Perjeta Full Prescribing Information
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

1: Clinical Pharmacokinetics 1
1: CLINICAL PHARMACOKINETICS 1 General overview: clinical pharmacokinetics, 2 Pharmacokinetics, 4 Drug clearance (CL), 6 Volume of distribution (Vd), 8 The half-life (t½), 10 Oral availability (F), 12 Protein binding (PB), 14 pH and pharmacokinetics, 16 1 Clinical pharmacokinetics General overview General overview: clinical pharmacokinetics 1 The ultimate aim of drug therapy is to achieve effi cacy without toxicity. This involves achieving a plasma concentration (Cp) within the ‘therapeutic window’, i.e. above the min- imal effective concentration (MEC), but below the minimal toxic concentration (MTC). Clinical pharmacokinetics is about all the factors that determine variability in the Cp and its time-course. The various factors are dealt with in subsequent chapters. Ideal therapeutics: effi cacy without toxicity Minimum Toxic Concentration (MTC) Ideal dosing Minimum Effective Concentration (MEC) Drug concentration Time The graph shows a continuous IV infusion at steady state, where the dose-rate is exactly appropriate for the patient’s clearance (CL). Inappropriate dosing Dosing too high in relation to the patient’s CL – toxicity likely Minimum Toxic Concentration (MTC) Minimum Effective Concentration (MEC) Dosing too low in relation to the Drug concentration patient’s CL – drug may be ineffective Time Some reasons for variation in CL Low CL High CL Normal variation Normal variation Renal impairment Increased renal blood fl ow Genetic poor metabolism Genetic hypermetabolism Liver impairment Enzyme induction Enzyme inhibition Old age/neonate 2 General overview Clinical Pharmacokinetics Pharmacokinetic factors determining ideal therapeutics If immediate effect is needed, a loading dose (LD) must be given to achieve a desired 1 concentration. The LD is determined by the volume of distribution (Vd). -

Pertuzumab and Trastuzumab: the Rationale Way to Synergy
Anais da Academia Brasileira de Ciências (2016) 88(1 Suppl.): 565-577 (Annals of the Brazilian Academy of Sciences) Printed version ISSN 0001-3765 / Online version ISSN 1678-2690 http://dx.doi.org/10.1590/0001-3765201620150178 www.scielo.br/aabc Pertuzumab and trastuzumab: the rationale way to synergy SANDRINE RICHARD1, FRÉDÉRIC SELLE1, JEAN-PIERRE LOTZ1,2, AHMED KHALIL1, JOSEPH GLIGOROV1,2 and DANIELE G. SOARES1 1Medical Oncology Department, APREC (Alliance Pour la Recherche En Cancérologie), Tenon Hospital (Hôpitaux Universitaires de l’Est-Parisien, AP-HP), rue de la Chine, 75020 Paris, France 2Institut Universitaire de Cancérologie Université Pierre et Marie Curie (IUC-UPMC Univ Paris 06), Sorbonne Universités, 4 place Jussieu, 75005 Paris, France Manuscript received on March 13, 2015; accepted for publication on May 5, 2015 ABSTRACT It has now been 15 years since the HER2-targeted monoclonal antibody trastuzumab was introduced in clinical and revolutionized the treatment of HER2-positive breast cancer patients. Despite this achievement, most patients with HER2-positive metastatic breast cancer still show progression of their disease, highlighting the need for new therapies. The continuous interest in novel targeted agents led to the development of pertuzumab, the first in a new class of agents, the HER dimerization inhibitors. Pertuzumab is a novel recombinant humanized antibody directed against extracellular domain II of HER2 protein that is required for the heterodimerization of HER2 with other HER receptors, leading to the activation of downstream signalling pathways. Pertuzumab combined with trastuzumab plus docetaxel was approved for the first-line treatment of patients with HER2-positive metastatic breast cancer and is currently used as a standard of care in this indication. -

Trastuzumab, Biosimilars, Trastuzumab-Hyaluronidase
Clinical Policy: Trastuzumab, Biosimilars, Trastuzumab-Hyaluronidase Reference Number: CP.PHAR.228 Effective Date: 06.01.16 Last Review Date: 05.20 Coding Implications Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description Trastuzumab (Herceptin®) is a human epidermal growth factor receptor 2 (HER2)/neu receptor antagonist. Trastuzumab-dkst (Ogivri™), trastuzumab-pkrb (Herzuma®), trastuzumab-dttb (Ontruzant®), trastuzumab-qyyp (Trazimera™), and trastuzumab-anns (Kanjinti™) are Herceptin biosimilars. Trastuzumab-hyaluronidase-oysk (Herceptin Hylecta™) is a combination of trastuzumab and hyaluronidase, an endoglycosidase. FDA Approved Indication(s) Indications* Description Herceptin, Herzuma Herceptin Ogivri, Hylecta Ontruzant, Trazimera, Kanjinti Adjuvant For adjuvant As part of a treatment X X X breast cancer treatment of regimen consisting of HER2- doxorubicin, overexpressing cyclophosphamide, node positive and either paclitaxel or node or docetaxel negative As part of a treatment X X X (ER/PR regimen with negative or docetaxel and with one high carboplatin risk feature) As a single agent X X X breast cancer: following multi- modality anthracycline based therapy Metastatic In combination with paclitaxel for first- X X X breast cancer line treatment of HER2-overexpressing metastatic breast cancer As a single agent for treatment of X X X HER2-overexpressing breast cancer in patients who have received one or more Page 1 of 13 -

Refreshing the Biologic Pipeline 2020
news feature Credit: Science Lab / Alamy Stock Photo Refreshing the biologic pipeline 2020 In the absence of face-to-face meetings, FDA and industry implemented regulatory workarounds to maintain drug and biologics approvals. These could be here to stay. John Hodgson OVID-19 might have been expected since 1996) — a small miracle in itself “COVID-19 confronted us with the need to severely impair drug approvals (Fig. 1 and Table 1). to better triage sponsors’ questions,” says Cin 2020. In the event, however, To the usual crop of rare disease and Peter Marks, the director of the Center for industry and regulators delivered a small genetic-niche cancer treatments, 2020 Biologics Evaluation and Research (CBER) miracle. They found workarounds and also added a chimeric antigen receptor at the FDA. “That was perhaps the single surrogate methods of engagement. Starting (CAR)-T cell therapy with a cleaner biggest takeaway from the pandemic related in January 2020, when the outbreak veered manufacturing process and the first to product applications.” Marks says that it westward, the number of face-to face approved blockbuster indication for a became very apparent with some COVID- meetings declined rapidly; by March, small-interfering RNA (siRNA) — the 19-related files that resolving a single they were replaced by Webex and Teams. European Medicines Agency’s (EMA) issue can help a sponsor enormously and (Secure Zoom meeting are to be added registration of the RNA interference accelerate the development cycle. Before this year.) And remarkably, by 31 December, (RNAi) therapy Leqvio (inclisiran) for COVID-19, it was conceivable that a small the US Food and Drug Administration cardiovascular disease. -

Dual Targeting of HER2-Positive Cancer with Trastuzumab Emtansine and Pertuzumab: Critical Role for Neuregulin Blockade in Antitumor Response to Combination Therapy
Published OnlineFirst October 4, 2013; DOI: 10.1158/1078-0432.CCR-13-0358 Clinical Cancer Cancer Therapy: Clinical Research See related article by Gwin and Spector, p. 278 Dual Targeting of HER2-Positive Cancer with Trastuzumab Emtansine and Pertuzumab: Critical Role for Neuregulin Blockade in Antitumor Response to Combination Therapy Gail D. Lewis Phillips1, Carter T. Fields1, Guangmin Li1, Donald Dowbenko1, Gabriele Schaefer1, Kathy Miller5, Fabrice Andre6, Howard A. Burris III8, Kathy S. Albain9, Nadia Harbeck10, Veronique Dieras7, Diana Crivellari11, Liang Fang2, Ellie Guardino3, Steven R. Olsen3, Lisa M. Crocker4, and Mark X. Sliwkowski1 Abstract Purpose: Targeting HER2 with multiple HER2-directed therapies represents a promising area of treatment for HER2-positive cancers. We investigated combining the HER2-directed antibody–drug con- jugate trastuzumab emtansine (T-DM1) with the HER2 dimerization inhibitor pertuzumab (Perjeta). Experimental Design: Drug combination studies with T-DM1 and pertuzumab were performed on cultured tumor cells and in mouse xenograft models of HER2-amplified cancer. In patients with HER2- positive locally advanced or metastatic breast cancer (mBC), T-DM1 was dose-escalated with a fixed standard pertuzumab dose in a 3þ3 phase Ib/II study design. Results: Treatment of HER2-overexpressing tumor cells in vitro with T-DM1 plus pertuzumab resulted in synergistic inhibition of cell proliferation and induction of apoptotic cell death. The presence of the HER3 ligand, heregulin (NRG-1b), reduced the cytotoxic activity of T-DM1 in a subset of breast cancer lines; this effect was reversed by the addition of pertuzumab. Results from mouse xenograft models showed enhanced antitumor efficacy with T-DM1 and pertuzumab resulting from the unique antitumor activities of each agent. -

Colony Stimulating Factors
Market Applicability Market GA KY MD NJ NY Applicable X NA X X X Colony Stimulating Factors Overrides Approval Duration Prior Authorization 1 year Quantity Limit Medications Quantity Limit Fulphila (pegfligrastim-jmdb) May be subject to quantity limit Granix (tbo-filgrastim) N/A Leukine (sargramsotim) N/A Neulasta (pegfilgrastim) May be subject to quantity limit Neupogen (filgrastim) N/A Nivestym (filgrastim-aafi) N/A Nyvepria (pegfilgrastim-apgf) May be subject to quantity limit Udenyca (pegfilgrastim-cbqv) May be subject to quantity limit Zarxio (filgrastim-sndz) N/A Ziextenzo (pegfilgrastim-bmez) May be subject to quantity limit APPROVAL CRITERIA I. *In addition to criteria outlined below, requests for Granix, Leukine, Neupogen, Nivestym, must also meet the following criteria: A. Individual has had a trial and inadequate response or intolerance to Zarxio; OR B. Zarxio is not FDA-approved for the prescribed indication and Granix, Leukine, Neupogen or Nivestym is. *Step Therapy does not apply to Florida Healthy Kids II. Requests for filgrastim (Neupogen), filgrastim-aafi (Nivestym), or filgrastim-sndz (Zarxio) may be approved if the following criteria are met: A. Individual with nonmyeloid malignancy is using for primary prophylaxis of Febrile Neutropenia (FN); AND B. Individual has a risk of FN of 20% or greater based on chemotherapy regimen (see Appendix, Table 1); OR C. Individual with nonmyeloid malignancy is using for primary prophylaxis of FN; AND D. Individual’s risk of developing FN is greater than or equal to 10% and less than 20% based on chemotherapy regimen (see Appendix, Table 1) and individual has any risk factors for: PAGE 1 of 18 02/01/2021 This policy does not apply to health plans or member categories that do not have pharmacy benefits, nor does it apply to Medicare. -

CPIC Guideline for Pharmacogenetics-Guided Warfarin Dosing – Supplement V2.0 1 Table of Contents Guideline Updates
Supplement to: Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for Pharmacogenetics-guided Warfarin Dosing: 2016 Update Julie A. Johnson1, Kelly Caudle2, Li Gong3, Michelle Whirl-Carrillo3, C. Michael Stein4, Stuart A. Scott5, Ming Ta Michael Lee6 , Brian F. Gage7, Stephen E. Kimmel8,9, Minoli A. Perera10, Jeffrey L. Anderson11, Munir Pirmohamed12, Teri E. Klein3, Nita A. Limdi13, Larisa H. Cavallari1, Mia Wadelius14 1Department of Pharmacotherapy and Translational Research, College of Pharmacy, and Center for Pharmacogenomics, University of Florida, Gainesville, Florida, USA 2Department of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, Memphis, TN 3Department of Genetics, Stanford University, Stanford, California, USA 4Division of Clinical Pharmacology Vanderbilt Medical School, Nashville, TN, USA 5Department of Genetics and Genomic Sciences, Icahn School of Medicine at Mount Sinai, New York, NY, USA 6Laboratory for International Alliance on Genomic Research, RIKEN Center for Integrative Medical Sciences, Yokohama, Japan; National Center for Genome Medicine; Institute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan; Genomic Medicine Institute Geisinger Health system, Danville, PA 7Department of Internal Medicine, Washington University in St. Louis, St. Louis, Missouri 8Center for Clinical Epidemiology and Biostatistics, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania, USA 9Department of Medicine and Department of Biostatistics and Epidemiology, University of Pennsylvania -

Primary and Acquired Resistance to Immunotherapy in Lung Cancer: Unveiling the Mechanisms Underlying of Immune Checkpoint Blockade Therapy
cancers Review Primary and Acquired Resistance to Immunotherapy in Lung Cancer: Unveiling the Mechanisms Underlying of Immune Checkpoint Blockade Therapy Laura Boyero 1 , Amparo Sánchez-Gastaldo 2, Miriam Alonso 2, 1 1,2,3, , 1,2, , José Francisco Noguera-Uclés , Sonia Molina-Pinelo * y and Reyes Bernabé-Caro * y 1 Institute of Biomedicine of Seville (IBiS) (HUVR, CSIC, Universidad de Sevilla), 41013 Seville, Spain; [email protected] (L.B.); [email protected] (J.F.N.-U.) 2 Medical Oncology Department, Hospital Universitario Virgen del Rocio, 41013 Seville, Spain; [email protected] (A.S.-G.); [email protected] (M.A.) 3 Centro de Investigación Biomédica en Red de Cáncer (CIBERONC), 28029 Madrid, Spain * Correspondence: [email protected] (S.M.-P.); [email protected] (R.B.-C.) These authors contributed equally to this work. y Received: 16 November 2020; Accepted: 9 December 2020; Published: 11 December 2020 Simple Summary: Immuno-oncology has redefined the treatment of lung cancer, with the ultimate goal being the reactivation of the anti-tumor immune response. This has led to the development of several therapeutic strategies focused in this direction. However, a high percentage of lung cancer patients do not respond to these therapies or their responses are transient. Here, we summarized the impact of immunotherapy on lung cancer patients in the latest clinical trials conducted on this disease. As well as the mechanisms of primary and acquired resistance to immunotherapy in this disease. Abstract: After several decades without maintained responses or long-term survival of patients with lung cancer, novel therapies have emerged as a hopeful milestone in this research field. -

Trastuzumab Products
1 Trastuzumab Products: Trastuzumab (Herceptin®), Trastuzumab-anns (Kanjinti®), Trastuzumab-dkst (Ogivri®), Trastuzumab-dttb (Ontruzant®), Trastuzumab-pkrb (Herzuma®), Trastuzumab-qyyp (Trazimera®) Prior Authorization Drug Coverage Policy Effective Date: 11/9/2020 Revision Date: n/a Review Date: 10/27/2020 Lines of Business: Commercial Policy type: Prior Authorization This Drug Coverage Policy provides parameters for the coverage of trastuzumab products, which includes Trastuzumab (Herceptin®), Trastuzumab-anns (Kanjinti ®), Trastuzumab-dkst (Ogivri ®), Trastuzumab-dttb (Ontruzant®), Trastuzumab-pakrb (Herzuma®), and Trastuzumab-qyyp (Trazimera ®). Consideration of medically necessary indications are based upon U.S. Food and Drug Administration (FDA) indications, recommended uses within the Centers of Medicare & Medicaid Services (CMS) five recognized compendia, including the National Comprehensive Cancer Network (NCCN) Drugs & Biologics Compendium (NCCN Category 1 or 2A recommendations), and peer-reviewed scientific literature eligible for coverage according to the CMS, Medicare Benefit Policy Manual, Chapter 15, section 50.4.5 titled, “Off-Label Use of Anti- Cancer Drugs and Biologics.” This policy evaluates whether the drug therapy is proven to be effective based on published evidence-based medicine. Drug Description 1 The human epidermal growth factor receptor 2 (HER2) proto-oncogene encodes a transmembrane receptor protein of 185 kDa, which is structurally related to the epidermal growth factor receptor. Trastuzumab products have been shown, in both in vitro assays and in animals, to inhibit the proliferation of human tumor cells that overexpress HER2. Trastuzumab products are mediators of antibody-dependent cellular cytotoxicity (ADCC). In vitro , trastuzumab product mediated ADCC has been shown to be preferentially exerted on HER2 overexpressing cancer cells compared with cancer cells that do not overexpress HER2. -

Efavirenz) Capsules and Tablets 3 Rx Only
1 SUSTIVA® 2 (efavirenz) capsules and tablets 3 Rx only 4 DESCRIPTION 5 SUSTIVA® (efavirenz) is a human immunodeficiency virus type 1 (HIV-1) specific, non- 6 nucleoside, reverse transcriptase inhibitor (NNRTI). 7 Capsules: SUSTIVA is available as capsules for oral administration containing either 8 50 mg, 100 mg, or 200 mg of efavirenz and the following inactive ingredients: lactose 9 monohydrate, magnesium stearate, sodium lauryl sulfate, and sodium starch glycolate. 10 The capsule shell contains the following inactive ingredients and dyes: gelatin, sodium 11 lauryl sulfate, titanium dioxide, and/or yellow iron oxide. The capsule shells may also 12 contain silicon dioxide. The capsules are printed with ink containing carmine 40 blue, 13 FD&C Blue No. 2, and titanium dioxide. 14 Tablets: SUSTIVA is available as film-coated tablets for oral administration containing 15 600 mg of efavirenz and the following inactive ingredients: croscarmellose sodium, 16 hydroxypropyl cellulose, lactose monohydrate, magnesium stearate, microcrystalline 17 cellulose, and sodium lauryl sulfate. The film coating contains Opadry® Yellow and 18 Opadry® Clear. The tablets are polished with carnauba wax and printed with purple ink, 19 Opacode® WB. 20 Efavirenz is chemically described as (S)-6-chloro-4-(cyclopropylethynyl)-1,4-dihydro-4- 21 (trifluoromethyl)-2H-3,1-benzoxazin-2-one. 22 Its empirical formula is C14H9ClF3NO2 and its structural formula is: 1 of 45 Approved v2.0 F C 3 Cl O NO 23 H 24 Efavirenz is a white to slightly pink crystalline powder with a molecular mass of 315.68. 25 It is practically insoluble in water (<10 µg/mL). -

Modifications to the Harmonized Tariff Schedule of the United States To
U.S. International Trade Commission COMMISSIONERS Shara L. Aranoff, Chairman Daniel R. Pearson, Vice Chairman Deanna Tanner Okun Charlotte R. Lane Irving A. Williamson Dean A. Pinkert Address all communications to Secretary to the Commission United States International Trade Commission Washington, DC 20436 U.S. International Trade Commission Washington, DC 20436 www.usitc.gov Modifications to the Harmonized Tariff Schedule of the United States to Implement the Dominican Republic- Central America-United States Free Trade Agreement With Respect to Costa Rica Publication 4038 December 2008 (This page is intentionally blank) Pursuant to the letter of request from the United States Trade Representative of December 18, 2008, set forth in the Appendix hereto, and pursuant to section 1207(a) of the Omnibus Trade and Competitiveness Act, the Commission is publishing the following modifications to the Harmonized Tariff Schedule of the United States (HTS) to implement the Dominican Republic- Central America-United States Free Trade Agreement, as approved in the Dominican Republic-Central America- United States Free Trade Agreement Implementation Act, with respect to Costa Rica. (This page is intentionally blank) Annex I Effective with respect to goods that are entered, or withdrawn from warehouse for consumption, on or after January 1, 2009, the Harmonized Tariff Schedule of the United States (HTS) is modified as provided herein, with bracketed matter included to assist in the understanding of proclaimed modifications. The following supersedes matter now in the HTS. (1). General note 4 is modified as follows: (a). by deleting from subdivision (a) the following country from the enumeration of independent beneficiary developing countries: Costa Rica (b). -
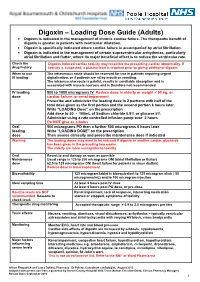
Digoxin – Loading Dose Guide (Adults) Digoxin Is Indicated in the Management of Chronic Cardiac Failure
Digoxin – Loading Dose Guide (Adults) Digoxin is indicated in the management of chronic cardiac failure. The therapeutic benefit of digoxin is greater in patients with ventricular dilatation. Digoxin is specifically indicated where cardiac failure is accompanied by atrial fibrillation. Digoxin is indicated in the management of certain supraventricular arrhythmias, particularly atrial fibrillation and flutter, where its major beneficial effect is to reduce the ventricular rate. Check the Digoxin-induced cardiac toxicity may resemble the presenting cardiac abnormality. If drug history toxicity is suspected, a plasma level is required prior to giving additional digoxin. When to use The intravenous route should be reserved for use in patients requiring urgent IV loading digitalisation, or if patients are nil by mouth or vomiting. The intramuscular route is painful, results in unreliable absorption and is associated with muscle necrosis and is therefore not recommended. IV loading 500 to 1000 micrograms IV Reduce dose in elderly or weight < 50 kg, or dose cardiac failure, or renal impairment Prescribe and administer the loading dose in 2 portions with half of the total dose given as the first portion and the second portion 6 hours later. Write “LOADING Dose” on the prescription Add dose to 50 - 100mL of Sodium chloride 0.9% or glucose 5% Administer using a rate controlled infusion pump over 2 hours Do NOT give as a bolus Oral 500 micrograms PO then a further 500 micrograms 6 hours later loading Write “LOADING DOSE” on the prescription dose Then assess clinically and prescribe maintenance dose if indicated Warning The loading doses may need to be reduced if digoxin or another cardiac glycoside has been given in the preceding two weeks.