Beyond the Streetlight in Hearing Aid Research
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Learning About Hearing Aids
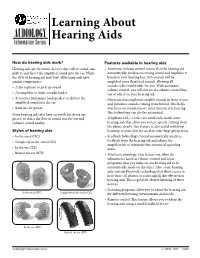
Learning About AUDIOLOGY Information Series Hearing Aids How do hearing aids work? Features available in hearing aids Hearing aids are electronic devices that collect sound, am- • Automatic volume control means that the hearing aid plify it, and direct the amplified sound into the ear. While automatically analyzes incoming sound and amplifies it the style of hearing aid may vary, all hearing aids have based on your hearing loss. Soft sounds will be similar components: amplified more than loud sounds, allowing all • A microphone to pick up sound sounds to be comfortable for you. With automatic volume control, you will not need a volume control but- • An amplifier to make sounds louder ton or wheel on your hearing aid. • A receiver (miniature loudspeaker) to deliver the • Directional microphones amplify sounds in front of you amplified sound into the ear and minimize sounds coming from behind. This helps • Batteries for power you focus on sound you are most interested in hearing. This technology can also be automated. Some hearing aids also have earmolds (or dome ear pieces) to direct the flow of sound into the ear and • Telephone coils (t-coils) are small coils inside some enhance sound quality. hearing aids that allow you to hear speech coming from the phone clearly. This feature is also useful with loop Styles of hearing aids listening systems that are used in some large group areas. • In-the-canal (ITC) • Feedback (whistling) control automatically analyzes • Completely-in-the-canal (CIC) feedback from the hearing aid and adjusts the amplification to minimize this unwanted squealing • In-the-ear (ITE) noise. -

A Study on Wireless Hearing Aids System Configuration and Simulation
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by ScholarBank@NUS A STUDY ON WIRELESS HEARING AIDS SYSTEM CONFIGURATION AND SIMULATION TANG BIN NATIONAL UNIVERSITY OF SINGAPORE 2005 A STUDY ON WIRELESS HEARING AIDS SYSTEM CONFIGURATION AND SIMULATION TANG BIN (B. ENG) A THESIS SUBMITTED FOR THE DEGREE OF MASTER OF SCIENCE GRADUATE PROGRAM IN BIOENGINEERING NATIONAL UNIVERSITY OF SINGAPORE 2005 ACKNOWLEDGEMENT I would like to thank my supervisors, Dr. Ram Singh Rana, A/Prof. Hari Krishna Garg, and Dr. Wang De Yun for their invaluable guidance, advice and motivation. Without their generous guidance and patience, it would have been an insurmountable task in completing this work. Their research attitudes and inspirations have impressed me deeply. I have learned from them not only how to do the research work, but also the way to difficulties and life. I would also like to extend my appreciation to A/Prof. Hanry Yu and Prof. Teoh Swee Hin, for the founding and growing of the Graduate Program in bioengineering, and also the perfect research environment they have created for the students. Special thanks to Dr. Hsueh Yee Lim from National University Hospital for her precious suggestions and encouragement as a hearing clinician to my research work. Thanks my colleague Zhang Liang, who is pursuing his master degree in department of Electrical and Computer Engineering. The valuable suggestions and discussions with him have contributed a lot to this work. This work would have been impossible without the consent for Dr. Wang De Yun to support my scholarship. -
Remote Microphone + Operations Manual
Remote Microphone + OPERATIONS MANUAL Table of Contents Overview � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 2 Basic Use � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 6 Daily Use � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 8 Wearing the Remote Mic + � � � � � � � � � � � � � � � � � � � � � � 10 Pairing with Hearing Aids � � � � � � � � � � � � � � � � � � � � � � � 11 Pairing with Bluetooth Devices � � � � � � � � � � � � � � � � � � � 13 Using the Input Mode Button � � � � � � � � � � � � � � � � � � � � 14 Remote Microphone � � � � � � � � � � � � � � � � � � � � � � � � � � � 14 Bluetooth Phone and Audio � � � � � � � � � � � � � � � � � � � � � 15 Loop System � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 17 FM System � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 17 Line-In � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 17 Start/Stop Audio Streaming � � � � � � � � � � � � � � � � � � � � � 18 Assembling the Power Adapter � � � � � � � � � � � � � � � � � � � 19 Troubleshooting � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 20 Safety Information � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 23 Regulatory Notices � � � � � � � � � � � � � � � � � � � � � � � � � � � � 26 2 | Overview Overview | 3 The Remote Microphone + is designed to stream 2 audio from different audio sources directly to your 2.4 3 GHz wireless hearing aids. 1 When worn by a distant -

Signal Processing in High-End Hearing Aids: State of the Art, Challenges, and Future Trends
EURASIP Journal on Applied Signal Processing 2005:18, 2915–2929 c 2005 V. Hamacher et al. Signal Processing in High-End Hearing Aids: State of the Art, Challenges, and Future Trends V. Hamacher, J. Chalupper, J. Eggers, E. Fischer, U. Kornagel, H. Puder, and U. Rass Siemens Audiological Engineering Group, Gebbertstrasse 125, 91058 Erlangen, Germany Emails: [email protected], [email protected], [email protected], eghart.fi[email protected], [email protected], [email protected], [email protected] Received 30 April 2004; Revised 18 September 2004 The development of hearing aids incorporates two aspects, namely, the audiological and the technical point of view. The former focuses on items like the recruitment phenomenon, the speech intelligibility of hearing-impaired persons, or just on the question of hearing comfort. Concerning these subjects, different algorithms intending to improve the hearing ability are presented in this paper. These are automatic gain controls, directional microphones, and noise reduction algorithms. Besides the audiological point of view, there are several purely technical problems which have to be solved. An important one is the acoustic feedback. Another instance is the proper automatic control of all hearing aid components by means of a classification unit. In addition to an overview of state-of-the-art algorithms, this paper focuses on future trends. Keywords and phrases: digital hearing aid, directional microphone, noise reduction, acoustic feedback, classification, compres- sion. 1. INTRODUCTION being close to each other. Details regarding this problem and possible solutions are discussed in Section 5. Note that Driven by the continuous progress in the semiconductor feedback suppression can be applied at different stages of technology, today’s high-end digital hearing aids offer pow- the signal flow dependent on the chosen strategy. -

Hearing Loss and Hearing Aid Options Options for Style and Technology Understanding Hearing Loss
YOUR VALUES YOUR PREFERENCES YOUR CHOICE Hearing Loss and Hearing Aid Options Options for Style and Technology Understanding Hearing Loss Hearing Loss These problems can get worse with age. Hearing loss caused by aging usually affects high pitch sounds more than low pitch If you have hearing loss, part of your ear has been damaged. sounds. A hearing aid cannot bring back normal hearing but it can help you hear better. Hearing aids can help you hear certain pitches you are missing. However, hearing aids cannot give you back normal hearing. Hearing loss affects each person differently. For example, one person with mild hearing loss will have no problems Hearing Aids with his or her day-to-day activities. Another person may Hearing aids are devices that make sounds louder at many have a lot of problems hearing and understanding others. different pitches. Most people lose their hearing over time. It will take time for There are many different types and styles of hearing aids. you to get used to hearing the sounds you have been missing. Hearing aids can: Call your primary care provider if you are having trouble make the sound louder so it can reach the parts of the ear hearing and understanding others. He or she may want you that are still working to see an audiologist (hearing specialist) to have a hearing test. help you better understand people talking to you in a What are the effects of hearing loss? different listening situations Hearing loss that is not treated can affect communication help you keep the volume on the television lower. -

Low-Voltage CMOS Log-Companding Techniques for Audio Applications
(c) 2004 Kluwer Academic Publishers http://dx.doi.org/10.1023/B:ALOG.0000011163.29809.57 Low-Voltage CMOS Log-Companding Techniques for Audio Applications Francisco Serra-Graells ([email protected]) Centro Nacional de Microelectr´onica, Institut de Microelect`onica de Barcelona Adoraci´onRueda ([email protected]) Centro Nacional de Microelectr´onica, Instituto de Microelectr´onica de Sevilla Jos´eLuis Huertas ([email protected]) Centro Nacional de Microelectr´onica, Instituto de Microelectr´onica de Sevilla Abstract. This paper presents a collection of novel current-mode circuit techniques for the integration of very low-voltage (down to 1V) low-power (few hundreds of ¹A) complete SoCs in CMOS technologies. The new design proposal is based on both, the Log Companding theory and the MOSFET operating in subthreshold. Several basic building blocks for audio amplification, AGC and arbitrary filtering are given. The feasibility of the proposed CMOS circuits is illustrated through experimental data for different design case studies in 1.2¹m and 0.35¹m VLSI technologies. Keywords: Low-Voltage, CMOS, Subthreshold, Log, Companding, Audio, Design, Hearing-Aids 1. Introduction The increasing market demand on portable System-on-Chip (SoC) ap- plications has stimulated the search for new low-voltage and low-power analog techniques for mixed VLSI circuits. The critical design con- strains in such products come from the battery technology itself, which imposes very low-voltage supply operation (down to 1.1V) combined with low-power figures (below 1mA) in order to extend battery life as long as possible. In order to overcome the very low-voltage restriction in CMOS tech- nologies, supply multipliers based on charge pumps [1] are commonly used, although some effort are being done in switched-capacitors filters for very low-voltage compatibility [2]. -

Shopping Wisely for Hearing Aids
Consumer’s Edge Consumer Protection Division, Maryland Office of the Attorney General Brian E. Frosh, Maryland Attorney General Listen Up! Shopping Wisely for Hearing Aids Evelyn spent $2,300 for hearing aids but they did not your problem is diagnosed properly, since a hearing loss improve her ability to hear. Although she informed the may be a symptom of a more serious medical condition. seller, he repeatedly insisted she simply needed more time to get used to them. The sales contract didn’t in- A hearing aid seller is required by federal law to inform clude the 30-day notice of cancellation as required by you that it is in your best interest to have a medical exam law. After contacting the Attorney General’s Consumer by a licensed physician. In fact, your hearing must be Protection Division, she was able to get a refund. evaluated by a doctor before you buy a hearing aid, unless you sign a statement saying you’ve waived that protection. Don’t sign it. It’s always wise to have a medical evaluation to make sure all medically treatable conditions that may affect your hearing are identified and treated before you purchase a hearing aid. What kind of doctor should you see to have your hearing evaluated? The U.S. Food and Drug Administration recom- mends an ear, nose and throat specialist (otolaryngologist), an ear specialist (otologist) or any licensed physician. Look for the right seller. Once your doctor confirms you need a hearing aid, you’ll need a hearing aid evaluation. Hearing aids can be difficult to fit, often requiring several adjustments. -
Hearing Aids: the Basic Information You Need to Know
Hearing Aids: The Basic Information You Need to Know FDA BASICS WEBINAR May 23, 2012 Presented by Shu‐Chen Peng, Ph.D. CCC‐A Scientific Reviewer in Audiology Center for Devices and Radiological Health Outline Hearing loss Basics about hearing aids . What are hearing aids and who are they for? . How does a hearing aid work? . Styles and common features Getting the most out of your hearing aids . Hearing aid fitting & care . Hearing aid benefits & limitations . Learning to listen with hearing aids Hearing Aids vs. Personal Sound Amplifying Products Questions & Answers 2 Facts about Hearing Loss Individuals with hearing loss may be limited in daily oral communication. Some facts about hearing loss & hearing aids (NIDCD/NIH) . 36 million (or 17%) adult population in the US report some degree of hearing loss. Less than 20% of those with hearing loss who might benefit from treatment actually seek help. Most hearing aid users had lived with hearing loss for 10+ years, and waited until it progressed to moderate‐to‐severe levels before seeking professional help for hearing aid fitting. 3 Types of Hearing Loss Conductive: Middle ear pathology Sensorineural: Damage at the inner ear (cochlea) Mixed: Both cochlear damage & outer/middle ear pathology 4 Degrees of Hearing Loss 0 ‐ 20 dB HL: Within normal limits (WNL) 20 ‐40 dB HL: Mild 40 ‐70 dB HL: Moderate WNL 70 ‐90 dB HL: Severe > 90 dB HL: Profound mild moderate severe profound 5 Who are Hearing Aids for? Sound‐amplifying medical devices to aid individuals with hearing loss. Hearing aids may be useful for: . -

Low Noise Amplifier Design and Noise Cancellation for Wireless Hearing Aids
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by ScholarBank@NUS LOW NOISE AMPLIFIER DESIGN AND NOISE CANCELLATION FOR WIRELESS HEARING AIDS ZHANG LIANG NATIONAL UNIVERSITY OF SINGAPORE 2005 LOW NOISE AMPLIFIER DESIGN AND NOISE CANCELLATION FOR WIRELESS HEARING AIDS ZHANG LIANG A THESIS SUBMITTED FOR THE DEGREE OF MASTER OF ENGINEERING DEPARTMENT OF ELECTRICAL AND COMPUTER ENGINEERING NATIONAL UNIVERSITY OF SINGAPORE 2005 Acknowledgements I would like to thank my supervisors, Dr. Ram Singh Rana and A/Prof. Hari Krishna Garg. They gave me opportunities to blossom my research ideas. Their research attitudes and inspirations are impressed deeply on me. During the two years study, they helped me open my mind and be an independent researcher. I learnt a lot from them not only how to think about problems but also how to do the research work. I hope they are proud of having me as research scholar as I am proud to have them as my supervisors. Specifically thank to my colleague, TangBin who is pursuing his Graduate Program in Bioengineering. I really appreciate many valuable discussions held with him. Furthermore, I would like to thank the Institute of Microelectronics (IME) for providing the scholarship in the past two years. This work has been supported by IME and NUS (National University of Singapore). The infrastructure and the fabrication support provided by IME are greatly acknowledged. Finally, I thank my families for their never-ending support who had patience while I was away from them during -
User Guide Lyric(Pdf)
User Guide The contact lens for your ear™ This user guide is valid for the following hearing aid model: Non wireless model CE mark applied Lyric3 2014 Contents 1. Introduction to Lyric 6 1.1 What makes Lyric different 7 1.2 What you can expect with your new Lyric 7 2. Adjusting and removing Lyric 10 2.1 Using the SoundLync™ 10 2.2 Putting Lyric in SLEEP mode 12 2.3 Turning Lyric OFF 12 2.4 Turning Lyric ON 13 2.5 Adjusting the volume 13 2.6 SoundLync quick reference 14 2.7 Self-removal instructions 15 3. Follow-up care and replacement 19 4. Frequently asked questions 21 5. Service and warranty 27 6. Compliance information 28 7. Information and explanation of symbols 29 8. Important information: Cell phones 34 9. For the US market only, complies with 36 the FDA regulations 10. Privacy Notice 40 11. Important safety information 42 11.1 Hazard warnings 42 11.2 Information on product safety 45 Lyric. The contact lens for your ear. Thank you for choosing Lyric, the first extended wear hearing aid that is 100% invisible. Your Lyric hearing aid requires a lot less interaction and handling compared to conventional hearing aids. We are convinced that your hearing aid will provide valuable benefits to your daily life. Please read this user guide carefully in order to safely operate your Lyric hearing aid and to benefit from all the possibilities it has to offer. If you have any questions, please consult your hearing care professional. Phonak – life is on www.phonak.com 5 1. -

Digital Hearing Aids: a Tutorial Review*
Veterans Administration Journal of Rehabilitation Research and Development Vol. 24 No. 4 Pages 7-20 Digital hearing aids: A tutorial review* HARRY LEVYITT, PIh,D. GenterJi)r Research in Speech nnd Nearing Sciences, Crud~ruieSchool and Uni~~ersityCenter of tlze Cily Univec~ityof Mew Yo&, New YorA, NY 10036 Abstract-The basic concepts underlying digital signal hearing aids because of the constraints on chip size processing are reviewed briefly, followed by a short and power consumption. But all of the above- historical account of the development of digital hearing mentioned features have already been demonstrated aids. Key problem areas and opportunities are identified, in a master digital hearing aid (12,14) and it is likely and the various approaches used in attempting to develop that (with the development of more advanced signal- a practical digital hearing aid are discussed. processing chips) an increasing number of these attractive features will be incorporated in the wear- able digital hearing aids of the future. ADVANTAGES OF DIGITAL HEARING AIDS The many advantages offered by digital hearing aids can be subdivided into three broad groups: Digital hearing aids promise many advantages I) Signal-processing capabilities that are analo- over conventional heartng aids. These include: gous to, but superior to, those offered by conven- Programmability; tional analog hearing aids. Much greater precision in adjusting electroacous- 2) Signal-processing capabilities that are ~~nique tic parameters; to digital systems and which cannot be implemented Self-monitoring capabilities; in conventional analog hearing aids. Logical operations for self-testing and self-cali- 3) Methods of processing and controfllng signals "oation ; that change our way of thinking about how hearing Control of acoustic feedback (a serious practical aids should be designed, prescribed, and fitted. -
Assistive Devices and Technologies for Visually and Hearing Impaired Persons
2015 Patent Landscape Report on Assistive Devices for Visually and Hearing Impaired Persons Assistive Devices and Technologies for Visually and Hearing Impaired Persons 2015 Patent Landscape Report on PATENT LANDSCAPE REPORTS PROJECT PATENT LANDSCAPE REPORT ON ASSISTIVE DEVICES AND TECHNOLOGIES FOR VISUALLY AND HEARING IMPAIRED PERSONS Prepared for: World Intellectual Property Organization By Thomson Reuters IP Analytics - Nick Solomon and Pardeep Bhandari - 2015 2 EXECUTIVE SUMMARY The present Patent Landscape Report (PLR) forms part of WIPO’s Patent Landscape Reports series 1. The PLRs started as one of the outputs of WIPO’s Development Agenda project “Developing Tools for Access to Patent Information”, (DA_19_30_31_01) described in document CDIP/4/6, adopted by the Committee on Development and IP in 2009. The project document foresaw the preparation of PLRs in the areas of food and agriculture, public health, environment and energy, and disabilities, on topics of particular interest foremost to developing and least developed countries. This report is the first one prepared in the area of disabilities. It aims to provide patent-based evidence on the available technologies, patenting and innovation trends in the area of assistive devices and technologies for visually and hearing impaired persons. The present PLR is prepared in collaboration with the World Health Organization (WHO) Medical Devices Program and the Disabilities and Rehabilitation Program 2 and is aimed , among others, at supporting the Global Cooperation on Assistive Technology (GATE)3 in its efforts to assist “ children accessing education and adults to earning a living, overcome poverty, participate in all societal activities, and live with dignity, which are some of the key objectives of the global development goals ” It will also be distributed to NGOs working to the benefit of persons with visual and/or hearing impairments.