Being Mortal: Medicine and What Matters in the End
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Being Mortal by Atul Gawande MD
Being Mortal by Atul Gawande MD Or The Book I Wish I’d Written! Reviewed by David R Grube MD I see it now – this world is swiftly passing. - the warrior Karna, in the Mahabharata Atul Gawande MD Education was born in 1965 in NY; parents both physicians; moved to Athens, Ohio as a youth obtained an undergraduate degree from Stanford (1987). Rhodes Scholar at Oxford (Philosophy, Politics, Economics, 1989). graduated with an MD, Harvard, 1995, MPH, 1999 completed General Surgery residency, Brigham and Women's Hospital, (2003) Political career was an early volunteer for Gary Hart’s presidential campaign (1984) involved with Al Gore’s campaign (1988) stopped medical school for two years to work on Bill Clinton’s campaign as Healthcare Lieutenant (1992) Political career in 1992, after Clinton’s inauguration, he became a Senior Adviser in the Department of Health and Human Services. He directed one of the three committees of the Clinton Health Care Task Force; the committee’s charge was to define the benefits packages for Americans and subsidies and requirements for employers. He returned to MS in 1993 Writings Slate Magazine (online) articles on residency New Yorker Magazine, staff writer 1998 June 2009 article compared health care in two towns in Texas; it “argued that a revenue-maximizing businessman-like culture (which can provide substantial amounts of unnecessary care) was an important factor in driving up costs, unlike a culture of low-cost high-quality care as provided by efficient health systems (ex: Mayo Clinic).” WIKIPEDIA Books 2002 - Complications: A Surgeon's Notes on an Imperfect Science 2007 - Better: A Surgeon's Notes on Performance 2009 - The Checklist Manifesto: How to Get Things Right 2014 - Being Mortal: Medicine and What Matters in the End Awards / Honors 2006 – MacArthur Fellow 2007 – Director of WHO’s effort to reduce surgical deaths 2009 – Hastings Center Fellow 2014 – Reith Lecturer (The Future of Medicine) (Boston/London/Edinburgh/Delhi) Rare photo of Atul Gawande as a little boy…. -

Mental Health Care in Mcallen Texas: Utilization, Expenditure, and Continuum of Care Josefina Irigoyen Antioch University - New England
Antioch University AURA - Antioch University Repository and Archive Student & Alumni Scholarship, including Dissertations & Theses Dissertations & Theses 2014 Mental Health Care in McAllen Texas: Utilization, Expenditure, and Continuum of Care Josefina Irigoyen Antioch University - New England Follow this and additional works at: http://aura.antioch.edu/etds Part of the Clinical Psychology Commons Recommended Citation Irigoyen, Josefina, "Mental Health Care in McAllen Texas: Utilization, Expenditure, and Continuum of Care" (2014). Dissertations & Theses. 129. http://aura.antioch.edu/etds/129 This Dissertation is brought to you for free and open access by the Student & Alumni Scholarship, including Dissertations & Theses at AURA - Antioch University Repository and Archive. It has been accepted for inclusion in Dissertations & Theses by an authorized administrator of AURA - Antioch University Repository and Archive. For more information, please contact [email protected], [email protected]. Running head: MENTAL HEALTH CARE IN MCALLEN Mental Health Care in McAllen Texas: Utilization, Expenditure, and Continuum of Care by Josefina Irigoyen B.A., The University of Texas at San Antonio, 2002 M.Ed., The University of Texas Pan-American, 2004 M.S., Antioch University New England, 2007 DISSERTATION Submitted in partial fulfillment for the degree of Doctor of Psychology in the Department of Clinical Psychology at Antioch University New England, 2014 Keene, New Hampshire MENTAL HEALTH CARE IN MCALLEN ii Department of Clinical Psychology DISSERTATION COMMITTEE PAGE The undersigned have examined the dissertation entitled: MENTAL HEALTH CARE IN MCALLEN TEXAS: UTILIZATION, EXPENDITURE, AND CONTINUUM OF CARE presented on March 17, 2014 by Josefina Irigoyen Candidate for the degree of Doctor of Psychology and hereby certify that it is accepted*. -

The Leg.Up Local, State and National News of Interest to the Physician Community
The Leg.Up Local, state and national news of interest to the physician community January 25, 2017 Dr. Atul Gawande on "The Heroism of Incremental Care" Click here to read "The Heroism of Incremental Care," the latest New Yorker essay by Dr. Atul Gawande - a past speaker at RAM. Gawande describes the case of a patient who has "spent almost four decades under attack from the inside of his skull" from "severe migraines that felt as if a drill were working behind his eyes, across his forehead, and down the back of his head and neck." "He saw all kinds of doctors - primary-care physicians, neurologists, psychiatrists - who told him what he already knew: he had chronic migraine headaches. And what little the doctors had to offer didn't do him much good." Gawande describes the many symptoms of migraines -- whose cause he says "remains unknown" -- and the multiple treatments the patient tried. At the John Graham Headache Center in Boston, Gawande explores a process where "success meant that the headaches became less frequent and less intense," and "that the patients grew more confident in handling them." Bottom line: "Success would be incremental." Click here to read Gawande's essay on the power of "incremental care," which often clashes with our "heroic expectations of how medicine works." Atul Gawande is a surgeon at Brigham and Women's Hospital in Boston, a professor at Harvard T.H. Chan School of Public Health and the director of Ariandne Labs. His latest book is "Being There." Trump's ACA Order Rattles System President Trump's executive order instructing federal agencies to grant relief to constituencies affected by Obamacare "has begun to reverberate throughout the nation's healthcare system, injecting further uncertainty into an already unsettled insurance landscape," reports The Washington Post. -

Pay-For-Performance Reimbursement in Health Care
University of Richmond UR Scholarship Repository Political Science Faculty Publications Political Science 3-22-2011 Pay-for-Performance Reimbursement in Health Care: Chasing Cost Control and Increased Quality through "New and Improved" Payment Incentives Rick Mayes University of Richmond, [email protected] Jessica Walradt Follow this and additional works at: http://scholarship.richmond.edu/polisci-faculty-publications Part of the Health Policy Commons, Social Policy Commons, and the Social Welfare Commons Recommended Citation Mayes, Rick, and Jessica Walradt. "Pay-for-Performance Reimbursement in Health Care: Chasing Cost Control and Increased Quality through "New and Improved" Payment Incentives." Health Law Review 19, no. 2 (March 22, 2011): 39-43. This Article is brought to you for free and open access by the Political Science at UR Scholarship Repository. It has been accepted for inclusion in Political Science Faculty Publications by an authorized administrator of UR Scholarship Repository. For more information, please contact [email protected]. Pay-for-Performance Reimbursement in Health Care: Chasing Cost Control and Increased Quality through “New and Improved” Payment Incentives Rick Mayes and Jessica Walradt Abstract associated with fee-for-service reimbursement, which Pay-for-performance (P4P) reimbursement has become is the dominant model in the U.S.1 Instead of simply a popular and growing form of health care payment reimbursing providers more for greater volume and built on the belief that payment incentives strongly intensity of care, P4P pays more to providers whose care affect medical providers’ behavior. By paying more to is deemed to be of higher (or suffi ciently high) quality.2 those providers who are deemed to deliver better care, These plans are intended to lower health care costs over the goal is to increase quality and, hopefully, restrain the long term by increasing preventative care, primary cost growth. -
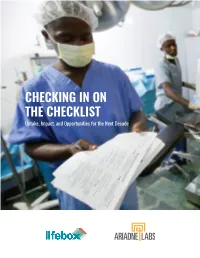
CHECKING in on the CHECKLIST Uptake, Impact, and Opportunities for the Next Decade COVER PHOTO: AHMED JALLANZO PREFACE 1
CHECKING IN ON THE CHECKLIST Uptake, Impact, and Opportunities for the Next Decade COVER PHOTO: AHMED JALLANZO PREFACE 1 ACKNOWLEDGMENTS 2 EXECUTIVE SUMMARY 4 CHAPTER 1: A SIMPLE, EVIDENCE-BASED TOOL 6 TESTING THE CHECKLIST . 12 CHAPTER 2: THE ENTREPRENEURIAL PHASE 14 LESSONS LEARNED FROM EARLY ADOPTERS . 17. CHAPTER 3: THE CHECKLIST FOOTPRINT AT TEN YEARS 20 UNFINISHED BUSINESS: IMPLEMENTATION IN LMICS . 22 CHAPTER 4: IMPACT OF THE CHECKLIST 24 BEYOND MORTALITY AND MORBIDITY . .26 . CHAPTER 5: OPPORTUNITIES IN THE SECOND DECADE 28 CONTEXT AS AN INESCAPABLE DETERMINANT . 30 STRATEGIES TO GET TO SCALE AND SUSTAINED USE . 32. TOOLS FOR CHECKLIST IMPLEMENTATION AND USE . 34 . CONCLUSION: GETTING TO SCALE, SUSTAINING SAFER SURGICAL PRACTICES 36 ENDNOTES 38 PREFACE The very fact that surgery exists—that we to see how rapidly and enthusiastically it has can safely open people’s bodies, remove and been adopted. A pooled analysis of international rearrange the parts, close the bodies back up studies found that the Checklist is being used again, and turn out to have made people in 75% of operations globally. Multiple, large- better—is an astonishment. scale evaluations have confirmed substantial reductions in surgical complications and deaths Nonetheless, over the last century, the art that when implemented effectively. How? Leaders became a science has become a mass enterprise point to the way that use of the Checklist breaks delivering more than 300 million operations down operating room hierarchies, improves a year worldwide. Surgery has become an communication and compliance with best essential part of enabling human beings to live safety practices, and ultimately helps surgical long and healthy lives. -

Atul Gawande
Atul Gawande n the book-jacket photograph of than people expect them to be, but also Complications: A Surgeon’s Notes on more extraordinary than they under- Ian Imperfect Science, Atul Gawande stand, is the balance I’ve tried to show”. looks 20-ish (he is actually 37). In per- These big ideas, which could so easily son, he appears to be about 13. The lend themselves to high-handed and Wunderkind seated before me is a utterly impenetrable academic analysis, surgery resident, a Rhodes scholar, a are instead embedded in scenes that are, staff writer for The New Yorker, the as his editor says, filled with the “small author of this new book, a father of memorable details of real life”. Once three, and, oh yeah, was a health-policy you’ve read a Gawande essay, for exam- advisor to former US President Bill ple, nausea is not just the miserable result Clinton. That last bit is ancient history, ubiquitous in Gawande’s writing. He is, of “unanticipated sensory input”. of course, having taken place when he according to Henry Finder, his editor at Instead, it becomes the indelible and was all of 26. the New Yorker, “peculiarly drawn to seemingly endless central problem of the Gawande, a graduate of Stanford paradoxes, tragic choices”. (Gawande story of Amy Fitzpatrick. Her hypereme- University and Harvard Medical School, writes four essays a year for the maga- sis, which began in the eighth week of her worked for the Clinton campaign and zine, with each piece taking him 3–4 pregnancy with twins, is treated with then moved on to the White House to -

The Texas Physician's Accountable Care Guide
The Texas Physician’s Accountable Care Guide Volume I By Julian D. (“Bo”) Bobbitt Jr., JD The Texas Physician’s Accountable Care Guide Volume I Julian D. (“Bo”) Bobbitt Jr., JD No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the publisher. The Texas Physician’s Accountable Care Guide Volume I Author: Julian D. (“Bo”) Bobbitt Jr., JD Editor: Ellen Terry, Communications Manager TMA Client Services NOTICE: The Texas Medical Association provides this information with the express understanding that (1) no attorney- client relationship exists, (2) neither TMA nor its attorneys are engaged in providing legal advice, and (3) the information is of a general character. This is not a substitute for the advice of an attorney. While every effort is made to ensure that content is complete, accurate, and timely, TMA cannot guarantee the accuracy and totality of the information contained in this publication and assumes no legal responsibility for loss or damages resulting from the use of this content. You should not rely on this information when dealing with personal legal matters; rather legal advice from retained legal counsel should be sought. The information contained in this publication is Texas-specific and may or may not apply in your state. This information is provided as a commentary on legal issues and is not intended to provide advice on any specific legal matter. Certain links provided with this information connect to websites maintained by third parties. -
Understanding Health Insurance
Understanding Health Insurance A Guide for Brokers, Administrators, Students and Healthcare Practitioners 1 2 Understanding Health Insurance A Guide for Brokers, Administrators, Students and Healthcare Practitioners Copyright © 2010 by Gary Fradin All rights reserved. This book may not be duplicated in any way, either in books, digital form, or any other medium, without the expressed written consent of Gary Fradin, except in the form of brief excerpts or quotations for the purposes of review ISBN: 978-0-557-42092-6 3 4 The Author Gary Fradin teaches healthcare economics to insurance brokers and healthcare professionals nationally. He is President of HealthInsuranceCE LLC, which provides health insurance continuing education courses to licensed insurance brokers nationally. He has authored 2 previous books, Healthcare Problems and Solutions in 2008 and Moral Hazard in American Healthcare in 2007. He also has had numerous articles published in industry journals. Gary holds Masters degrees from both Harvard and London Universities, and a Bachelors degree from Lancaster University in England. He is a licensed health insurance broker and lives in Massachusetts. 5 6 Preface This book grew out of discussions I had with many health insurance brokers between 2007 and 2009. I had been lecturing regularly to groups of experienced brokers. They typically understood their businesses well – underwriting, policy provisions and regulations. Their questions and comments typically reflected a high degree of policy knowledge and professionalism. But I was struck by their lack of understanding about the context within which they worked. Though they knew a great deal about specific policies, they frequently knew very little about policy implications or the overall working of our health insurance system. -
Atul Gawande, Md, Mph
Joint Plenary: Population Health Colloquium & Medical Home Summit Marci Nielsen, PhD, MPH CEO, PCPCC March 23, 2015 National Imperative: “Triple Aim” Source : Berwick, Donald M., Thomas W. Nolan, and John Whittington. "The triple aim: care, health, and cost." Health Affairs 27.3 (2008): 759-769. PCPCC 2014. All Rights Reserved. ATUL GAWANDE, MD, MPH Harvard Professor, Surgeon, Writer, Public Health Researcher 3 AtulAtul Gawande,Gawande, MD,MD, MPHMPH • Born: 1965, Brooklyn, NY • Education: Balliol College (1989), Stanford University (1987), Harvard (MD, MPH) • Additional facts: MacArthur Fellowship; nomination for National Book Award for Nonfiction, New Yorker author 4 ATUL GAWANDE, MD, MPH Harvard Professor, Surgeon, Writer, Public Health Researcher Chief Executive Officer, PCPCC 5 Coincidence?!Coincidence?! Atul Gawande, MD, MPH Marci Nielsen, PhD, MPH • Born: 19651965 • Born: 19651965 • Education: BBalliol • Education: BBriar CCliff CCollege (1989), Stanford (1987), George University (1987), Washington University Harvard (MD, MPH) (1994), Johns Hopkins • Wrote a speech called (PhD) “Cowboys and Pit • Live in a state with realreal crews” livelive cowboyscowboys andand pitpit crewscrews 6 So what’s “our story”? Study Authors: •Marci Nielsen, PhD, MPH •Amy Gibson, RN, MS •Lisabeth Buelt •Paul Grundy, MD, MPH •Kevin Grumbach, MD PCPCC 2014. All Rights Reserved. PCMH PeerPeer‐‐ReviewedReviewed Outcomes • Medicare FFS (NCQA PCMH) • Veterans Affairs (PACT) • (4 studies) • Florida Medicaid • Illinois Medicaid • Kentucky –Ft. Campbell • New -

Five Questions for Atul Gawande, M.D
Five Questions for Atul Gawande, M.D. An interview by David Cameron, Director of Media Relations, Office of Communications and External Relations, Harvard Medical School Atul Gawande, M.D., MPH, is a surgeon at Brigham and Women’s Hospital; Associate Professor of Surgery, Harvard Medical School; and Associate Professor in Health Policy and Courtesy of Picker Institute Management, Harvard School of Public Health—all in Boston, Mass. He received his B.A.S. from Stanford University, an M.A. in politics, philosophy and economics from Oxford University, his M.D. from Harvard Medical School, and an MPH from the Harvard School of Public Health. He is director of the Global Challenge for Safer Surgical Care of the World Health Organization. A staff writer for The New Yorker magazine since 1998, he recently published “The Checklist Manifesto: How to Get Things Right” (Picador, 2011). David Cameron: Your latest book, “The Checklist Manifesto,” examines the role of the checklist in the operating room. Can a humble checklist really save lives? Atul Gawande: Though it seems almost ridiculous in its simplicity, we’ve found that a checklist can save lives. And two recent studies—in the Veterans Administration system and in the Netherlands—have confirmed the substantial mortality reductions we observed when teams are trained in the principles the checklist embodies. What’s intriguing are those principles. Checklists are memory aids. But, designed well, they also foster teamwork. Doctors don’t love to use them at first. I know I didn’t, and I was running the World Health Organization’s program that was testing them. -

The Importance of Narrative in Medicine
The importance of narrative in medicine Catherine Spaulding, MD Dr. Spaulding is a Resident-Physician in Internal Medicine The list comes from the speech “Suggestions on and Pediatrics at Georgetown University Hospital in Becoming a Positive Deviant,” by physician and writer Washington, DC. Atul Gawande.1 At the time I read this speech I had barely or the past six years, a Post-it® note has been left the seat of my first-year medical school classroom, yet Gawande’s words struck a chord. I felt compelled to write taped to the corner of my bedroom mirror. The them down and put them in a place I would see everyday— writing has faded over time, but the importance on my bedroom mirror. of these words has not: Most of Dr. Gawande’s suggestions I understood without further explanation. A simple question—Where did you 1. Ask an unscripted question grow up?—fosters an emotional connection with patients. 2. Don’t complain Those personal details are reminders of our patients’ hu- 3. Count something manity, which may be a key motivator regarding Gawande’s 4. Write something admonition not to complain. 5. Change The act of counting something may sound arbitrary, but it represents the most basic form of research, which The importance of narrative in medicine A 28-year-old ultimately impacts patient outcomes. The female with ability to change in response to evolving metastatic clinical situations is a critical skill for any- one in health care. melanoma However, his fourth suggestion, to “write s/p bilateral something,” gave me pause. -

Resources for Reflection on Health Disparities and Medical Humanities
Resources for Reflection on Health Disparities and Medical Humanities Books Many of these books are written by medical doctors either reflecting on their experience as residents, on becoming doctors, with patients and families, making mistakes, and so on. One book is a memoir written by a lawyer and has nothing to do with medicine, and everything to do with being human. Two items include pieces written by patients or their family members on the human aspects of clinical experiences. You might disagree with some, none or all of what is said in these writings, or the politics of the writers themselves, but they offer multiple perspectives on a view into the heart of being human, remembering what it means to be a patient, and the import of these for being a physician. Gawande, Atul. Being Mortal: Medicine and What Matters in the End. , 2014. Print.i Medicine has triumphed in modern times, transforming birth, injury, and infectious disease from harrowing to manageable. But in the inevitable condition of aging and death, the goals of medicine seem too frequently to run counter to the interest of the human spirit. Nursing homes, preoccupied with safety, pin patients into railed beds and wheelchairs. Hospitals isolate the dying, checking for vital signs long after the goals of cure have become moot. Doctors, committed to extending life, continue to carry out devastating procedures that in the end extend suffering. Gawande, a practicing surgeon, addresses his profession's ultimate limitation, arguing that quality of life is the desired goal for patients and families. Gawande offers examples of freer, more socially fulfilling models for assisting the infirm and dependent elderly, and he explores the varieties of hospice care to demonstrate that a person's last weeks or months may be rich and dignified (Publisher’s abstract).