'Ig-6---4C Clerk
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
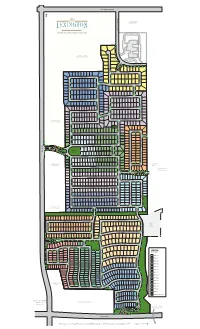
Lexington Phases Mastermap RH HR 3-24-17
ELDORADO PARKWAY MAMMOTH CAVE LANE CAVE MAMMOTH *ZONED FUTURE LIGHT RETAIL MASTER PLANNED GATED COMMUNITY *ZONED FUTURE RETAIL/MULTI-FAMILY MAJESTIC PRINCE CIRCLE MAMMOTH CAVE LANE T IN O P L I A R E N O D ORB DRIVE ARISTIDES DRIVE MACBETH AVENUE MANUEL STREETMANUEL SPOKANE WAY DARK STAR LANE STAR DARK GIACOMO LANE CARRY BACK LANE 7 8 NORTHERN DANCER WAY GALLAHADION WAY GRINDSTONE MANOR GRINDSTONE FUNNY CIDE COURT FUNNY THUNDER GULCH WAY BROKERS TIP LANE MANUEL STREETMANUEL E PLAC RAL DMI WAR A DAY STAR WAY *ZONED FUTURE 3 LIGHT COMMERCIAL BOLD FORBES STREET FERDINAND TRAIL LEONATUS LANE LEONATUS PONDER LANE SEATTLE SLEW STREET GRAHAM AVENUE WINTERGREEN DRIVE COIT ROAD COIT SECRETARIAT BOULEVARD COUNT TURF COUNT DRIVE AMENITY SMARTY JONES STREET CENTER STRIKE GOLD BOULEVARD 2 DEBONAIR LANE LUCKY 5 CAVALCADE DRIVE CAVALCADE 1 Yucca Ridge *ZONED FUTURE FLYING EBONY STREET LIGHT RETAIL Park AFFIRMED AVENUE Independence High School SUTHERLAND LANE AZRA TRAIL OMAHA DRIVE BOLD VENTURE AVENUE CONQUISTADOR COURT CONQUISTADOR LUCKY DEBONAIR LANE LUCKY OXBOW AVENUE OXBOW CAVALCADE DRIVE CAVALCADE 4 WHIRLAWAY DRIVE 9 IRON LIEGE DRIVE *ZONED FUTURE IRON LIEGE DRIVE LIGHT COMMERCIAL 6 A M EMPIRE MAKER ROAD E RISEN STAR ROAD R I BUBBLING OVER ROAD C WAR EMBLEM PLACE WAR A N Future P H City A R O Park A H D R I V E 14DUST COMMANDER COURT CIRCLE PASS FORWARD DETERMINE DRIVE SPECTACULAR BID STREET REAL QUIET RD. TIM TAM CIRCLE EASY GOER AVENUE LEGEND PILLORY DRIVE PILLORY BY PHASES HALMA HALMA TRAIL 11 PHASE 1 A PROUD CLAIRON STREET M E MIDDLEGROUND PLACE -

BAY FILLY Barn 20 Hip No. 3495
Consigned by VanMeter-Gentry Sales, Agent XVIII Barn BAY FILLY Hip No. 20 Foaled February 8, 2018 3495 A.P. Indy Malibu Moon ........................ Macoumba Orb ........................................ Unbridled Lady Liberty .......................... Mesabi Maiden BAY FILLY Storm Cat Bernstein .............................. La Affirmed Soft Whisper ........................ (2009) Unbridled's Song Unbridled Mistress .............. Special Mistress By ORB (2010). Classic winner of $2,612,516, Kentucky Derby [G1] (CD, $1,- 414,800), etc. Sire of 3 crops of racing age, 273 foals, 148 starters, 78 winners of 127 races and earning $4,911,964, including Sippican Harbor ($262,650, Spinaway S. [G1] (SAR, $192,500)), Orbolution ($164,150, P. G. Johnson S. [L] (SAR, $60,000), etc.), Autumn Warrior ($94,020, Super Derby Prelude S. (LAD, $36,000), etc.), black-type-placed Zero Gravity [G3] ($132,317), Inspeightof [L] ($114,290), Orra Moor [L] ($112,900), etc. 1st dam Soft Whisper , by Bernstein. 6 wins, 2 to 5, $317,778, 2nd West Virginia Senate President's Cup S. [L] (MNR, $20,000), Dream Supreme S. (CD, $11,- 921), 3rd Kentucky Downs Ladies Sprint S. (KD, $15,996), Indian Maid H (HAW, $7,500), Ellis Park Turf S. (ELP, $5,500), Holiday Inaugural S. (TP, $4,700). Dam of 2 other registered foals, 1 of racing age, a 2-year- old of 2019, which has not started. 2nd dam UNBRIDLED MISTRESS, by Unbridled's Song. Placed at 3 and 4, $8,200. Sis - ter to UNINHIBITED SONG . Dam of 4 winners, including-- Soft Whisper (f. by Bernstein). Black-type-placed winner, above. 3rd dam SPECIAL MISTRESS, by Deputy Minister. Unraced. -
Lex Mastermap Handout
ELDORADO PARKWAY M A MM *ZONED FUTURE O TH LIGHT RETAIL C A VE LANE MASTER PLANNED GATED COMMUNITY *ZONED FUTURE RETAIL/MULTI-FAMILY M A J E MAMMOTH CAVE LANE S T T IN I C O P P L I R A I N R E C N E O C D I R C L ORB DRIVE E A R I S T MACBETH AVENUE I D E S D R I V E M SPOKANE WAY D ANUEL STRE ARK S G I A C T O AR LANE CARRY BACK LANE 7 M O E L T A N E 8 NORTHERN DANCER WAY GALLAHADION WAY GRINDS FUN N T Y CIDE ONE THUNDER GULCH WAY M C ANOR OU BROKERS TIP LANE R T M ANUEL STRE E PLAC RAL DMI WAR A E T DAY STAR WAY *ZONED FUTURE 3 LIGHT COMMERCIAL BOLD FORBES STREET FERDINAND VIEW LEON PONDER LANE A TUS LANE SEATTLE SLEW STREET GRAHAM AVENUE WINTE R GREEN DRIVE C OIT SECRETARIAT BOULEVARD C OUNT R O TURF DRIVE AD S AMENITY M A CENTER R T Y JONES STRE STRIKE GOLD BOULEVARD E T L 5 2 UC K Y DEBONAIR LANE C 1 A Yucca Ridge *ZONED FUTURE V FLYING EBONY STREET A LIGHT RETAIL L C Park ADE DRIVE AFFIRMED AVENUE Independence High School SUTHERLAND LANE AZRA TRAIL OMAHA DRIVE BOLD VENTURE AVENUE C L ONQUIS UC O XBOW K Y DEBONAIR LANE C 4 T A ADOR V A A VENUE L C ADE DRIVE WHIRLAWAY DRIVE C OU R 9T IRON LIEGE DRIVE *ZONED FUTURE IRON LIEGE DRIVE LIGHT COMMERCIAL 6 A M EMPIRE MAKER ROAD E RISEN STAR ROAD R I BUBBLING OVER C W A AR EMBLEM PL N Future P H City A R O Park A H D R A O R CE I AD V E DUST COMMANDER COURT FO DETERMINE DRIVE R W ARD P 14 ASS CI SPECTACULAR BID STREET REAL QUI R CLE E T R TIM TAM CIRCLE D . -
Wagering Guide
TRAVERS STAKES WAGERING GUIDE 866.88XPRESS (866.889.7737) National gambling support line 800.522.4700 Fellow Race Fans! Welcome to the first edition of Xpressbet’s Travers Stakes Wagering Guide! Affectionately dubbed the ‘Midsummer Derby,’ the Travers Stakes is the keystone race of Saratoga’s seven- week meet. Now in its 144th running, the Travers annually attracts the nation’s premier three-year-olds and is an important step on the trail to the Breeders’ Cup Classic. To help you separate the contenders from the pretenders in this year’s Travers, we’ve produced this handy Wagering Guide so that you can bet the race with confidence. Our Travers Stakes Wagering Guide was written with you, the Bettor, in mind. Our contributors have decades of industry experience, and each approaches handicapping the races from a different, unique perspective. Inside this Guide, you’ll find Race Analysis, Main Contender Profiles and potential Value Plays from each of our contributors, along with $100 Wagering Strategies to help you play the race intelligently. At Xpressbet, we do more than simply process your wagers. To us, it’s important that we arm our customers with the best information available. Take a look at our free Daily Picks, access the products in our Pro Shop and read our free Wagering Guides. Hopefully they’ll help you cash a few wagers. Bet the Travers Stakes with Xpressbet on your computer or mobile device on Saturday, August 24, and we hope our Wagering Guide will help you pick the winner. We hope you enjoyed our Saratoga Wagering Guides this year, and we hope they helped you cash some tickets. -

CHESTNUT FILLY Barn 1 Hip No. 62
Property of Blake-Albina Thoroughbred Services LLC Hip No. CHESTNUT FILLY Barn 62 Foaled February 19, 2018 1 Seattle Slew A.P. Indy ................................ Weekend Surprise Malibu Moon ........................ Mr. Prospector Macoumba ............................ Maximova (FR) CHESTNUT FILLY Unbridled Unbridled's Song .................. Trolley Song Samsational .......................... (2012) Roy Meguial (ARG) ...................... Starry Night By MALIBU MOON (1997). Winner of $33,840. Among the leading sires, sire of 17 crops of racing age, 1818 foals, 1414 starters, 116 black-type win - ners, 1038 winners of 3338 races and earning $117,811,623, 2 champi - ons, including Declan's Moon ($705,647, Hollywood Futurity [G1] (HOL, $267,900), etc.), and of Devil May Care ($724,000, BetFair TVG Coaching Club American Oaks [G1] (SAR, $150,000), etc.), Orb ($2,612,516, Ken - tucky Derby [G1] (CD, $1,414,800), etc.), Life At Ten [G1] ($1,277,515). 1st dam SAMSATIONAL, by Unbridled's Song. Unraced. Dam of 2 other registered foals, 2 of racing age, including a 2-year-old of 2019, 1 to race, 1 winner-- Sam’n Cat (f. by Tale of the Cat). Winner at 3, 2019, $6,204, in N.A./U.S. (Total: $6,813). 2nd dam MEGUIAL (ARG) , by Roy. Winner at 2 in Argentina, Juan Salvador Boucau [L], 2nd Polla de Potrancas-Argentine One Thousand Guineas [G1] , Seleccion- Argentine Oaks [G1] , 3rd Mil Guineas [G1] ; winner at 4, $61,980, in N.A./ U.S., 3rd Golden Poppy H. (BM, $9,000), etc. (Total: $69,793). Dam of-- I WANT REVENGE (c. by Stephen Got Even). 3 wins at 2 and 3, $928,000, Wood Memorial S. -

Bay Horse; Foaled 2010 by MALIBU MOON (1997). Winner of $33,840. Among the Leading Sires, Sire of 90 Black-Type Winners, Includi
ORB Bay Horse; foaled 2010 Seattle Slew A.P. Indy ............................ Weekend Surprise Malibu Moon .................... Mr. Prospector Macoumba ........................ Maximova (FR) ORB Fappiano Unbridled .......................... Gana Facil Lady Liberty ...................... (1999) Cox's Ridge Mesabi Maiden ................ Steel Maiden By MALIBU MOON (1997). Winner of $33,840. Among the leading sires, sire of 90 black-type winners, including champion Declan's Moon ($705,647, Hollywood Futurity [G1] (HOL, $267,900), etc.), and of Orb ($2,612,516, Kentucky Derby [G1] (CD, $1,414,800), Life At Ten [G1] ($1,277,515), Devil May Care [G1] ($724,000), Ask the Moon [G1] (10 wins, $713,640). 1st dam LADY LIBERTY, by Unbridled. 4 wins, 3 to 5, $202,045. Dam of 6 foals, 3 to race, 2 winners, including-- ORB (c. by Malibu Moon). Subject stallion. 2nd dam MESABI MAIDEN , by Cox's Ridge. 3 wins at 2 and 3, $240,314, Black-Eyed Susan S. [G2] , 3rd Monmouth Breeders' Cup Oaks [G2] , New York City Astarita S. [G2] , Anne Arundel S. [G3] . Dam of-- Steely Dame. 4 wins, 2 to 4, $45,006. 3rd dam STEEL MAIDEN , by Damascus. 4 wins to 3, $119,030, Dancealot S. [L] (LRL, $36,660), Resolution S. (LRL, $28,210), etc. Dam of 4 winners, incl.-- MESABI MAIDEN . Black-type winner, above. Pro Prospect . 8 wins, 3 to 6, $136,328, 2nd Sportsman's Park Budweiser Breeders' Cup H. [L] (SPT, $21,020), 3rd Better Bee S. (AP, $3,481). Sire. Women's Rights. Unraced. Producer. Granddam of SUGGESTIVE BOY (ARG) (Total: $730,654, champion twice in Argentina, Jockey Club [G1] , etc.), SUBTLETY (to 5, 2015, Total: $103,091, Republica Oriental Del Uruguay [G3] , etc.), Suffisant (Total: $32,467, 2nd Gran Premio Cri - adores Salvador Hess Riveros [G2] , Jose Saavedra Baeza [G3] , etc.). -

Coralina Bay Colt; Feb 11, 2016 A.P
equineline.com Product 40P 11/29/17 13:48:42 EST 16--Coralina Bay Colt; Feb 11, 2016 A.P. Indy, 89 dk b/ Malibu Moon, 97 b Macoumba, 92 b Orb, 10 b Unbridled, 87 b Unnamed Lady Liberty, 99 b Mesabi Maiden, 93 b Foaled in Kentucky Cee's Tizzy, 87 gr/ro Tiznow, 97 b Coralina, 10 b Cee's Song, 86 dk b/ Forestry, 96 b Forestier, 01 b D'Youville Nurse, 84 b By ORB (2010). Classic winner of 5 races of $2,612,516, Kentucky Derby [G1] (CD, $1,414,800), Besilu Stables Florida Derby [G1] (GP, $600,000), etc. His first foals are 2-year-olds of 2017. Sire of 99 foals, 36 starters, 1 stakes winner, 7 winners of 8 races and earning $490,298 USA, including Orbolution (at 2, 2017, $145,800, P. G. Johnson S. [L] (SAR, $60,000), etc.), Earth (at 2, 2017, $34,500, 3rd Tyro S. (MTH, $6,000)), Radiant Beauty (at 2, 2017, $61,688), Golden Orb (at 2, 2017, $56,850 USA), Belles Orb (at 2, 2017, $25,860), Poco Suenos (at 2, 2017, $21,254), Lunaris (at 2, 2017, $12,570), On the Hassle (placed, at 2, 2017, $21,800), Orbatron (placed, at 2, 2017, $21,336), Orbortunistic (placed, at 2, 2017, $12,966 USA). 1st dam CORALINA, by Tiznow. Unplaced. Dam of 2 foals-- Unnamed (c. by Orb). 2nd dam FORESTIER, by Forestry. 5 wins, 2 to 4, $195,710, Classy Mirage S. -R (AQU, $36,360), 2nd Jameela S. -R (LRL, $15,000), Marshua S. -

NO LAUGHING MATTER Digestive Health Progeny of Practical Joke Coveted Rethink at Juvenile Sales See Page 4
MONDAY, APRIL 19, 2021 BLOODHORSE.COM/DAILY COURTESY ASHFORD STUD COURTESY your horse’s NO LAUGHING MATTER digestive health Progeny of Practical Joke Coveted rethink at Juvenile Sales See page 4 relyneGI gives horse owners like you just what they want for their horses. IN THIS ISSUE A PATENTED STOMACH-BUFFERING HA AN IMMUNE-BOOSTING BETA-GLUCAN 9 On Racing: Another Jockey Heartbreak A NATURAL ALTERNATIVE FOR DAILY, on Derby-Go-Round LONG-TERM USE 12 Prat Guides Cezanne, Tizamagician to Stakes Victories Buy now at Resolvet.com by 14 Bubbles On Ice Breaks Through RESOLVET.COM • 859.281.9511 in Memories of Silver BLOODHORSE DAILY Download the FREE smartphone app PAGE 1 OF 34 CONTENTS 4 Progeny of Practical Joke Coveted at Juvenile Sales 7 Leading Sires 9 On Racing: Another Jockey Heartbreak on Derby-Go-Round 12 Prat Guides Cezanne, Tizamagician to Stakes Victories 14 Bubbles On Ice Breaks Through in Memories of Silver 16 Undefeated Efforia Lands Japan’s Two Thousand Guineas 18 Highly Motivated Works Ahead of Kentucky Derby 19 Rosario to Ride Rock Your World in Kentucky Derby 21 Letruska Exits Apple Blossom Victory in Good Order 23 Eclipse Thoroughbred Partners’ Turf Runners Gear Up 26 Mean Mary Eyes Return in New York Stakes 27 Former Manager of Royal Studs Sir Michael Oswald Dies 28 Snow Lantern Showcases Classic Credentials at Newbury 30 Results & Entries ANNE M. EBERHARDT ANNE M. TAA a ccreditation: The G o l d S t a n d a r d in aftercare. A publication of The Jockey Club Information Systems, Inc. -

It Was American Pharoah
WEDNESDAY, JANUARY 1, 2020 HORSE OF THE DECADE? IT INDEPENDENCE HALL LOOMS LARGE IN JEROME WAS AMERICAN PHAROAH Leading newly turned sophomore Independence Hall (Constitution) is an overwhelming 1-5 morning line favorite in Wednesday=s Jerome S. at Aqueduct, which carries with it 10 qualifying points for the 2020 GI Kentucky Derby. A 4 3/4-length debut winner at Parx Sept. 21, the Mike Trombetta trainee annexed the track-and-trip GIII Nashua S. Nov. 3 by 12 1/4 lengths, good for a 101 Beyer Speed Figure, the fastest run by a 2-year-old last term. Second choice on the morning line is New York-bred Bourbon Bay (Bayern). A narrow runner-up in his sprint unveiling Nov. 11, he broke through emphatically in another restricted and abbreviated affair here Dec. 5. Prince of Pharoahs (American Pharoah), also bred in the Empire State, was last seen airing by five lengths going a mile at Belmont Oct. 13 in his second attempt. See field p7 American Pharoah | Sarah Andrew by Bill Finley More than just a year ended Tuesday. The sport says goodbye not just to 2019, but to an entire decade, one filled with IN TDN EUROPE TODAY tremendous highs (two Triple Crown winners) and tremendous GALILEO SCALING THE HEIGHTS lows (2019's fatalities at Santa Anita). To mark the occasion, we Galileo continues his meteoric ascent by adding his eleventh submit our winners in random group of categories, celebrating champion sire title in England and Ireland. Click or tap here to the very best of the 2010's. -

Early Derby Favorite Bill Seeks Usada Drug Regulation
THURSDAY, MAY 2, 2013 732-747-8060 $ TDN Home Page Click Here ORB DRAWS 16; EARLY DERBY FAVORITE BILL SEEKS USADA DRUG REGULATION An oversubscribed field of 21 was yesterday drawn Senator Tom Udall and Representative Joe Pitts are for Saturday=s 139th running of the GI Kentucky Derby, expected to introduce legislation in Congress next week with 7-2 morning-line choice Orb (Malibu Moon) which would give power to regulate the horse racing drawing post 16 and 50-1 longshot Fear the Kitten industry to the United States Anti-Doping Agency. An (Kitten=s Joy) the lone entrant on the also-eligible list. independent organization, USADA is in charge of drug Unbeaten Verrazano (More Than Ready) is the 4-1 testing for the United States Olympic Team. According second choice on the morning line and drew post 14. to the New York Times, the Horseracing Integrity and Connections of Safety Act would empower the USADA to develop the two favorites national rules for approved and prohibited substances had to sweat out and would create testing and penalty programs. the pill draw as AThe chronic abuse of racehorses with painkillers and both were left other drugs is dangerous and just plain wrong,@ Udall late in the told the Times. ARacing groups have promised drug process and with reform for decades, but this bill would bring in real the unpopular standards and enforcement from an organization with a inside posts proven record for cleaning up sports.@ remaining. Orb=s News of the proposed legislation brought a measured number was the response from industry organizations. -

750 Orb 2010 Page 1
#750 Orb 2010 Page 1 Seattle Slew A.P. Indy Weekend Surprise Malibu Moon Mr. Prospector Orb Macoumba Maximova (FR) Bay Colt Fappiano Foaled February 24, 2010 Unbridled Lady Liberty Gana Facil (1999) Cox's Ridge Mesabi Maiden Steel Maiden By MALIBU MOON (1997), Winner, $33,840. Sire of 11 crops. 922 foals, 701 starters, 63 black type winners, 516 winners, $55,998,919, including Declan's Moon (Champion, $705,647), Life at Ten ($1,277,515, Beldame S. [G1], etc.), Orb ($921,050, Besilu Stables Florida Derby [G1], etc.), Devil May Care ($724,000, Frizette S. [G1], etc.), Malibu Mint ($723,829, Princess Rooney Handicap [G1], etc.), Ask the Moon ($713,640, Personal Ensign Invitational S. [G1], etc.), Malibu Prayer ($618,026, Ruffian Invitational H. [G1], etc.). 1ST DAM LADY LIBERTY, by Unbridled. 4 wins, 3 to 5, $202,045 in NA. Dam of 3 foals to race, 2 winners-- ORB (c, by Malibu Moon). Black type winner, see records. Cause of Freedom (g, by Alphabet Soup). 3 wins at 4 and 5, $105,834 in US. 2ND DAM MESABI MAIDEN, by Cox's Ridge. 3 wins at 2 and 3, $240,314 in NA. Won Black-Eyed Susan S. [G2]. 3rd Monmouth Breeders' Cup Oaks [G2], Astarita S. [G2], Anne Arundel S. [G3]. Dam of 6 foals to race, 2 winners, including-- Steely Dame (f, by Purge). 4 wins, 2 to 4, $45,006 in US. Altar Girl (f, by Pulpit). Placed at 2, $1,350 in NA. Placed at 3, $2,305 in US. (Total: $3,655) Dam of 2 winners, including-- Narita. -

RUNNING STYLE at Quarter Mile Decidedly 1962 9 9 ¼ Carry Back 1961 11 18
RUNNING STYLE At Quarter Mile Decidedly 1962 9 9 ¼ Carry Back 1961 11 18 Venetian Way 1960 4 3 ½ Wire-To-Wire Kentucky Derby Winners : Horse Year Call Lengths Tomy Lee 1959 2 1 ½ American Pharoah 2015 3 1 Tim Tam 1958 8 11 This listing represents 22 Kentucky Derby California Chrome 2014 3 2 Iron Liege 1957 3 1 ½ winners that have led at each point of call during the Orb 2013 16 10 Needles 1956 16 15 race. Points of call for the Kentucky Derby are a I’ll Have Another 2012 6 4 ¼ quarter-mile, half-mile, three-quarter-mile, mile, Swaps 1955 1 1 Animal Kingdom 2011 12 6 Determine 1954 3 4 ½ stretch and finish. Super Saver 2010 6 5 ½ From 1875 to 1959 a start call was given for Dark Star 1953 1 1 ½ Mine That Bird 2009 19 21 Hill Gail 1952 2 2 the race, but was discontinued in 1960. The quarter- Big Brown 2008 4 1 ½ Count Turf 1951 11 7 ¼ mile then replaced the start as the first point of call. Street Sense 2007 18 15 Middleground 1950 5 6 Barbaro 2006 5 3 ¼ Ponder 1949 14 16 Wire-to-Wire Winner Year Giacomo 2005 18 11 Citation 1948 2 6 Smarty Jones 2004 4 1 ¾ War Emblem 2002 Jet Pilot 1947 1 1 ½ Funny Cide 2003 4 2 Winning Colors-f 1988 Assault 1946 5 3 ½ War Emblem 2002 1 ½ Spend a Buck 1985 Hoop Jr. 1945 1 1 Monarchos 2001 13 13 ½ Bold Forbes 1976 Pensive 1944 13 11 Riva Ridge 1972 Fusaichi Pegasus 2000 15 12 ½ Count Fleet 1943 1 head Kauai King 1966 Charismatic 1999 7 3 ¾ Shut Out 1942 4 2 ¼ Jet Pilot 1947 Real Quiet 1998 8 6 ¾ Whirlaway 1941 8 15 ½ Silver Charm 1997 6 4 ¼ Count Fleet 1943 Gallahadion 1940 3 2 Grindstone 1996 15 16 ¾ Bubbling Over 1926 Johnstown 1939 1 2 Thunder Gulch 1995 6 3 Paul Jones 1920 Lawrin 1938 5 7 ½ Go for Gin 1994 2 head Sir Barton 1919 War Admiral 1937 1 1 ½ Sea Hero 1993 13 10 ¾ Regret-f 1915 Bold Venture 1936 8 5 ¾ Lil E.