PDF Version Here
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
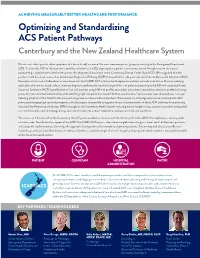
Optimizing and Standardizing ACS Patient Pathways Canterbury and the New Zealand Healthcare System
ACHIEVING MEASURABLY BETTER HEALTHCARE PERFORMANCE Optimizing and Standardizing ACS Patient Pathways Canterbury and the New Zealand Healthcare System Patients with chest pain (or other symptoms of a heart attack) are one of the most common patient groups presenting to the Emergency Department (ED). Traditionally, 90% of these patients would be admitted to the ED, exposing many patients to unnecessary risk through invasive testing and representing a large burden to the health system. An integrated clinical team at the Canterbury District Health Board (CDHB) recognized that the problem could be solved via use of an Accelerated Diagnostics Pathway (ADP) that enabled the safe early rule out of Acute Myocardial Infarction (AMI). Research partners and collaborations in accordance with the ICARE-ACS initiative led to expansive analytics and outcomes data in this area including application of evidence-based, safe, accelerated diagnostic pathways for rapid discharge of low-risk patients presenting to the ED with suspected Acute Coronary Syndrome (ACS). Identification of ‘low-risk’ patients using TIMI risk profiles and cardiac biomarkers measured on admission enabled discharge protocols that maximized patient safety while admitting high-risk patients in need of further care. Iterative improvements were observed year over year following adoption of the EDACS risk score and using more sensitive cardiac biomarkers. While maximum discharge rates can be observed with ADP processes leveraging high sensitivity troponin, safe discharge is also possible using point of care. Implementation of these ADP pathways have positively impacted Key Performance Indictors (KPIs) throughout the Canterbury Health System including median length of stay, number of patients transported to central hospitals, cost of prolonged stays and cost of transports, patient satisfaction, and increased clinician confidence. -

Name of Recognized Medical Schools (Foreign)
1 Name of Recognized Medical Schools (Foreign) Expired AUSTRALIA 1 School of Medicine, Faculty of Heath, University of Tasmania, Tasmania, Australia (5 years Program) 9 Jan Main Affiliated Hospitals 2021 1. Royal H obart Hospital 2. Launceston Gen Hospital 3. NWest Region Hospital 2 Melbourne Medical School, University of Melbourne, Victoria, Australia (4 years Program) 1 Mar Main Affiliated Hospitals 2022 1. St. Vincent’s Public Hospital 2. Epworth Hospital Richmond 3. Austin Health Hospital 4. Bendigo Hospital 5. Western Health (Sunshine, Footscray & Williamstown) 6. Royal Melbourne Hospital Affiliated Hospitals 1. Pater MacCallum Cancer Centre 2. Epworth Hospital Freemasons 3. The Royal Women’s Hospital 4. Mercy Hospital for Women 5. The Northern Hospital 6. Goulburn Valley Health 7. Northeast Health 8. Royal Children’s Hospital 3 School of Medicine and Public Health, University of Newcastle, New South Wales, Australia (5 years Program) 3 May Main Affiliated Hospitals 2022 1.Gosford School 2. John Hunter Hospital Affiliated Hospitals 1. Wyong Hospital 2. Calvary Mater Hospital 3. Belmont Hospital 4. Maitland Hospital 5. Manning Base Hospital & University of Newcastle Department of Rural Health 6. Tamworth Hospital 7. Armidale Hospital 4 Faculty of Medicine, Nursing and Health Sciences, Monash University, Australia (4 and 5 years Program) 8 Nov Main Affiliated Hospitals 1. Eastern Health Clinical School: EHCS 5 Hospitals 2022 2. Southern School for Clinical Sciences: SCS 5 Hospitals 3. Central Clinical School จ ำนวน 6 Hospitals 4. School of Rural Health จ ำนวน 7 Hospital 5 Sydney School of Medicine (Sydney Medical School), Faculty of Medicine and Health, University of Sydney, Australia 12 Dec (4 years Program) 2023 2 Main Affiliated Hospitals 1. -

Adapting to Institutional Change in New Zealand Politics
21. Taming Leadership? Adapting to Institutional Change in New Zealand Politics Raymond Miller Introduction Studies of political leadership typically place great stress on the importance of individual character. The personal qualities looked for in a New Zealand or Australian leader include strong and decisive action, empathy and an ability to both reflect the country's egalitarian traditions and contribute to a growing sense of nationhood. The impetus to transform leaders from extraordinary people into ordinary citizens has its roots in the populist belief that leaders should be accessible and reflect the values and lifestyle of the average voter. This fascination with individual character helps account for the sizeable biographical literature on past and present leaders, especially prime ministers. Typically, such studies pay close attention to the impact of upbringing, personality and performance on leadership success or failure. Despite similarities between New Zealand and Australia in the personal qualities required of a successful leader, leadership in the two countries is a product of very different constitutional and institutional traditions. While the overall trend has been in the direction of a strengthening of prime ministerial leadership, Australia's federal structure of government allows for a diffusion of leadership across multiple sources of influence and power, including a network of state legislatures and executives. New Zealand, in contrast, lacks a written constitution, an upper house, or the devolution of power to state or local government. As a result, successive New Zealand prime ministers and their cabinets have been able to exercise singular power. This chapter will consider the impact of recent institutional change on the nature of political leadership in New Zealand, focusing on the extent to which leadership practices have been modified or tamed by three developments: the transition from a two-party to a multi-party parliament, the advent of coalition government, and the emergence of a multi-party cartel. -

Bromley Cemetery Guide
Bromley Cemetery Tour Compiled by Richard L. N. Greenaway June 2007 Block 1A Row C No. 33 Hurd Born at Hinton, England, Frank James Hurd emigrated with his parents. He worked as a contractor and, in 1896, in Wellington, married Lizzie Coker. The bride, 70, claimed to be 51 while the groom, 40, gave his age as 47. Lizzie had emigrated on the Regina in 1859 with her cousin, James Gapes (later Mayor of Christchurch) and his family and had already been twice-wed. Indeed, the property she had inherited from her first husband, George Allen, had enabled her second spouse, John Etherden Coker, to build the Manchester Street hotel which bears his name. Lizzie and Frank were able to make trips to England and to Canada where there dwelt Lizzie’s brother, once a member of the Horse Guards. Lizzie died in 1910 and, two years later, Hurd married again. He and his wife lived at 630 Barbadoes Street. Hurd was a big man who, in old age he had a white moustache, cap and walking stick. He died, at 85, on 1 April 1942. Provisions of Lizzie’s will meant that a sum of money now came to the descendants of James Gapes. They were now so numerous that the women of the tribe could spend their inheritance on a new hat and have nothing left over. Block 2 Row B No. 406 Brodrick Thomas Noel Brodrick – known as Noel - was born in London on 25 December 1855. In 1860 the Brodricks emigrated on the Nimrod. As assistant to Canterbury’s chief surveyor, J. -

Fallsstop – Free Seminar About Falls Reduction with Anne-Marie Hill
FallsStop – free seminar about falls reduction with Anne-Marie Hill SaveSave the the date date Essential HelpCare is kindly sponsoring this seminar to allow free entry. FallsStop is a free seminar about reducing falls in the hospital setting, designed for hospital falls champions, nursing management, and physiotherapy, gerontology and aged care representatives. Guest speaker Associate Professor Anne-Marie Hill will cover various topics including: • evidence-based positive outcomes • patient engagement • individualised approaches • an overview of falls prevention work in Western Australia (WA). The seminar includes presentations from local falls prevention leaders and members of Whanganui District Health Board’s (DHB) ‘care with dignity’ team. ‘Care with dignity’ has been highly successful in reducing harm from in-hospital falls among patients with cognitive impairment. Assoc Prof Hill will run a physiotherapy-specific session during the lunch break. This is a professional gathering and an opportunity to have lunch and an informal discussion with a gerontological physiotherapist and ask about Anne-Marie’s work. Four seminars will be held between 3 and 7 April 2017, in the following locations: • Dunedin, Monday 3 April – Southern DHB, Wakari Hospital, Board Room, Level 3, Main Block, 369 Taieri Road, Halfway Bush, Dunedin • Wellington, Tuesday 4 April – Nordmeyer Theatre, University of Otago, Wellington Hospital, 23A Mein Street, Wellington • Auckland, Thursday 6 April – Auckland DHB, Fisher & Paykel Healthcare Clinical Education Centre, Level 5, Auckland City Hospital, 2 Park Road, Auckland • Counties Manukau, Friday 7 April – Ko Awatea, Middlemore Hospital, 100 Hospital Road, Auckland. Attendees from across the health and disability sector are welcome. To register go to: https:// app.smartsheet.com/b/form?EQBCT=cfa0ae6e15ac4b548a566233e13d7abd or phone 0800 331 332. -
Association of Incident Dialysis Modality with Mortality: a Protocol for Systematic Review and Meta-Analysis of Randomized Controlled Trials and Cohort Studies Mark R
Marshall et al. Systematic Reviews (2019) 8:55 https://doi.org/10.1186/s13643-019-0972-1 PROTOCOL Open Access Association of incident dialysis modality with mortality: a protocol for systematic review and meta-analysis of randomized controlled trials and cohort studies Mark R. Marshall1,2,3* , Chun-Yuan Hsiao2, Philip K. Li4, Masaaki Nakayama5,6, S. Rabindranath7, Rachael C. Walker8, Xueqing Yu9,10 and Suetonia C. Palmer11 Abstract Background: At least 2.6 million adults and children receive dialysis treatment for end-stage kidney disease (ESKD) worldwide. The large majority of these receive hemodialysis (HD), while the remaining receive peritoneal dialysis (PD). Peritoneal dialysis may be associated with similar mortality outcomes as HD, and patient-reported outcomes are potentially increased with PD. Existing evidence for the mortality associated with PD was summarized over 20 years ago, and there has been greater marginal improvement in survival with PD relative to HD since that time. It is therefore timely to reexamine the question of differential mortality by modality and summarize evidence from more contemporary practice settings. Methods/design: Electronic databases will be systematically searched for publications that report the association between dialysis modality (HD or PD) with death from any cause and cause-specific death in incident patients with end-stage kidney disease. The database searches will be supplemented by searching through citations and references and consultation with experts. Studies published before 1995 will be excluded. Screening of both titles and abstracts will be done by two independent reviewers. All disagreements will be resolved by an independent third reviewer. A quantitative meta-analysis of effect sizes and standard errors will be applied. -

'About Turn': an Analysis of the Causes of the New Zealand Labour Party's
Newcastle University e-prints Date deposited: 2nd May 2013 Version of file: Author final Peer Review Status: Peer reviewed Citation for item: Reardon J, Gray TS. About Turn: An Analysis of the Causes of the New Zealand Labour Party's Adoption of Neo-Liberal Policies 1984-1990. Political Quarterly 2007, 78(3), 447-455. Further information on publisher website: http://onlinelibrary.wiley.com Publisher’s copyright statement: The definitive version is available at http://onlinelibrary.wiley.com at: http://dx.doi.org/10.1111/j.1467-923X.2007.00872.x Always use the definitive version when citing. Use Policy: The full-text may be used and/or reproduced and given to third parties in any format or medium, without prior permission or charge, for personal research or study, educational, or not for profit purposes provided that: A full bibliographic reference is made to the original source A link is made to the metadata record in Newcastle E-prints The full text is not changed in any way. The full-text must not be sold in any format or medium without the formal permission of the copyright holders. Robinson Library, University of Newcastle upon Tyne, Newcastle upon Tyne. NE1 7RU. Tel. 0191 222 6000 ‘About turn’: an analysis of the causes of the New Zealand Labour Party’s adoption of neo- liberal economic policies 1984-1990 John Reardon and Tim Gray School of Geography, Politics and Sociology Newcastle University Abstract This is the inside story of one of the most extraordinary about-turns in policy-making undertaken by a democratically elected political party. -

New Zealand Out-Of-Hospital Acute Stroke Destination Policy Northland and Auckland Areas
New Zealand Out-of-Hospital Acute Stroke Destination Policy Northland and Auckland Areas This policy is for the use of clinical personnel when determining the destination hospital for patients with an acute stroke in the out-of-hospital setting in the Northland and Auckland areas of New Zealand. It has been developed by the Northern Region Stroke Network in conjunction with the National Stroke Network and the Ambulance Sector. Publication date October 2020 Acute Stroke Destination Flowchart: Auckland Area Does the patient have signs or symptoms Stroke is unlikely, treat of an acute stroke? NO appropriately without YES using this policy. Perform additional screening using the PASTA tool Will the patient arrive at: NO NO A stroke hospital within 4 hours Does the patient Transport to the of symptom onset, or meet ‘wake-up’ most appropriate Auckland City Hospital within stroke criteria?1 hospital. 6 hours of symptom onset? YES YES Transport to the catchment YES PASTA positive? NO area hospital and notify hospital personnel of the Patient will arrive in ED 0800–1600, Mon–Fri following information: PASTA results and Transport to the most appropriate stroke hospital and notify hospital personnel as below: FAST results and Time of symptom onset and North Shore Hospital. Auckland City Hospital. NHI number Waitakere Hospital. Middlemore Hospital. Out of hours If the patient is in the North Shore Hospital, Notify hospital personnel Waitakere Hospital or Middlemore Hospital ASAP and provide the catchment: following information as a – Phone the on-call neurologist at Auckland City minimum: Hospital on 0800 1 PASTA as per the PASTA tool. -

Emergency Nurse New Zealand
August | 2018 EMERGENCY NURSE NEW ZEALAND The Journal of the College of Emergency Nurses New Zealand (NZNO) ISSN 1176-2691 EMERGENCY NURSE NEW ZEALAND COLLEGE OF EMERGENCY NURSES NEW ZEALAND - NZNO AUGUST 2018 In this issue Features Compassion fatigue: CENNZ National P 6 P 12 the cost of caring Committee Nominations Author: Suzanne Hamilton What is the AENN Group? P 30 Understanding Some P 8 Commonly Used Statistics: Diagnostic Studies Snippets Winter 2018 Author: Jane Key P 31 Regulars A Word from Regional Reports P 3 P 13 the Editor Chairperson’s NEW FEATURE P 5 P 29 Report What are you looking at? P 2 EMERGENCY NURSE NEW ZEALAND COLLEGE OF EMERGENCY NURSES NEW ZEALAND - NZNO AUGUST 2018 A Word from the Editor: nursing education has seldom been Editorial Committee raised. I understand the issues of safe Matt Comeskey staffing and pay equity are important and Emergency Nurse N.Z. is the official Editor | Emergency Nurse NZ immediate concerns – but it saddens me journal of the College of Emergency [email protected] that the erosion of our ongoing education Nurses of New Zealand (CENNZ) / Letters to the Editor are welcome. Letters should is not being addressed. We need to be New Zealand Nurses Organisation be no more than 500 words, with no more than 5 vigilant that we don’t undermine the references and no tables or figures. (NZNO). The views expressed in this value of our professional development by focusing exclusively on equally critical publication are not necessarily those of Welcome to this, the first digital edition issues. -

Immigration During the Crown Colony Period, 1840-1852
1 2: Immigration during the Crown Colony period, 1840-1852 Context In 1840 New Zealand became, formally, a part of the British Empire. The small and irregular inflow of British immigrants from the Australian Colonies – the ‘Old New Zealanders’ of the mission stations, whaling stations, timber depots, trader settlements, and small pastoral and agricultural outposts, mostly scattered along the coasts - abruptly gave way to the first of a number of waves of immigrants which flowed in from 1840.1 At least three streams arrived during the period 1840-1852, although ‘Old New Zealanders’ continued to arrive in small numbers during the 1840s. The first consisted of the government officials, merchants, pastoralists, and other independent arrivals, the second of the ‘colonists’ (or land purchasers) and the ‘emigrants’ (or assisted arrivals) of the New Zealand Company and its affiliates, and the third of the imperial soldiers (and some sailors) who began arriving in 1845. New Zealand’s European population grew rapidly, marked by the establishment of urban communities, the colonial capital of Auckland (1840), and the Company settlements of Wellington (1840), Petre (Wanganui, 1840), New Plymouth (1841), Nelson (1842), Otago (1848), and Canterbury (1850). Into Auckland flowed most of the independent and military streams, and into the company settlements those arriving directly from the United Kingdom. Thus A.S.Thomson observed that ‘The northern [Auckland] settlers were chiefly derived from Australia; those in the south from Great Britain. The former,’ he added, ‘were distinguished for colonial wisdom; the latter for education and good home connections …’2 Annexation occurred at a time when emigration from the United Kingdom was rising. -

REFERENCE LIST: 10 (4) Legat, Nicola
REFERENCE LIST: 10 (4) Legat, Nicola. "South - the Endurance of the Old, the Shock of the New." Auckland Metro 5, no. 52 (1985): 60-75. Roger, W. "Six Months in Another Town." Auckland Metro 40 (1984): 155-70. ———. "West - in Struggle Country, Battlers Still Triumph." Auckland Metro 5, no. 52 (1985): 88-99. Young, C. "Newmarket." Auckland Metro 38 (1984): 118-27. 1 General works (21) "Auckland in the 80s." Metro 100 (1989): 106-211. "City of the Commonwealth: Auckland." New Commonwealth 46 (1968): 117-19. "In Suburbia: Objectively Speaking - and Subjectively - the Best Suburbs in Auckland - the Verdict." Metro 81 (1988): 60-75. "Joshua Thorp's Impressions of the Town of Auckland in 1857." Journal of the Auckland Historical Society 35 (1979): 1-8. "Photogeography: The Growth of a City: Auckland 1840-1950." New Zealand Geographer 6, no. 2 (1950): 190-97. "What’s Really Going On." Metro 79 (1988): 61-95. Armstrong, Richard Warwick. "Auckland in 1896: An Urban Geography." M.A. thesis (Geography), Auckland University College, 1958. Elphick, J. "Culture in a Colonial Setting: Auckland in the Early 1870s." New Zealand Journal of Educational Studies 10 (1974): 1-14. Elphick, Judith Mary. "Auckland, 1870-74: A Social Portrait." M.A. thesis (History), University of Auckland, 1974. Fowlds, George M. "Historical Oddments." Journal of the Auckland Historical Society 4 (1964): 35. Halstead, E.H. "Greater Auckland." M.A. thesis (Geography), Auckland University College, 1934. Le Roy, A.E. "A Little Boy's Memory of Auckland, 1895 to Early 1900." Auckland-Waikato Historical Journal 51 (1987): 1-6. Morton, Harry. -
BMJ Open Is Committed to Open Peer Review. As Part of This Commitment We Make the Peer Review History of Every Article We Publish Publicly Available
BMJ Open: first published as 10.1136/bmjopen-2018-025253 on 5 May 2019. Downloaded from BMJ Open is committed to open peer review. As part of this commitment we make the peer review history of every article we publish publicly available. When an article is published we post the peer reviewers’ comments and the authors’ responses online. We also post the versions of the paper that were used during peer review. These are the versions that the peer review comments apply to. The versions of the paper that follow are the versions that were submitted during the peer review process. They are not the versions of record or the final published versions. They should not be cited or distributed as the published version of this manuscript. BMJ Open is an open access journal and the full, final, typeset and author-corrected version of record of the manuscript is available on our site with no access controls, subscription charges or pay-per-view fees (http://bmjopen.bmj.com). If you have any questions on BMJ Open’s open peer review process please email [email protected] http://bmjopen.bmj.com/ on October 2, 2021 by guest. Protected copyright. BMJ Open BMJ Open: first published as 10.1136/bmjopen-2018-025253 on 5 May 2019. Downloaded from Comparing the variants of takotsubo syndrome: an observational study of the electrocardiogram and structural changes. ForJournal: peerBMJ Open review only Manuscript ID bmjopen-2018-025253 Article Type: Research Date Submitted by the Author: 05-Jul-2018 Complete List of Authors: Watson, George; Christchurch Hospital, Cardiology Chan, Christina; Christchurch Hospital, Cardiology Belluscio, Laura; Christchurch Hospital, Biostatistics Doudney, Kit; Canterbury District Health Board, Molecular Pathology Lacey, Cameron; Christchurch Hospital, Psychological Medicine Kennedy, Martin; University of Otago, Department of Pathology Bridgman, Paul; Christchurch Hospital, Cardiology Echocardiography < CARDIOLOGY, Heart failure < CARDIOLOGY, Keywords: Cardiomyopathy < CARDIOLOGY, Takotsubo http://bmjopen.bmj.com/ on October 2, 2021 by guest.