Quality Early Education and Child Care from Birth to Kindergarten
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Family Handbook: 2018
Faith Christian Academy Family Handbook: 2018 “Training Students…Transforming Lives” Family Handbook: 2018 Table of Contents I. Philosophy, Foundations, and Admissions 5 Accreditation 5 Admission Information 5 Admissions Procedures 5 Admissions Procedures/Requirements by Grade Level 6 Immunizations 6 Non Discrimination Policy 6 Students with Special Academic Needs 6 Students with Court Records 7 Students with Infectious Diseases 7 Core Values 7 Expected Student Outcomes 8 History 9 Mission Statement 9 Organization 9 Potential for Revision 10 Statement of Faith 10 Statement of Purpose and Philosophy of Education 14 Vision Statement 15 II. Academic Information 16 Academic Eligibility ..............................................................................................16 Academic Fairs and Competitions .........................................................................16 Cheating/Academic Integrity .................................................................................16 Christian/Community Service Recognition ...........................................................16 College Courses/Dual Credits ................................................................................16 Curriculum Guides .................................................................................................17 Grading System ......................................................................................................17 Graduation Requirements ......................................................................................17 -

School Profile 2019-2020
SCHOOL PROFILE 2019-2020 10 MAIN STREET Cheshire Academy was founded in 1794. The Academy is a selective independent, coeducational CHESHIRE, CT 06410 boarding and day school enrolling 362 students in grades 9-12 and a postgraduate year. Cheshire Academy endeavors to enroll students who are eager to pursue their passions and realize their potential. 203-272-5396 The Academy has a rich tradition of enrolling a diverse student body and providing a student-centered FAX: 203-439-7202 program. Cheshire Academy is accredited by the New England Association of Schools and Colleges CEEB CODE: 070095 and is approved by the Connecticut State Department of Education. Among other affiliations, the school is a member of the Secondary School Admissions Test Board (SSATB) the National Association of WWW.CHESHIREACADEMY.ORG Independent Schools (NAIS) and the Connecticut Association of Independent Schools (CAIS). * ADMINISTRATION CHESHIRE ACADEMY AT A GLANCE Julie Anderson • 362 students, 57% boys, 43% girls • 57 full time faculty Head of School • 16 PGs, 108 Seniors, 94 Juniors, • 46 with advanced degrees (up to M.A.) 94 Sophomores, 50 Freshmen • Average class size: 11 Laura Longacre • 51% boarding, 49% day Chief Academic Officer • From13 states and 29 countries * As of September 1, 2018 GPA DISTRIBUTION—CLASS OF 2019 * COLLEGE COUNSELING OFFICE ACADEMIC INFORMATION & GRADUATION REQUIREMENTS 4.1-4.0 2.4 % of class Madeleine Bergstrom • Semester system 3.99-3.67 17.1 % of class Director • Over 110 courses offered in 6 disciplines 3.66.-3.33 25.2 % of class 203-439-7550 • International Baccalaureate® Diploma Programme 3.32-3.0 18.7 % of class [email protected] 2.99-2.67 17.1 % of class CLASS RANK & GPA 2.66-2.33 15.4 % of class Laura Dempsey Beginning with the 2016-2017 academic year, Senior Associate Director Cheshire Academy no longer applies weight to 2.32-and under 4.1 % of class 203-439-7294 the student GPA. -

Investigation Into University Technical Colleges
A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department for Education Investigation into university technical colleges HC 101 SESSION 2019-20 30 OCTOBER 2019 4 What this investigation is about Investigation into university technical colleges What this investigation is about 1 University technical colleges (UTCs) are a type of free school in England that focuses on teaching students who are mainly aged 14 to 19. UTCs are publicly funded state schools, independent of local authorities. Each UTC must be part of an academy trust, a charitable company that manages the school’s budget and employs the staff. Academy trusts are directly funded by, and accountable to, the Department for Education (the Department), via the Education and Skills Funding Agency. Single-academy trusts have one academy school, while multi-academy trusts bring together groups of academy schools. 2 In 2010, the government undertook to improve the quality of vocational education, including increasing flexibility for 14- to 19-year-olds and creating new technical academies as part of plans to diversify school provision.1 The Department supported the establishment of the first UTC in 2010/11 and the government announced its ambitions for UTCs in subsequent budgets.2 The Department’s vision was for employers and universities to work together, with educational experts, to open new institutions to deliver technical education in specialist areas that meets the needs of local employers and the economy. 3 However, UTCs have faced challenges that have threatened their viability. In December 2016, we reported that the then Education Funding Agency had assessed 22 of 47 UTCs as at risk due to financial concerns.3 The financial difficulties were caused, at least in part, by the fact that UTCs had fewer students than predicted. -

LANGSTON UNIVERSITY TRANSPORTATION ACADEMY FREQUENTLY ASKED QUESTIONS What Is the Langston Transportation Academy? the Langston
LANGSTON UNIVERSITY TRANSPORTATION ACADEMY FREQUENTLY ASKED QUESTIONS What is the Langston Transportation Academy? The Langston University Transportation Academy (the Academy) is funded by the Southern Plains Transportation Center (SPTC) and is supported by many public and private transportation agencies and companies to provide high school students an opportunity to learn about the transportation industry and to strengthen and increase participation of Minority Institutions of Higher Learning in federal programs. The threefold-purpose is to: (1) Create awareness and stimulate interest in secondary school students to take maximum advantage of the career opportunities in the transportation industry; (2) Attract a broad and diverse selection of bright minds, and acquaint and stimulate them with the various aspects of the transportation industry; and (3) Increase the number of students who choose careers in the transportation industry. Who is eligible to apply? Any student who is a citizen or permanent resident of the United States and who is currently enrolled in grade 9 or 10 is eligible. The student must have at least a cumulative grade point average (GPA) of 2.5, have interest in attending college/university/technical school, express interest in pursuing a career in transportation or transportation-related field, agree to participate for the whole duration of the residential program, and submit a complete application. When is the Academy held? The Academy is conducted in the month of June, for four weeks. How much does it cost to participate? The Academy is free of charge to participants. Is the Academy a day camp? No, the Academy is a two-week residential program. -
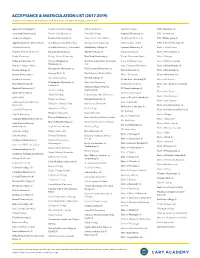
Acceptance & Matriculation List (2017-2019)
ACCEPTANCE & MATRICULATION LIST (2017-2019) Schools in bold indicate matriculation, with the number of students attending in parentheses. Agnes Scott College (1) Florida Southern College Mercer University Spelman College UNC-Charlotte (5) American University (1) Florida State University Meredith College Stanford University (2) UNC-Greensboro Amherst College (1) Fordham University (2) Miami University of Ohio Stony Brook University UNC-Wilmington (1) Appalachian State University (3) Franklin and Marshall College Michigan State University SUNY College of ESF UNC-School of the Arts (1) Auburn University Franklin University, Switzerland Middlebury College (1) Syracuse University (1) Univ. of North Texas Baldwin Wallace University Furman University (1) The New School (5) Temple University Univ. of Notre Dame (1) Baylor University George Mason University New York University (3) Temple University, Japan Univ. of Oregon Belmont University (1) George Washington North Carolina State University Texas A&M University Univ. of Ottawa, Canada University (3) (34) Berklee College of Music Texas Christian University Univ. of Pennsylvania (1) Georgetown University (1) Northeastern University (2) Boston College (1) Tufts University (6) Univ. of Pittsburgh (1) Georgia Tech (2) Northwestern University (1) Boston University (3) Tulane University Univ. of Richmond (4) Gettysburg College Oberlin College (3) Brandeis University US Air Force Academy (1) Univ. of Rochester Goldsmiths, University of Ohio State University Brown University (5) US Military Academy Univ. of St. Andrews, Scotland London (1) Oxford College of Emory (1) Bucknell University (1) US Naval Academy (1) Goucher College University (1) Univ. of San Diego Butler University (2) University of Arizona Guilford College Pennsylvania State University Univ. of San Francisco Cal Tech (2) Univ. -
Opening a Studio School a Guide for Studio School Proposer Groups on the Pre-Opening Stage
Opening a studio school A guide for studio school proposer groups on the pre-opening stage August 2014 Contents Introduction 3 Section 1 - Who does what - roles and responsibilities? 5 Section 2 - Managing your project 10 Section 3 – Governance 12 Section 4 - Pupil recruitment and admissions 21 Section 5 - Statutory consultation 33 Section 6 - Staffing and education plans 36 Section 7 - Site and buildings 42 Section 8 – Finance 56 Section 9 - Procurement and additional support 63 Section 10 - Funding Agreement 67 Section 11 - The equality duty 71 Section 12 - Preparing to open 73 Section 13 - Once your school is open 80 Annex A - RSC regions and Local authorities 82 2 Introduction Congratulations! All your planning and preparation has paid off, and the Secretary of State for Education has agreed that your application to open a studio school should move to the next stage of the process – known as the ‘pre-opening’ stage. This is the stage between the approval of your application and the opening of the school. The setting up of a studio school is a challenging but ultimately very rewarding task and it will require significant commitment and time from sponsors and partners. Your original application set out your plans for establishing the studio school, from the education vision and the admission of pupils to the recruitment of staff and the curriculum. Now your application has been approved, you must begin work to implement these plans. The letter of approval you received from the Department for Education (DfE) sets out important conditions of approval. It is vital that you consider these conditions carefully in planning your priorities and what you need to focus on next. -

Academy of Art University Transfer Guide for San Jose City College
Academy of Art University Transfer Guide for San Jose City College Academy of Art University will consider following courses from San Jose City College towards fulfillment of the Liberal Arts graduation requirements for the Bachelor of Fine Arts (BFA) or Bachelor of Arts (BA) degrees. Students are encouraged to contact their Admissions Representative prior to registration to ensure direct transfer of coursework. Coursework must be successfully completed with a minimum letter grade of “C” or above to be evaluated for transfer of credit to Academy of Art University. Official transfer evaluations are based on the current transfer policies during the student’s semester of admission and will be binding for their entire matriculation. Units completed at another institution after the student has started a degree program at Academy of Art University will not be considered for transfer. Academy of Art University Course San Jose City College Equivalent LA 108: Composition for the Artist ENGL 001A English Composition Written ENGL 001B English Composition [or] Communication LA 202: English Composition: Creative Persuasion & Argument ENGL 001C Critical Thinking/Composition Art Historical LA 120: Art History through the 15th ART 091 Survey of Art History: Prehistoric Through Gothic Awareness Century Historical LA 171: Western Civilization HIST 010A Development of Western Culture [or] Awareness Only 1 Course LA 270: U.S. History HIST 017B History of the United States Quantitative LA 255: College Math MATH 051 Mathematics for General Education [or] Literacy -
Academy Articles of Association: Model One for Use by Mainstream, Special, 16-19, Alternative Provision Academies and Free Schools; and Studio Schools
Academy articles of association: model one For use by mainstream, special, 16-19, alternative provision academies and free schools; and studio schools February 2016 ACADEMY ARTICLES OF ASSOCIATION MODEL ONE For use by mainstream, special, 16-19, alternative provision, free and studio schools Contents Contents 2 INTERPRETATION 5 OBJECTS 8 GENERAL MEETINGS 18 NOTICE OF GENERAL MEETINGS 18 PROCEEDINGS AT GENERAL MEETINGS 19 PARENT TRUSTEES 24 CO-OPTED TRUSTEES 26 TERM OF OFFICE 26 SUSPENSION 27 DISQUALIFICATION OF TRUSTEES 28 CLERK TO THE TRUSTEES 30 CHAIRPERSON AND VICE-CHAIRPERSON OF THE TRUSTEES 30 POWERS OF TRUSTEES 31 CONFLICTS OF INTEREST 32 THE MINUTES 33 COMMITTEES 33 DELEGATION 34 CHIEF EXECUTIVE OFFICER AND PRINCIPALS 34 MEETINGS OF THE TRUSTEES 34 PATRONS AND HONORARY OFFICERS 38 THE SEAL 38 ACCOUNTS 38 ANNUAL REPORT 39 ANNUAL RETURN 39 NOTICES 39 INDEMNITY 40 RULES 40 2 ACADEMY ARTICLES OF ASSOCIATION MODEL ONE For use by mainstream, special, 16-19, alternative provision, free and studio schools AVOIDING INFLUENCED COMPANY STATUS 41 THE COMPANIES ACT 2006 A COMPANY LIMITED BY GUARANTEE ARTICLES OF ASSOCIATION OF MOORLANDS LEARNING TRUST COMPANY NUMBER: 07663864 3 ACADEMY ARTICLES OF ASSOCIATION MODEL ONE For use by mainstream, special, 16-19, alternative provision, free and studio schools THE COMPANIES ACT 2006 COMPANY LIMITED BY GUARANTEE ARTICLES OF ASSOCIATION OF MOORLANDS LEARNING TRUST 4 ACADEMY ARTICLES OF ASSOCIATION MODEL ONE For use by mainstream, special, 16-19, alternative provision, free and studio schools INTERPRETATION 1. In these Articles:- a. Not used; b. “the Academies" means all the schools and educational institutions referred to in Article 4a and operated by the Academy Trust (and “Academy” shall mean any one of those schools or educational institutions); c. -
University Technical Colleges How to Apply
University technical colleges How to apply October 2015 Contents 1. Things to know before you start 4 Vision 4 UTCs: law and policy 6 2. Getting started 10 Organising your group 10 Establishing your academy trust 12 Financial accountability 13 Conflicts of interest 14 Recruiting trustees 15 Suitability of applicants and applications 16 Priority locations for UTCs 16 Area-based reviews of post-16 institutions 17 3. Preparing and submitting your application 19 What happens when 19 Submitting your application 19 4. Application assessment and interviews 20 Assessment of your application 20 Interviews 20 Decisions and pre-opening 20 Appeals and reapplying 22 5. Application form sections and criteria 23 Section A: Applicant details 23 Section B: Outline of the school 23 Section C: Education vision 23 Section D: Education plan 26 Section E: Evidence of need and demand 30 Section F: Capacity and capability 31 Section G: Budget planning and affordability 40 2 Section H: Premises and Equipment 43 6. Support for applicants 45 Useful contacts 45 Further information and key documents 45 Annex A: Completing the 2014/15 financial template 47 Budget 47 The template 48 Annex B: Glossary of terms 52 3 1. Things to know before you start Vision 1.1 The government wants to improve our education system so that all children thrive and prosper, regardless of their background. The university technical college (UTC) programme, alongside the free schools programme, is helping us realise this vision. UTCs provide an opportunity for employers and universities to work together, with educational experts, to open new institutions that deliver high quality technical education in a range of specialist areas. -

Faith Academy 2020-2021 Confidence in Our Community
Faith Academy 2020-2021 Confidence in our Community Throughout the past few months, our constant prayer for all of us has been that "the peace of God, which transcends all understanding, will guard our hearts and minds in Christ Jesus." As we have wrestled with what's happening in our world and what our response to the pandemic should be, we have certainly been in need of God's peace. Faith Academy's mission and purpose remain stronger than ever during these challenging times. According to TEA, "Research from the Centers for Disease Control (CDC), among others, has found that while children do get infected by COVID-19 and some severe outcomes have been reported in children, relatively few children with COVID-19 are hospitalized or have severe symptoms. Furthermore, the American Academy of Pediatrics notes that COVID-19 risks must be balanced with the need for children to attend school in person, given that lack of physical access to school leads to a number of negative consequences." We appreciate your patience and understanding as we continue to be thoughtful and comprehensive in our approach to welcoming everyone back to campus. Over the past few months, our Executive Leadership Team and Academic Team have developed and continue to refine not only our return to campus for the 2020-2021 school year, but also both safety and learning continuity for our students and staff. Campus Opens Aug. 18 Faith Academy's re-entry process is guided by careful consideration of our School Board, NAUMS, ACSI, TEA, TAPPS, Governor Abbott and our local officials. -

American Dance Academy 2020/2021 Handbook
American Dance Academy 2020/2021 Handbook A Guide for Students and Parents American Dance Academy Handbook A Guide for Students and Parents As a condition of enrollment at American Dance Academy (ADA) students and their parents or guardians agree to abide by all the policies set forth by ADA, its director, faculty, and staff. ADA reserves the right to terminate any student’s enrollment at any time for misconduct or inappropriate actions by either the student or his or her parent(s). Welcome to American Dance Academy! This handbook will serve as your guide to American Dance Academy and its philosophy of dance education. We take our roles as mentors and teachers in your child’s life very seriously. It is our objective to inspire a passion for the art of dance in every child who passes through our doors. In the process, we strive to set the right example and help your child (and you) create memories that will last a lifetime. Philosophy American Dance Academy is committed to providing high-quality dance classes to enhance the overall development of the child. We provide a safe and child-centered environment to encourage our students to explore dance with qualified, nurturing teachers. We believe that dance training encourages young people to develop a positive self- image as they increase awareness of their physical being. Along with improving coordination skills and developing muscular awareness, dance classes give children the freedom to express themselves through movement. The highest educational standards are expected from all American Dance Academy faculty members. They are lifelong learners who continue to educate themselves through certification programs, teacher-training schools, conferences, and other learning opportunities. -

Academies, Autonomy, Equality and Democratic Accountability: Reforming the Fragmented Publicly Funded School System in England’
West, A. and Wolfe, D. (2019) ‘Academies, autonomy, equality and democratic accountability: Reforming the fragmented publicly funded school system in England’. London Review of Education, 17 (1): 70–86. DOI https://doi.org/10.18546/LRE.17.1.06 Academies, autonomy, equality and democratic accountability: Reforming the fragmented publicly funded school system in England Anne West* − London School of Economics and Political Science, UK David Wolfe − Matrix Chambers, UK Abstract This article focuses on the transformative academies policy in England. Based on an analysis of documentary evidence, we argue that the policy has resulted in the fragmentation of the state-funded school system and stark variation between academies, with those within multi-academy trusts (MATs) having no legal identity. We examine the variation between funding agreements, the control by central government, the role of MATs and the governance of academies. We propose policy options to improve the current incoherent and fragmented set of provisions, including restoring the legal identity of schools in MATs and allowing academies if they so wish, to convert to maintained schools. Keywords: academies; multi-academy trusts (MATs); funding agreements; law; governance; finance Introduction Since 2000 there has been a rapid and radical transformation of publicly funded school- based education in England: over a third of schools – and nearly three-quarters of secondary schools – are now ‘academies’ rather than ‘maintained’ by local authorities. Academies are owned and run by not-for-profit private trusts (exempt charities) that register as companies with Companies House and are subject to company law. They are controlled and funded directly by central government by means of a contract – a funding agreement – between a trust (that is, a legal entity) and the Secretary of State for Education (DfE, 2018a), rather than being run by a governing body in accordance with statutory education law, as is essentially the case for maintained schools.