Diagnostic Accuracy of Single Channel Cystometry for Neurogenic Bladder Diagnosis Following Spinal Cord Injury: a Pilot Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Suprapubic Puncture in the Treatment of Neurogenic Bladder
SUPRAPUBIC PUNCTURE IN THE TREATMENT OF NEUROGENIC BLADDER CHARLES C. HIGGINS, M.D. W. JAMES GARDNER, M.D. WM. A. NOSIK, M.D. The treatment of "cord bladder", a disturbance of bladder function from disease or trauma of the spinal cord, can be a difficult problem. Until the recent publications of Munro, there was little physiological basis for whatever treatment was instituted. With the advent of tidal drainage and recognition of the various types or stages of a given cord bladder, more satisfactory results have been obtained. In his excellent work on the cystometry of the bladder Munro1,2 classifies "cord bladders" into four groups: 1. Atonic — characterized by retention and extreme distention from lack of detrusor tone, lack of any activity of the external urethral sphincter, and complete lack of emptying contractions. 2. Autonomous — the detrusor and internal sphincter musculature show signs of reciprocal action of varying degree. There is an increase in detrusor muscle tone, and an inability to store an appreciable amount of urine without leakage. The condition of this bladder represents the end result in destructive lesions of the sacral segments or cauda equina. 3. Hypertonic — an expression of an uncontrolled spinal segmental reflex, characterized by a markedly increased detrusor muscle tone, almost constantly present emptying contractions, low residual urine, and impairment of control of the external sphincter. 4. Normal cord bladders — in transecting lesions above the sacral segments, consisting of two types which differ largely only in their cystometric findings: (a) Uninhibited cord bladder — an apparently normal bladder which empties itself quite regularly. The detrusor tone is still somewhat increased, emptying contractions are rhythmical, the residual is low, and the capacity is rather low. -

General Catalogue GENERAL CATALOGUE
Coloplast develops products and services that make life easier for people with very personal and private medical conditions. Working closely with the people who use our products, we create solutions that are sensitive to their special needs. We call this intimate healthcare. Our business includes ostomy care, urology and continence care, wound and skin care. & Gynaecology Urology We operate globally and employ more than 10 000 employees. General Catalogue GENERAL CATALOGUE Urology & Gynaecology The Coloplast logo and Porgès logo are registered trademarks of Coloplast A/S. © [2016- 05.] All rights reserved. Coloplast A/S, 3050 Humlebaek, Denmark. 2016 - 000NGLOBALCATEN01 INTRODUCTION Introduction With a world class innovative spirit and the ultimate objective of always being able to make your life easier, Coloplast presents its latest dedicated Urology Care catalogue including all of our disposables and implants for urology and gynaecology. For over 120 years, we have supported the medical progress through the development of the latest techniques and devices in co-operation with our leading surgeon partners. Our know-how and high quality industrial processes permit us to offer you medical materials of the very highest standards with worldwide recognition and expertise. Within this catalogue you will find all of the latest products you will need for your daily operating practice: • Endourology : A wide range of disposable products for stone management like Dormia stone extractors, Ureteral stents, Access sheath (Retrace) and guidewires. We have extended our line with a new innovative digital solution to remove ureteral stents in one step: ISIRIS α . The product is a combination between a single use flexible cystoscope with an integrated grasper and a reusable portable device • Female Pelvic Health: slings (Altis, Aris), and lightweight meshes (Restorelle), to treat stress urinary incontinence and pelvic organ prolapses. -

Urological Complications in Renal Transplantation
Henry Ford Hospital Medical Journal Manuscript 2015 Urological Complications in Renal Transplantation Riad N. Farah Richard Klugo Thomas Mertz Joseph C. Cerny Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal Part of the Life Sciences Commons, Medical Specialties Commons, and the Public Health Commons Henry Ford Hosp Med Journal Vol 26, No 3, 1978 Urological Complications in Renal Transplantation Riad N. Farah, MD,* Richard Klugo, MD,* Thomas Mertz, MD,* and Joseph C. Cerny, MD' There were 116 renal transplants performed on 108 patients RAFT survival after renal transplantation depends upon over a five-year period at Henry Ford Hospital with three the vascular and urinary anastomosis as well as control of major urological complications. The rate of 2.6% compares graft rejection. Numerous factors contribute to good results favorably with that reported in other series. Careful pre in transplantation, among which are immediate function of operative urological evaluation together with technically the homograft, high degree of histocompatibility, the avoid precise ureteroneocystostomy are factors that minimize the ance of excessive immunosuppression, and minimal wound incidence of urological complications. and urological complications. There have been several reportsof urological complications following renal transplantation (See Table). Complication rates as high as 25.7%' have been reported with ureteropyelostomy, while the rates for ureteroneocystos tomy range from 15%^ to less than 1%.' In our review of 116 renal transplants we found three urological complications (2.6%). This rate compares favorably wfth that reported in earlier series and underscores the importance ofthe urolo gist in the work-up and management of the transplant recipient. -

Cystometry (Basic Module)
Received: 6 September 2016 | Accepted: 19 September 2016 DOI 10.1002/nau.23181 REVIEW ARTICLE ICS teaching module: Cystometry (basic module) Carlos Arturo Levi D’Ancona1 | MarioJoãoGomes2 | Peter F.W.M. Rosier3 1 Division of Urology, University of Campinas School of Medicine, Campinas, Sao Paulo, Brazil Aims: To summarize the evidence background for education of good urodynamic 2 In remembrance: Hospital Santo Antonio, Porto, practice, especially cystometry. Portugal Methods: A search was done in PubMed for the last 5 years of publications selecting 3 Department of Urology, University Medical Center only clinical studies, utilizing the following keywords: cystometry 133 articles and Utrecht, The Netherlands filling cystometry 53 articles. Correspondence Results: The evidence with regard to clinical setting and cystometry technique, as Carlos Arturo Levi D’Ancona, Division of Urology, University of Campinas School of Medicine, well as for catheters and transducers type, infused solution and patient position is Campinas, Sao Paulo, Brazil. presented with recommendations. Also the practice of determining bladder filling Email: [email protected] sensation and capacity and the basis of detrusor storage function diagnosis is educated. Conclusions: This manuscript provides the evidence background for the practice of cystometry. KEYWORDS cystometry, urodynamics 1 | INTRODUCTION performing, and analyzing urodynamic testing. The teaching module consists of a presentation, in combination with this Cystometry is the method by which the storage function of the manuscript. This manuscript serves as a scientific background lower urinary tract (LUT) is measured during the filling of the review; the evidence base, for the ICS PowerPoint presenta- bladder.1,3 The aim of urodynamics is to find an objective, tion; available via http://www.icsoffice.org/eLearning/..... -

Sonographic Evaluation of Bladder Wall Thickness in Women with Lower
Original Article Obstet Gynecol Sci 2018;61(3):367-373 https://doi.org/10.5468/ogs.2018.61.3.367 pISSN 2287-8572 · eISSN 2287-8580 Sonographic evaluation of bladder wall thickness in women with lower urinary tract dysfunction Un Ju Shin1, Jihye Koh1, Jiwon Song1, Soyun Park2, Eun Joo Park3, Chung-Hoon Kim1, Sung Hoon Kim1, Byung Moon Kang1, Hee Dong Chae1 Department of Obstetrics and Gynecology, 1University of Ulsan College of Medicine, Asan Medical Center, Seoul; 2Jeju National University College of Medicine, Jeju National University Hospital, Jeju; 3Eulji University, Nowon Eulji Medical Center, Seoul, Korea Objective To investigate the correlation between bladder wall thickness (BWT) measured by ultrasonography and lower urinary tract dysfunction (LUTD) in patients with lower urinary tract symptoms (LUTS). Methods Forty-eight women with LUTS who underwent urodynamic study and BWT by ultrasonography as outpatients were studied. We assessed LUTS during a medical examination by interview. The thinnest part of the bladder wall was measured by a transabdominal ultrasonography. We excluded patients who had visited another hospital previously because we did not know what treatment they had received, including medications, behavioral therapy, or other treatments. We constructed receiver operating characteristic (ROC) curves for diagnosis of LUTD and also determined reliable BWT criteria by calculating the area under the curve. Statistical analyses were performed using the Kolmogorov-Smirnov method and Student's t-test. Results The mean age, body mass index, and duration of symptoms were 59.9±9.7 years, 26.06±3.4 kg/m2, and 53.4±38.2 months, respectively. Urodynamic study parameters (Valsalva leak point pressure, maximal urethral closure pressure, functional length, and postvoid residual volume) were lower in patients with BWT <3 mm; however, these differences were not significant. -

EAU Guidelines on Urological Infections 2018
EAU Guidelines on Urological Infections G. Bonkat (Co-chair), R. Pickard (Co-chair), R. Bartoletti, T. Cai, F. Bruyère, S.E. Geerlings, B. Köves, F. Wagenlehner Guidelines Associates: A. Pilatz, B. Pradere, R. Veeratterapillay © European Association of Urology 2018 TABLE OF CONTENTS PAGE 1. INTRODUCTION 6 1.1 Aim and objectives 6 1.2 Panel composition 6 1.3 Available publications 6 1.4 Publication history 6 2. METHODS 6 2.1 Introduction 6 2.2 Review 7 3. THE GUIDELINE 7 3.1 Classification 7 3.2 Antimicrobial stewardship 8 3.3 Asymptomatic bacteriuria in adults 9 3.3.1 Evidence question 9 3.3.2 Background 9 3.3.3 Epidemiology, aetiology and pathophysiology 9 3.3.4 Diagnostic evaluation 9 3.3.5 Evidence summary 9 3.3.6 Disease management 9 3.3.6.1 Patients without identified risk factors 9 3.3.6.2 Patients with ABU and recurrent UTI, otherwise healthy 9 3.3.6.3 Pregnant women 10 3.3.6.3.1 Is treatment of ABU beneficial in pregnant women? 10 3.3.6.3.2 Which treatment duration should be applied to treat ABU in pregnancy? 10 3.3.6.3.2.1 Single dose vs. short course treatment 10 3.3.6.4 Patients with identified risk-factors 10 3.3.6.4.1 Diabetes mellitus 10 3.3.6.4.2 ABU in post-menopausal women 11 3.3.6.4.3 Elderly institutionalised patients 11 3.3.6.4.4 Patients with renal transplants 11 3.3.6.4.5 Patients with dysfunctional and/or reconstructed lower urinary tracts 11 3.3.6.4.6 Patients with catheters in the urinary tract 11 3.3.6.4.7 Patients with ABU subjected to catheter placements/exchanges 11 3.3.6.4.8 Immuno-compromised and severely -

Early Management of Neuropathic Bladder in Spinal Cord
Paraplegia ('974), 1Z, 83-86 EARLY MANAGEMENT OF NEUROPATHIC BLADDER IN SPINAL CORD INJURIES 1 By J. DERMOT O'FLYNN, M.Ch., F.R.C.S.(Ed.), F.R.C.S.I. National Medical Rehabilitation Centre of Ireland, Dun Laoghaire; Urological Department, Meath Hospital, Dublin; Department of Surgery, Trinity College, Dublin FOLLOWING spinal cord injury the syndrome of spinal shock is reflected in the bladder by a state of atonicity. The smooth muscle of the bladder loses its normal tone and if cystometry is done at this stage no normal vesical contractions are discernible. This state is complicated by the fact that the external urethral sphincter (which is composed of striated muscle fibres, and which is usually closed) becomes paralysed, remains closed and cannot be relaxed. The bladder now has two peculiar disabilities-it cannot contract and empty itself, and its outlet is obstructed. Bladder tone and the ability to contract usually return in a period of days or a few weeks and vesical contractions can once again be detected on cystometry, but now the bladder may be subjected to very sudden and very violent rises of intravesical pressure, either due to uninhibited contractions of the vesical detrusor or participation in generalised aberrant reflux action. Despite the fact that the bladder does contract it does not necessarily empty satisfactorily as the external sphincter remains unrelaxed and the bladder cannot empty com pletely because its outlet is obstructed. The bladder's response to this situation is to hypertrophy, and the resulting raised intravesical pressure may enable it to overcome the external sphincter closure pressure-a small number of patients will establish apparently normal micturition. -

Training Guide Checklist
Training Guide Checklist Name: Date of Hire: Competence Requested GENERAL PROCEDURES demonstrated (date/ initial) Perform general patient assessment, including history and physical examination, and record or dictate the information appropriately in the patient medical record Order, perform, and interpret point-of-care tests, diagnostic laboratory tests and radiological studies Order medications and other therapies Consult with or refer to physician and non-physician health care professionals Give written or verbal orders per established collaborative practice agreement or per communication with the attending physician Admit and discharge patients in collaboration with the attending physician Direct provision of comprehensive, non-surgical management of common gynecologic conditions (e.g. age-appropriate periodic screening for gyn-related cancer, abnormal uterine bleeding, pelvic inflammatory disease, menstrual abnormalities, menopausal symptoms, sexual dysfunction, sexually transmitted infections, vulvovaginitis, vulvar dermatoses) SPECIAL PROCEDURES Competence Requested [e.g. Procedures that may not be part of prior training and\or are specific to demonstrated urogynecology or practice] (date/ initial) Advanced Urogynecologic Pelvic Examination (neurologic examination; POP-Q assessment; post-void residual; assessment of pelvic muscle strength, function, and pain; uroflow assessment; screening for urinary tract infection) Resources: Walters, M.D., Karram, M.M. (2015). Chapter 9, Evaluation of Urinary Incontinence and Pelvic Organ Prolapse: -

1 Evaluation of Renal Disease
Manual of Pediatric Nephrology Kishore Phadke • Paul Goodyer Martin Bitzan Editors Manual of Pediatric Nephrology Editors Kishore Phadke Martin Bitzan Department of Pediatric Nephrology Division of Pediatric Nephrology Children’s Kidney Care Center Montreal Children’s Hospital St. John’s Medical College Hospital McGill University Bangalore, KA Montreal , QC India Canada Paul Goodyer Division of Pediatric Nephrology Montreal Children’s Hospital McGill University Montreal, QC Canada ISBN 978-3-642-12482-2 ISBN 978-3-642-12483-9 (eBook) DOI 10.1007/978-3-642-12483-9 Springer Heidelberg New York Dordrecht London Library of Congress Control Number: 2013948392 © Springer-Verlag Berlin Heidelberg 2014 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, speci fi cally the rights of translation, reprinting, reuse of illustrations, recita- tion, broadcasting, reproduction on micro fi lms or in any other physical way, and transmission or infor- mation storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. Exempted from this legal reservation are brief excerpts in connection with reviews or scholarly analysis or material supplied speci fi cally for the purpose of being entered and executed on a computer system, for exclusive use by the purchaser of the work. Duplication of this publication or parts thereof is permitted only under the provisions of the Copyright Law of the Publisher’s location, in its current version, and permission for use must always be obtained from Springer. Permissions for use may be obtained through RightsLink at the Copyright Clearance Center. -
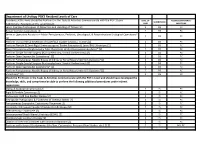
Department of Urology PGY2 Resident Levels of Care Residents at This Level Should Be Proficient in the Tasks & Activities Commensurate with the PGY-1 Level
Department of Urology PGY2 Resident Levels of Care Residents at this level should be Proficient in the Tasks & Activities Commensurate with the PGY-1 Level. LEVEL OF ACGME COMPETENCY/ SUPERVISION Additionally, Residents at this Level Should: CARE MILESTONE Learn Complex Techniques of Dissection and Handling of Tissues [2] 2 DS PC Repair Complex Lacerations [2] 2 DS PC Serve as Operative Assistant in Major Percutaneous, Pediatric, Oncological, & Reconstructive Urological Operations* 2 DS PC [2] Perform Transurethral Resection of Superficial Bladder Lesions / Tumors [2] 2 DS PC Perform Flexible & Semi-Rigid Ureteroscopy w/ Basket Extraction & Laser/EHL Lithotripsy [2] 2 DS PC Place Percutaneous Nephrostomy Tube Placement Under Fluoroscopic Guidance* [2] 2 DS PC Perform Simple Scrotal Surgery (Hydrocelectomy, Scrotal Orchiectomy) [2] 2 DS PC Perform Open Suprapubic Cystostomy* [2] 2 DS PC Perform Percutaneous Needle Biopsy of Kidney or Renal Mass Under U/S Guidance*[2] 2 DS PC Perform Simple Scrotal Surgery (Hydrocelectomy, Scrotal Orchiectomy) [2] 2 DS PC Perform Open Suprapubic Cystostomy* [2] 2 DS PC Perform Percutaneous Needle Biopsy of Kidney or Renal Mass Under U/S Guidance*[2] 2 DS PC Vasectomy* [2] 2 DS PC Should be Proficient in the Tasks & Activities Commensurate with the PGY-1 Level and should have developed the knowledge, skills, and competence be able to perform the following additional procedures under indirect supervision: Clamp & Surgical Circumcision [2] 2 IS PC Rigid & Flexible Cystoscopy [2] 2 IS PC Endoscopic Cold Cup -
Pathophysiology and Management of Urinary Tract Endometriosis
Nature Reviews|Urology, June 2017 Camran Nezhat, MD Endometriosis: presence of endometrial glands and stroma outside of the uterine cavity Predominantly affects the pelvic reproductive organs but also outside of the reproductive organs Most common sites of extragenital endometriosis are intestine and urinary tract. Theories: 1. Retrograde menstruation 90% of women have retrograde menstruation, only 10% develop endometriosis Further steps are necessary for endometrial cells to become endometriosis implants Affects distal>proximal ureter Affects left>right hemipelvis due to sigmoid colon 2. Altered immunity in the pathogenesis of endometrial implants Higher incidence of endometriosis in women with autoimmune disorders such as SLE, thyroid disease, RA, Sjogren’s syndrome, asthma, eczema Dysregulation of immune system might prevent normal clearance of ectopic endometrial cells, facilitating their implantation 3. Coelomic metaplasia Normal peritoneum transforms into endometriosis stimulated by hormonal or immunological factor Residual embryonic Mullerian rests stimulated by endogenous or exogenous estrogen exposure transforms into endometriosis 4. Benign metastasis Endometrial cells from within the uterus flow through lymphatic or hematological circulation and spread to distant parts of the body 5. Iatrogenic In port site and scar site ≤50% of bladder endometriosis found in women with prior cesarean 6. Genetic 7% risk of endometriosis in first-degree relatives Deeply infiltrating endometriosis (DIE) expresses invasive mechanisms -

Urodynamics Documentation Ruthie Youssefi, RN, MSN, CPNP Pediatric and Adolescent Urology, Inc Akron, Ohio Objectives
Urodynamics Documentation Ruthie Youssefi, RN, MSN, CPNP Pediatric and Adolescent Urology, Inc Akron, Ohio Objectives • Learn how and why to appropriately document urodynamics • Indications • Patient history • Procedure • Interpretation Differences from site to site • Not all of our sites may have the same exact way of documenting • Varied tools and formats • Paper documentation • Electronic documentation • Regardless of the method of documentation, there are certain key items that should be documented Components of a good urodynamic practice • A clear indication for and appropriate selection of, relevant test measurements and procedures • Precise measurement with data quality control and complete documentation • Accurate analysis and critical reporting of results Documentation prior to starting the study • A thorough history is extremely important to obtain prior to performing the study • History should include • Medications • Prior surgeries • Voiding/bowel diary OR cathing diary • Any significant medical history History- voiding/bowel diary • Voiding diary helps to define the functional bladder capacity • The child’s functional bladder capacity can be assessed as the largest voided volume, with the exception of the morning micturition, which actually represents night time bladder capacity • Frequency/volume chart is a detailed diary recording fluid intake and urine output over 24-hour periods • Gives objective information on the number of voidings, voided volumes and episodes of urgency and leakage, or dribbling • Defecation frequency,