology SDC Dr. Preeti Sharma, Subharti Dental College, SVSU The maxillary first premolar has two cusps, buccal and lingual. The buccal cusp is about 1mm longer than the lingual cusp. The crown is angular and buccal line angles are more prominent. The crown is shorter than the canine by 1.5 to 2mm on an average. The premolar resembles a canine from buccal aspect. -
Root Canal Configuration and Root Wall Thickness of First Maxillary
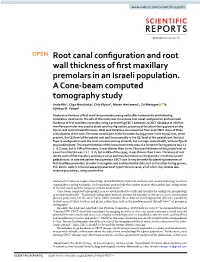
www.nature.com/scientificreports OPEN Root canal confguration and root wall thickness of frst maxillary premolars in an Israeli population. A Cone-beam computed tomography study Anda Kfr1, Olga Mostinsky1, Orly Elyzur1, Moran Hertzeanu1, Zvi Metzger 1* & Ajinkya M. Pawar2 Anatomical features of frst maxillary premolars may greatly afect endodontic and following restorative treatments. The aim of this study was to evaluate root canal confguration and root wall thickness of frst maxillary premolars using a preexisting CBCT database. A CBCT database of 400 frst maxillary premolar was used to study canal confguration, presence of furcation-facing groove on the buccal root and root wall thickness. Root wall thickness was measured from axial CBCT slices at three critical points of the root: The most coronal part of the furcation-facing groove in the buccal root, when present, the CEJ level of the palatal root and 5 mm apically to the CEJ level of the palatal root. Vertucci Type IV confguration was the most common among all teeth, but in single-rooted teeth, Vertucci Type II was predominant. The mean thickness of the buccal root in the area of a furcation-facing groove was 1.1 (±0.2) mm, but in 39% of the cases, it was thinner than 1 mm. The mean thickness of the palatal root at 5 mm from the CEJ was 1.1 (±0.2), but in 28% of the cases, it was thinner than 1 mm. Thickness of root dentin walls of frst maxillary premolars varies and may be limited at critical points in both buccal and palatal roots. -

Anterior and Posterior Tooth Arrangement Manual
Anterior & Posterior Tooth Arrangement Manual Suggested procedures for the arrangement and articulation of Dentsply Sirona Anterior and Posterior Teeth Contains guidelines for use, a glossary of key terms and suggested arrangement and articulation procedures Table of Contents Pages Anterior Teeth .........................................................................................................2-8 Lingualized Teeth ................................................................................................9-14 0° Posterior Teeth .............................................................................................15-17 10° Posterior Teeth ...........................................................................................18-20 20° Posterior Teeth ...........................................................................................21-22 22° Posterior Teeth ..........................................................................................23-24 30° Posterior Teeth .........................................................................................25-27 33° Posterior Teeth ..........................................................................................28-29 40° Posterior Teeth ..........................................................................................30-31 Appendix ..............................................................................................................32-38 1 Factors to consider in the Aesthetic Arrangement of Dentsply Sirona Anterior Teeth Natural antero-posterior -
CHAPTER 5Morphology of Permanent Molars
CHAPTER Morphology of Permanent Molars Topics5 covered within the four sections of this chapter B. Type traits of maxillary molars from the lingual include the following: view I. Overview of molars C. Type traits of maxillary molars from the A. General description of molars proximal views B. Functions of molars D. Type traits of maxillary molars from the C. Class traits for molars occlusal view D. Arch traits that differentiate maxillary from IV. Maxillary and mandibular third molar type traits mandibular molars A. Type traits of all third molars (different from II. Type traits that differentiate mandibular second first and second molars) molars from mandibular first molars B. Size and shape of third molars A. Type traits of mandibular molars from the buc- C. Similarities and differences of third molar cal view crowns compared with first and second molars B. Type traits of mandibular molars from the in the same arch lingual view D. Similarities and differences of third molar roots C. Type traits of mandibular molars from the compared with first and second molars in the proximal views same arch D. Type traits of mandibular molars from the V. Interesting variations and ethnic differences in occlusal view molars III. Type traits that differentiate maxillary second molars from maxillary first molars A. Type traits of the maxillary first and second molars from the buccal view hroughout this chapter, “Appendix” followed Also, remember that statistics obtained from by a number and letter (e.g., Appendix 7a) is Dr. Woelfel’s original research on teeth have been used used within the text to denote reference to to draw conclusions throughout this chapter and are the page (number 7) and item (letter a) being referenced with superscript letters like this (dataA) that Treferred to on that appendix page. -

Endodontic Treatment of a Maxillary First Premolar with an Unusual Working Length: a Clinical Case Report
dical C Me as d e n R a e l p Sulaiman and Adebayo, Clin Med Case Rep 2018, 2:2 a o c r i t n s i l C Clinical and Medical Case Reports Case Report Open Access Endodontic Treatment of a Maxillary First Premolar with an Unusual Working Length: A Clinical Case Report Omotayo Sulaiman and Gbenga Adebayo* Department of restorative dentistry, University College Hospital, Ibadan, Nigeria Abstract Purpose: To report a clinical case of unusually long maxillary first premolar submitted to non- surgical endodontic treatment. Case presentation: A 32 year old male patient that presented on account of severe toothache in upper right quadrant of 3 weeks duration. His medical history was not contributory. Clinical examination revealed no soft tissue abnormality in relation to the tooth, however there was distooclusal carious lesion which affected less than one third of the crown of the maxillary right first premolar. There was severe tenderness to digital percussion. Periapical radiograph showed unusually long tooth 14 with coronal radiolucency communicating with the pulp, there was minimal periapical radiolucency and widening of periodontal ligament space. Diagnosis of apical periodontitis secondary to class II dental caries was made and patient planned for root canal treatment with subsequent Porcelain Fused to metal crown. Anaesthesia was achieved by infiltration technique using (2% lidocaine 1:100,000 adrenalin) and access cavity made on tooth 14 after appropriate isolation. Palatal and buccal canals were located and working length determined by tactile method confirmed radiographically to be 29 mm and 28 mm respectively which required using the longest files 31 mm available for the biomechanical preparation. -

Maxillary Bilateral Canine-Premolar Transposition: a Rare Condition
Open Access Journal of Dentistry & Oral Disorders Case Report Maxillary Bilateral Canine-Premolar Transposition: A Rare Condition Agarwala P1, Agarwal V1, Rekhade R1 and Kulshrestha R2* Abstract 1Department of Orthodontics and Dentofacial Tooth transposition is very rare developmental phenomena in which Orthopaedics, Haldia Institute of Dental Sciences & the adjacent teeth are switched or have their positions changed with one Research, India another and due to this aesthetical and functional problem may be present. 2Consulting Orthodontist, Private Practice, Mumbai, The maxillary permanent canine is the tooth most frequently transposed, and India it is often transposed with the first premolar followed by the lateral incisor and *Corresponding author: Rohit Kulshrestha, lastly the central incisor in very rare cases. Several etiologic factors may lead Consulting Orthodontist, Private Practice, Mumbai, to transposition like genetics, developing tooth buds displacement, mechanical India interferences, trauma and early loss of incisors. This paper reports a case of bilateral transposition in the maxillary arch involving the first premolar and Received: March 28, 2017; Accepted: May 11, 2017; canine. Published: May 18, 2017 Keywords: Ectopic eruption; Maxillary canine; Tooth transposition Introduction interchanged positions between maxillary first premolar and canine on both right and the left sides (Figure 2). Upper left deciduous canine Tooth transposition is defined as the positional interchange in was still present and it showed decalcification on its labial aspect. spatial area of two adjacent teeth including their roots, or eruption Remaining teeth in all the other quadrants were at normal location and development of a tooth in a position normally occupied by a with normal morphology, overjet and overbite. -

Age and Sequence of Permanent Canine and Premolar Teeth Eruption in 102-174 Months Old Children in Kerman Province
Current Research in Dentistry 1 (1): 6-10, 2010 ISSN 1949-0119 © 2010 Science Publications Age and Sequence of Permanent Canine and Premolar Teeth Eruption in 102-174 Months Old Children in Kerman Province Farokhgissor Elham and Shahrzad Adhamy Department of Peadiatric Dentistry, Kerman University of Medical Science, Iran Abstract: Problem statement: The aim of this study was to investigate the eruption time of permanent canine and premolar teeth in 8.5-14.5 years (102-174 months) old boys and girls of Kerman province. Approach: The sample for this cross-sectional study consisted of 2602, 102-174 months old (8.5-14.5 years old) children form 56 primary and guidance schools in Kerman which were scattered over in 2 districts of the city. There were 1556 of girls and 1046 of boys were chosen by simple randomization and the emergence stage of each tooth was recorded. Results: The analysis indicated significantly earlier emergence ages in girls than in boys. The eruption pattern turned out to be symmetric in both sexes and no statically significant difference was detected between the right and left side. The most common observed emergence pattern in girls was mandibular canine and maxillary first premolar followed by mandibular first premolar, maxillary second premolar, then mandibular second premolar and canine and in boys it was maxillary and mandibular first premolar, mandibular canine, maxillary second premolar, mandibular second premolar and maxillary canine Conclusion: Significantly earlier emergence ages in girls seen than in boys. The sequence of eruption differs between girls and boys for mandibular canine and first premolar. -

Bilateral Maxillary Canine-First Premolar Transposition in Permanent Dentition Sarwat Memon and Mubassar Fida
CASE REPORT Bilateral Maxillary Canine-First Premolar Transposition in Permanent Dentition Sarwat Memon and Mubassar Fida ABSTRACT Transposition is a dental anomaly characterized by the exchange of position between two adjacent teeth, especially in relation to their roots, or development and eruption of a tooth in a position normally occupied by a nonadjacent tooth. Transposition of the maxillary canine and first premolar has a low prevalence in the population and it primarily affects maxillary canines and premolars. The aetiology of the transposition remains unclear, although it has been associated with genetic factors. It may also be related to a combination of localised factors such as malformation of adjacent teeth, tooth agenesis, retention of the deciduous canine and a history of local trauma. If uncorrected, the results are often both functionally and esthetically unsatisfactory. This case report presents treatment of a female patient with complete bilateral transposition of maxillary canine and premolar. The patient was treated orthodontically with non-extraction fixed mechanotherapy by simulation of maxillary first premolar as canine bilaterally. Key Words: Bilateral maxillary canine-first premolar. Transposition. Permanent dentition. INTRODUCTION and lower labial segment crowding, crossbite of upper Transposition is defined as an interchange in the right lateral incisor with right lower canine, overjet of position of two teeth within the same quadrant of the 3 mm and overbite of 4 mm (Figure 1 and 2). dental arch. Maxillary canine-premolar transposition Cephalometric analysis showed a mild skeletal Class-III (MxC.P1) is the most frequent transposition and relationship (ANB angle = -1°) with low vertical the incidence is reported to be 0.135 - 0.510%.1 proportions (FMA = 17°). -

Geometric Analysis of Maxillary First Premolar Prepared by Two Nickel
JCDP Dina Al-Sudani et al 10.5005/jp-journals-10024-1510 ORIGINAL ARTICLE Geometric Analysis of Maxillary First Premolar Prepared by Two Nickel-Titanium Rotary Instruments 1Dina Al-Sudani, 2Majed Almalki, 3Saad Al-Shahrani, 4Michael Ahlquist ABSTRACT Prepared by Two Nickel-Titanium Rotary Instruments. J Contemp Dent Pract 2014;15(2):174-180. Aim: The present study was conducted with the aim of evalua- ting and comparing the shaping ability of two Nickel-titanium Source of support: Nil rotary instruments, with two disparate design features, on root Conflict of interest: None canal geometry of extracted human maxillary first premolars using microcomputed tomography. INTRODUCTION Study design: Twenty four bifurcated maxillary first premolars were divided into two groups and embedded in a rubber-based Intra-radicular microbial infection has been shown to be the impression material. Both groups were submitted to micro- main cause of apical periodontitis.1-3 Therefore, the goal of computed tomography before and after canal preparation root canal treatment is to eliminate or reduce the number (buccal and palatal) with either ProFile Vortex or Revo-S rotary instruments. Images were reconstructed and cross-sections of microorganisms to a level that will allow healing of the 4 corresponding to a distance 1, 2, 3, 4, 5, 6, and 7 mm from periapical tissues and to prevent microbial reinfection. This the anatomical apex were selected for canal transportation process involves chemomechanical cleaning and shaping as analysis. Volume changes were also measured. well as obturation of the root canal system. Results: The degree and direction of canal transportation were Root canal preparation is essential for removing necrotic non-significant for both instruments. -
Access Cavity Pictures.Pdf
PLATE 1 Outline Form A. A standard radiograph (left) in buccolingual pro- triangular preparation in a youngster reflects pul- jection provides only a two-dimensional view of pal horn extension and size of the pulp chamber, what is actually a three-dimensional problem. If a whereas ovoid preparation in an adult relates to a mesiodistal x-ray projection could be made grossly receded pulp. Extension toward the incisal (right), one would find the pulp of the maxillary allows central-axis access for instruments. second premolar to be flat tapering “ribbon” rather E. Large size and shape of coronal preparation in a than round “thread” visualized on the initial radi- recently calcified incisor relate to huge pulp hous- ograph. The final ovoid occlusal cavity preparation ing. To remove all pulp remnants and to accom- (F) will mirror the internal anatomy rather than modate large endodontic instruments and filling the buccolingual x-ray image. materials, coronal preparation must be an exten- B. Coronal preparation of a maxillary first molar sive, triangular, funnel-shaped opening. Actually, illustrating the major principle of endodontic cav- no more than the lingual wall of pulp chamber has ity outline form: the internal anatomy of the tooth been removed. In lower incisors, the outline form (pulp) dictates the external outline form. This is may well be extended into the incisal edge. This accomplished by extending preparation from preparation allows absolutely direct access to apex. inside of the tooth to the outside surface, that is, F. The outline form of the endodontic coronal cavity working from inside to outside. -
1 – Introduction to Dental Anatomy
1 Introduction to Dental Anatomy LEARNING OBJECTIVES 5. Which of the following terms represents the surface of a tooth that is facing toward an adjoining tooth in the same dental arch? 1. Correctly define and pronounce the nomenclature (terms) A. Occlusal as emphasized in the bold type in this and each following B. Incisal chapter. C. Facial 2. Be able to identify each tooth of the primary and permanent D. Proximal dentitions using the Universal, Palmer, and Fédération Den- For additional study resources, please visit Expert Consult. taire Internationale (FDI) systems. 3. Correctly name and identify the surfaces, ridges, and ana- Dental anatomy is defined here as, but is not limited to, the study tomic landmarks of each tooth. of the development, morphology, function, and identity of each of 4. Understand and describe the methods used to measure ante- the teeth in the human dentitions, as well as the way in which the rior and posterior teeth. teeth relate in shape, form, structure, color, and function to the 5. Learn the tables of measurements and be able to discuss size other teeth in the same dental arch and to the teeth in the oppos- comparisons between the teeth from any viewing angle. A ing arch. Thus the study of dental anatomy, physiology, and occlu- useful skill at this point is to start illustrating the individual sion provides one of the basic components of the skills needed to teeth with line drawings. practice all phases of dentistry. The application of dental anatomy to clinical practice can be envisioned in Fig. 1.1A, where a faulty crown form has resulted in esthetic and periodontal problems that may be corrected by an appropriate restorative dental treatment, such as that illustrated in Fig. -

First Premolar Extraction Decisions and Effects Ryan Gregory Bowles University of Tennessee Health Science Center
University of Tennessee Health Science Center UTHSC Digital Commons Theses and Dissertations (ETD) College of Graduate Health Sciences 5-2005 First Premolar Extraction Decisions and Effects Ryan Gregory Bowles University of Tennessee Health Science Center Follow this and additional works at: https://dc.uthsc.edu/dissertations Part of the Orthodontics and Orthodontology Commons Recommended Citation Bowles, Ryan Gregory , "First Premolar Extraction Decisions and Effects" (2005). Theses and Dissertations (ETD). Paper 30. http://dx.doi.org/10.21007/etd.cghs.2005.0034. This Thesis is brought to you for free and open access by the College of Graduate Health Sciences at UTHSC Digital Commons. It has been accepted for inclusion in Theses and Dissertations (ETD) by an authorized administrator of UTHSC Digital Commons. For more information, please contact [email protected]. First Premolar Extraction Decisions and Effects Document Type Thesis Degree Name Master of Dental Science (MDS) Program Orthodontics Research Advisor Edward Harris, Ph.D. Committee Gregory Hutchins, D.D.S. Quinton Robinson, D.D.S., M.S. DOI 10.21007/etd.cghs.2005.0034 This thesis is available at UTHSC Digital Commons: https://dc.uthsc.edu/dissertations/30 FIRST PREMOLAR EXTRACTION DECISIONS AND EFFECTS A Thesis Presented for The Graduate Studies Council The University of Tennessee Health Science Center In Partial Fulfillment Of the Requirements for the Degree Master of Dental Science From The University of Tennessee By Ryan Gregory Bowles, D.D.S. May 2005 Copyright © Ryan Gregory Bowles, 2005 All rights reserved ii DEDICATION This thesis is dedicated to my parents Dr. Richard Matteson Bowles and Mrs. Sharon White Bowles in recognition of their love, guidance and support of my education iii ACKNOWLEDGMENTS I would like to thank my thesis committee for their help and support over these last three years.