Chapter 21: the Thigh, Hip, Groin, and Pelvis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Corporate Medical Policy Surgery for Groin Pain in Athletes
Corporate Medical Policy Surgery for Groin Pain in Athletes File Name: surgery_for_groin_pain_in_athletes Origination: 8/2014 Last CAP Review: 6/2020 Next CAP Review: 6/2021 Last Review: 6/2020 Description of Procedure or Service Sports-related groin pain, commonly known as athletic pubalgia or sports hernia, is characterized by disabling activity-dependent lower abdominal and groin pain that is not attributable to any other cause. Athletic pubalgia is most frequently diagnosed in high-performance male athletes, particularly those who participate in sports that involve rapid twisting and turning such as soccer, hockey, and football. Alternative names include Gilmore’s groin, osteitis pubis, pubic inguinal pain syndrome, inguinal disruption, slap shot gut, sportsmen’s groin, footballers groin injury complex, hockey groin syndrome, athletic hernia, sports hernia and core muscle injury. For patients who fail conservative therapy, surgical repair of any defects identified in the muscles, tendons or nerves has been proposed. Groin pain in athletes is a poorly defined condition, for which there is not a consensus regarding the cause and/or treatment. Some believe the groin pain is an occult hernia process, a prehernia condition, or an incipient hernia, with the major abnormality being a defect in the transversalis fascia, which forms the posterior wall of the inguinal canal. Another theory is that injury to soft tissues that attach to or cross the pubic symphysis is the primary abnormality. The most common of these injuries is thought to be at the insertion of the rectus abdominis onto the pubis, with either primary or secondary pain arising from the adductor insertion sites onto the pubis. -

Pelvic Anatomyanatomy
PelvicPelvic AnatomyAnatomy RobertRobert E.E. Gutman,Gutman, MDMD ObjectivesObjectives UnderstandUnderstand pelvicpelvic anatomyanatomy Organs and structures of the female pelvis Vascular Supply Neurologic supply Pelvic and retroperitoneal contents and spaces Bony structures Connective tissue (fascia, ligaments) Pelvic floor and abdominal musculature DescribeDescribe functionalfunctional anatomyanatomy andand relevantrelevant pathophysiologypathophysiology Pelvic support Urinary continence Fecal continence AbdominalAbdominal WallWall RectusRectus FasciaFascia LayersLayers WhatWhat areare thethe layerslayers ofof thethe rectusrectus fasciafascia AboveAbove thethe arcuatearcuate line?line? BelowBelow thethe arcuatearcuate line?line? MedianMedial umbilicalumbilical fold Lateralligaments umbilical & folds folds BonyBony AnatomyAnatomy andand LigamentsLigaments BonyBony PelvisPelvis TheThe bonybony pelvispelvis isis comprisedcomprised ofof 22 innominateinnominate bones,bones, thethe sacrum,sacrum, andand thethe coccyx.coccyx. WhatWhat 33 piecespieces fusefuse toto makemake thethe InnominateInnominate bone?bone? PubisPubis IschiumIschium IliumIlium ClinicalClinical PelvimetryPelvimetry WhichWhich measurementsmeasurements thatthat cancan bebe mademade onon exam?exam? InletInlet DiagonalDiagonal ConjugateConjugate MidplaneMidplane InterspinousInterspinous diameterdiameter OutletOutlet TransverseTransverse diameterdiameter ((intertuberousintertuberous)) andand APAP diameterdiameter ((symphysissymphysis toto coccyx)coccyx) -

Systematic Approach to the Interpretation of Pelvis and Hip
Volume 37 • Number 26 December 31, 2014 Systematic Approach to the Interpretation of Pelvis and Hip Radiographs: How to Avoid Common Diagnostic Errors Through a Checklist Approach MAJ Matthew Minor, MD, and COL (Ret) Liem T. Bui-Mansfi eld, MD After participating in this activity, the diagnostic radiologist will be better able to identify the anatomical landmarks of the pelvis and hip on radiography, and become familiar with a systematic approach to the radiographic interpretation of the hip and pelvis using a checklist approach. initial imaging examination for the evaluation of hip or CME Category: General Radiology Subcategory: Musculoskeletal pelvic pain should be radiography. In addition to the com- Modality: Radiography plex anatomy of the pelvis and hip, subtle imaging fi ndings often indicating signifi cant pathology can be challenging to the veteran radiologist and even more perplexing to the Key Words: Pelvis and Hip Anatomy, Radiographic Checklist novice radiologist given the paradigm shift in radiology residency education. Radiography of the pelvis and hip is a commonly ordered examination in daily clinical practice. Therefore, it is impor- tant for diagnostic radiologists to be profi cient with its inter- The initial imaging examination for the evaluation pretation. The objective of this article is to present a simple of hip or pelvic pain should be radiography. but thorough method for accurate radiographic evaluation of the pelvis and hip. With the advent of cross-sectional imaging, a shift in residency training from radiography to CT and MR imag- Systematic Approach to the Interpretation of Pelvis ing has occurred; and as a result, the art of radiographic and Hip Radiographs interpretation has suffered dramatically. -

Applied Anatomy of the Hip RICARDO A
Applied Anatomy of the Hip RICARDO A. FERNANDEZ, MHS, PT, OCS, CSCS • Northwestern University The hip joint is more than just a ball-and- bones fuse in adults to form the easily recog- socket joint. It supports the weight of the nized “hip” bone. The pelvis, meaning bowl head, arms, and trunk, and it is the primary in Latin, is composed of three structures: the joint that distributes the forces between the innominates, the sacrum, and the coccyx pelvis and lower extremities.1 This joint is (Figure 1). formed from the articu- The ilium has a large flare, or iliac crest, Key PointsPoints lation of the proximal superiorly, with the easily palpable anterior femur with the innomi- superior iliac spine (ASIS) anterior with the The hip joint is structurally composed of nate at the acetabulum. anterior inferior iliac spine (AIIS) just inferior strong ligamentous and capsular compo- The joint is considered to it. Posteriorly, the crest of the ilium ends nents. important because it to form the posterior superior iliac spine can affect the spine and (PSIS). With respect to surface anatomy, Postural alignment of the bones and joints pelvis proximally and the PSIS is often marked as a dimple in the of the hip plays a role in determining the femur and patella skin. Clinicians attempting to identify pelvic functional gait patterns and forces associ- distally. The biomechan- or hip subluxations, leg-length discrepancies, ated with various supporting structures. ics of this joint are often or postural faults during examinations use There is a relationship between the hip misunderstood, and the these landmarks. -

2019 Radiology Cpt Codes
2019 RADIOLOGY CPT CODES BONE DENSITOMETRY 1 Bone Density/DEXA 77080 CT 1 CT Abd & Pelvis W/ Contrast 74177 1 CT Enterography W/ Contrast 74177 1 CT Max/Facial W/O Contrast 70486 # CT Sinus Complete W/O Contrast 70486 1 CT Abd & Pelvis W W/O Contrast 74178 1 CT Extremity Lower W/ Contrast 73701 1 CT Neck W/ Contrast 70491 # CT Sinus Limited W/O Contrast 76380 1 CT Abd & Pelvis W/O Contrast 74176 1 CT Extremity Lower W/O Contrast 73700 1 CT Neck W/O Contrast 70490 # CT Spine Cervical W/ Contrast 72126 1 CT Abd W/ Contrast 74160 1 CT Extremity Upper W/ Contrast 73201 1 CT Orbit/ IAC W/ Contrast 70481 # CT Spine Cervical W/O Contrast 72125 1 CT Abd W/O Contrast 74150 1 CT Extremity Upper W/O Contrast 73200 1 CT Orbit/ IAC W/O Contrast 70480 # CT Spine Lumbar W/ Contrast 72132 1 CT Abd W W/O Contrast 74170 1 CT Head W/ Contrast 70460 1 CT Orbit/ IAC W W/O Contrast 70482 # CT Spine Lumbar W/O Contrast 72131 1 CT Chest W/ Contrast 71260 1 CT Head W/O Contrast 70450 1 CT Pelvis W/ Contrast 72193 # CT Spine Thoracic W/ Contrast 72129 1 CT Chest W/O Contrast 71250 1 CT Head W W/O Contrast 70470 1 CT Pelvis W/O Contrast 72192 # CT Spine Thoracic W/O Contrast 72128 1 CT Chest W W/O Contrast 71270 1 CT Max/Facial W/ Contrast 70487 1 CT Pelvis W W/O Contrast 72194 # CT Stone Protocol W/O Contrast 74176 CTA 1 Cardiac Calcium Score only 75571 1 CT Angiogram Abd & Pelvis W W/O Contrast 74174 1 CT Angiogram Head W W/O Contrast 70496 # CT / CTA Heart W Contrast 75574 1 CT Angiogram Abdomen W W/O Contrast 74175 1 CT Angiogram Chest W W/O Contrast 71275 -

Groin and Buttock Claudication Associated with Vascular Origin Due to Chronic Occlusion of Internal Iliac Artery -A Case Report
Anesth Pain Med 2015; 10: 93-96 http://dx.doi.org/10.17085/apm.2015.10.2.93 ■Case Report■ Groin and buttock claudication associated with vascular origin due to chronic occlusion of internal iliac artery -A case report- Departments of Anesthesiology and Pain Medicine, *Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University College of † Medicine, Seoul, Ire Pain Clinic, Incheon, Korea Hyun Mo Chung, Sang-Soo Kang, Keun-Man Shin, Sang-hoon Lee, Sung Eun Kim*, and Hong-Seong Yoo† Neurogenic and vascular claudication is sometimes difficult to When concomitant symptoms such as radiating pain are distinguish from each other due to similarities in symptoms. present, a herniated disc could be considered first [3]. We Symptoms and physical examinations may not always match the report a rare case of severe groin pain of vascular origin, severity in both diseases, and when atypical symptoms, such as groin pain, are present, diagnosis can be more challenging. Proper associated with mild pain in the buttock and lower leg, differential diagnosis of the two is important because of the without the typical vascular symptoms due to well developed invasiveness of treatment in both diseases. We report a rare case collateral flow of abdominal wall vessels. of a patient with severe groin and buttock pain due to chronic occlusion of the internal iliac artery, along with a review of the relevant literature. (Anesth Pain Med 2015; 10: 93-96) CASE REPORT Key Words: Claudication, Groin, Internal iliac artery, Pain. A 70-year-old male with persistent bilateral groin pain, more severe on the left, visited our department of pain medicine. -

Sportsmans Groin: the Inguinal Ligament and the Lloyd Technique
Rennie, WJ and Lloyd, DM. Sportsmans Groin: The Inguinal Ligament and the Lloyd Technique. Journal of the Belgian Society of Radiology. 2017; 101(S2): 16, pp. 1–4. DOI: https://doi.org/10.5334/jbr-btr.1404 OPINION ARTICLE Sportsmans Groin: The Inguinal Ligament and the Lloyd Technique WJ Rennie and DM Lloyd Groin pain is a catch all phrase used to define a common set of symptoms that affect many individuals. It is a common condition affecting sportsmen and women (1, 2) and is often referred to as the sportsman groin (SG). Multiple surgical operations have been developed to treat these symptoms yet no definitive imaging modalities exist to diagnose or predict prognosis. This article aims to discuss the anatomy of the groin, suggest a biomechanical pathophysiology and outline a logical surgical solution to treat the underlying pathology. A systematic clinical and imaging approach with inguinal ligament and pubic specific MRI assessment, can result in accurate selection for intervention. Close correlation with clinical examination and imaging in series is recommended to avoid misinterpretation of chronic changes in athletes. Keywords: Groin pain; Inguinal Ligament; MRI; Surgery; Lloyd release Introduction from SG is due to altered biomechanics, with specific pain Groin pain is a catch all phrase used to define a common symptoms that differ from those caused by inguinal or set of symptoms that affect many individuals. It is a com- femoral hernias. mon condition affecting sportsmen and women [1, 2] and is often referred to as the sportsman groin (SG). Multiple Anatomy of Sportsman’s Groin surgical operations have been developed to treat these The anatomical central structure in the groin is the pubic symptoms, yet no definitive imaging modalities exist to bone. -

Femoral Injecting Guide
FEMORAL INJECTING A GUIDE TO INJECTING IN THE GROIN USING THE FEMORAL VEIN (This is a restricted document NOT meant for general distribution) AUGUST 2006 1 INTRODUCTION INTRODUCTION This resource has been produced by some older intravenous drug users (IDU’s) who, having compromised the usual injecting sites, now inject into the femoral vein. We recognize that many IDU’s continue to use as they grow older, but unfortunately, easily accessible injecting sites often become unusable and viable sites become more dif- ficult to locate. Usually, as a last resort, committed IDU’s will try to locate one of the larger, deeper veins, especially when injecting large volumes such as methadone. ManyUnfortunately, of us have some had noof usalternat had noive alternative but to ‘hit butand to miss’ ‘hit andas we miss’ attempted as we attemptedto find veins to find that weveins couldn’t that we see, couldn’t but knew see, werebut knew there. were This there. was often This painful,was often frustrating, painful, frustrating, costly and, costly in someand, cases,in some resulted cases, inresulted permanent in permanent injuries such injuries as the such example as the exampleshown under shown the under the heading “A True Story” on pageheading 7. “A True Story” on page 7. CONTENTS CONTENTS 1) Introduction, Introduction, Contents contents, disclaimer 9) Rotating Injecting 9) Rotating Sites Injecting Sites 2) TheFemoral Femoral Injecting: Vein—Where Getting is Startedit? 10) Blood Clots 10) Blood Clots 3) FemoralThe Femoral Injecting: Vein— Getting Where -

Sir Ganga Ram Hospital Classification of Groin and Ventral Abdominal Wall Hernias
Symposium Sir Ganga Ram Hospital classification of groin and ventral abdominal wall hernias Pradeep K Chowbey, Rajesh Khullar, Magan Mehrotra, Anil Sharma, Vandana Soni, Manish Baijal Minimal Access and Bariatric Surgery Centre, Sir Ganga Ram Hospital, New Delhi - 110 060, India Address for correspondence: Pradeep K. Chowbey, Minimal Access and Bariatric Surgery Centre, Room No. 200 (2nd floor), Sir Ganga Ram Hospital, New Delhi - 110 060, India. E-mail: [email protected] Abstract of all ventral hernias of the abdomen. The system proposed by us includes all abdominal wall hernias and Background: Numerous classifications for groin is a final classification that predicts the expected level and ventral hernias have been proposed over the of difficulty for an endoscopic hernia repair. past five to six decades. The old, simple classification of groin hernia in to direct, inguinal Key words: Total extraperitoneal repair, SGRH classification, and femoral components is no longer adequate to laparoscopic ventral hernia repair understand the complex pathophysiology and management of these hernias.The most commonly followed classification for ventral hernias divide CLASSIFICATION SYSTEMS FOR GROIN HERNIA them into congenital, acquired, incisional and traumatic, which also does not convey any Numerous classifications for groin hernia have been information regarding the predicted level of difficulty. proposed over the past five to six decades. The old Aim: All the previous classification systems were based on open hernia repairs and have their own simple classification of groin hernia into indirect and fallacies particularly for uncommon hernias that direct, inguinal and femoral components is no longer cannot be classified in these systems. With the adequate to understand the complex advent of laparoscopic/ endoscopic approach, pathophysiology and management of these hernias.[1] surgical access to the hernia as well as the In the 1950s and 1960s, many surgical classifications functional anatomy viewed by the surgeon changed. -

Clinical Pelvic Anatomy
SECTION ONE • Fundamentals 1 Clinical pelvic anatomy Introduction 1 Anatomical points for obstetric analgesia 3 Obstetric anatomy 1 Gynaecological anatomy 5 The pelvic organs during pregnancy 1 Anatomy of the lower urinary tract 13 the necks of the femora tends to compress the pelvis Introduction from the sides, reducing the transverse diameters of this part of the pelvis (Fig. 1.1). At an intermediate level, opposite A thorough understanding of pelvic anatomy is essential for the third segment of the sacrum, the canal retains a circular clinical practice. Not only does it facilitate an understanding cross-section. With this picture in mind, the ‘average’ of the process of labour, it also allows an appreciation of diameters of the pelvis at brim, cavity, and outlet levels can the mechanisms of sexual function and reproduction, and be readily understood (Table 1.1). establishes a background to the understanding of gynae- The distortions from a circular cross-section, however, cological pathology. Congenital abnormalities are discussed are very modest. If, in circumstances of malnutrition or in Chapter 3. metabolic bone disease, the consolidation of bone is impaired, more gross distortion of the pelvic shape is liable to occur, and labour is likely to involve mechanical difficulty. Obstetric anatomy This is termed cephalopelvic disproportion. The changing cross-sectional shape of the true pelvis at different levels The bony pelvis – transverse oval at the brim and anteroposterior oval at the outlet – usually determines a fundamental feature of The girdle of bones formed by the sacrum and the two labour, i.e. that the ovoid fetal head enters the brim with its innominate bones has several important functions (Fig. -

DEPARTMENT of ANATOMY IGMC SHIMLA Competency Based Under
DEPARTMENT OF ANATOMY IGMC SHIMLA Competency Based Under Graduate Curriculum - 2019 Number COMPETENCY Objective The student should be able to At the end of the session student should know AN1.1 Demonstrate normal anatomical position, various a) Define and demonstrate various positions and planes planes, relation, comparison, laterality & b) Anatomical terms used for lower trunk, limbs, joint movement in our body movements, bony features, blood vessels, nerves, fascia, muscles and clinical anatomy AN1.2 Describe composition of bone and bone marrow a) Various classifications of bones b) Structure of bone AN2.1 Describe parts, blood and nerve supply of a long bone a) Parts of young bone b) Types of epiphysis c) Blood supply of bone d) Nerve supply of bone AN2.2 Enumerate laws of ossification a) Development and ossification of bones with laws of ossification b) Medico legal and anthropological aspects of bones AN2.3 Enumerate special features of a sesamoid bone a) Enumerate various sesamoid bones with their features and functions AN2.4 Describe various types of cartilage with its structure & a) Differences between bones and cartilage distribution in body b) Characteristics features of cartilage c) Types of cartilage and their distribution in body AN2.5 Describe various joints with subtypes and examples a) Various classification of joints b) Features and different types of fibrous joints with examples c) Features of primary and secondary cartilaginous joints d) Different types of synovial joints e) Structure and function of typical synovial -
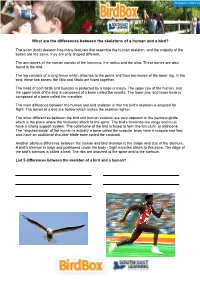
What Are the Differences Between the Skeletons of a Human and a Bird?
What are the differences between the skeletons of a human and a bird? The avian (bird) skeleton has many features that resemble the human skeleton, and the majority of the bones are the same, they are only shaped different. The arm bones of the human consist of the humerus, the radius and the ulna. These bones are also found in the bird. The leg consists of a long femur which attaches to the pelvis and then two bones of the lower leg. In the bird, these two bones: the tibia and fibula are fused together. The head of both birds and humans is protected by a large cranium. The upper jaw of the human, and the upper beak of the bird is composed of a bone called the maxilla. The lower jaw, and lower beak is composed of a bone called the mandible. The main difference between the human and bird skeleton is that the bird's skeleton is adapted for flight. The bones of a bird are hollow which makes the skeleton lighter. The other differences between the bird and human skeleton are very apparent in the pectoral girdle, which is the place where the forelimbs attach to the spine. The bird's forelimbs are wings and must have a strong support system. The collarbone of the bird is fused to form the furculum, or wishbone. The "shoulderblade" of the human is actually a bone called the scapula, birds have a scapula and they also have an additional shoulder blade bone called the corocoid. Another obvious difference between the human and bird skeleton is the shape and size of the sternum.