Supplemental Data
{2 Column Table}
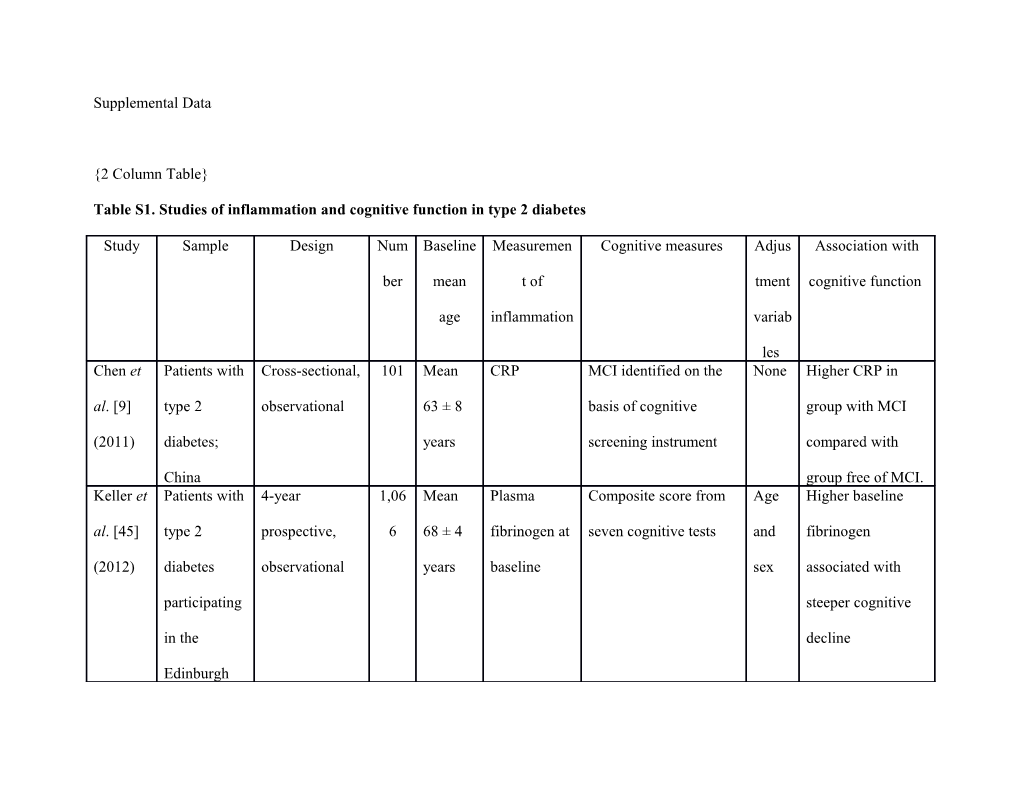
Table S1. Studies of inflammation and cognitive function in type 2 diabetes
Study Sample Design Num Baseline Measuremen Cognitive measures Adjus Association with
ber mean t of tment cognitive function
age inflammation variab
les Chen et Patients with Cross-sectional, 101 Mean CRP MCI identified on the None Higher CRP in al. [9] type 2 observational 63 ± 8 basis of cognitive group with MCI
(2011) diabetes; years screening instrument compared with
China group free of MCI. Keller et Patients with 4-year 1,06 Mean Plasma Composite score from Age Higher baseline al. [45] type 2 prospective, 6 68 ± 4 fibrinogen at seven cognitive tests and fibrinogen
(2012) diabetes observational years baseline sex associated with
participating steeper cognitive
in the decline
Edinburgh Type 2
Diabetes
Study;
Scotland Keller et Patients with 4-year 1,06 Mean Plasma IL-6 Composite score from Age Higher baseline IL- al. [46] type 2 prospective, 6 68 ± 4 at baseline seven cognitive tests and 6 associated with
(2012) diabetes observational years sex steeper cognitive
participating decline.
in the
Edinburgh
Type 2
Diabetes
Study;
Scotland Marioni Patients with Cross-sectional, 1,06 Mean Plasma Composite score from Age Higher fibrinogen et al. type 2 observational 6 68 ± 4 fibrinogen seven cognitive tests and associated with
[43] diabetes years sex lower cognitive
(2011) participating function. in the
Edinburgh
Type 2
Diabetes
Study;
Scotland Marioni Patients with Cross-sectional, 1,06 Mean Plasma IL-6, Composite score from Age, Higher IL-6 et al. type 2 observational 6 68 ± 4 TNF-α, and seven cognitive tests sex, associated with
[44] diabetes years CRP and estimate of pre- educa lower cognitive
(2010) participating morbid ability tion, function and
in the cardio steeper estimated
Edinburgh vascu lifetime decline
Type 2 lar (fully adjusted
Diabetes diseas analyses).
Study; e, Association of
Scotland durati higher TNF-α with
on of lower cognitive diabet function and
es, estimated lifetime
HbA1 decline only in
c, and analyses adjusted
estim for age, sex, and
ated estimated pre-
pre- morbid ability. No
morbi consistent finding
d for CRP.
abilit
y Umegak Patients with 6-year 79 Mean Mean of Composite score from None No association. i et al. type 2 prospective, 74 ± 5 CRP MMSE, Digit Symbol
[16] diabetes; observational years measured at Coding, Stroop, and
(2014) Japan baseline and word recall. Analyses of
annual ‘decliners’ versus ‘non-
follow-ups decliners’ on bases of composite score and
individual cognitive
tests. CRP, C-reactive protein; IL-6, interleukin-6; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; TNF-α, tumor necrosis factor-alpha. {2 Column Table}
Table S2. Studies of microvascular disease and cognitive function in type 2 diabetes
Study Sample Design Numbe Baseline Measuremen Cognitive Adjustment Association
r mean age t of measures variables with
microvascul cognitive
ar disease function de Bresser et Patients with 4-year 122 Mean 66 ± 6 Ophthalmol Composite Age, sex, No al. [49] type 2 diabetes prospective, years ogist- score from and pre- association.
(2010) participating in observationa identified 11 cognitive morbid
the Utrecht l presence tests, ability for
Diabetic versus estimate of analyses of
Encephalopath absence of pre-morbid cognitive
y Study; retinopathy ability, total function.
The according to brain Age and sex
Netherlands ‘standard volume, for analyses
clinical lateral of imaging
practice’ at ventricular data. baseline volume,
white matter
hyperintensi
ty volumes,
and cerebral
infarcts de Galan Patients with 5-year trial 11,140 Mean 66 ± 6 ‘Major At baseline None Cross- et al. [35] type 2 diabetes on effects of years diabetic eye and 2-year sectional
(2009) participating in intensified disease’ intervals: analysis:
ADVANCE blood MMSE increased
arm on pressure followed by prevalence
glycemic control and clinical of major
control, intensified interview diabetic eye
receiving glycemic for patients disease in
standard target control with MMSE groups with
versus target <24 or cognitive
HbA1c ≤6.5%; suspected dysfunction. Australia dementia.
‘Normal’
cognitive
function
defined as
MMSE ≥28;
‘mild
dysfunction’
as MMSE =
24-27;
‘severe
dysfunction’
as MMSE
<24.
Additional
use of
MMSE as continuous
measure. Hugenschmid Patients with 40-month 1,862 Mean 62 ± 6 Presence of Digit Age, sex, Cross- t et al. [50] type 2 diabetes prospective, years no Symbol ethnicity, sectional
(2014) participating in observationa retinopathy, Coding education, association
ACCORD-Eye l of mild non- (primary smoking, of
and ACCORD- proliferative outcome), geographic retinopathy
MIND retinopathy, MMSE, Rey region, with lower
substudies of or of Auditory duration of gray matter
ACCORD; moderate/se Verbal diabetes, volume but
North America vere Learning, HbA1c, not with
retinopathy and Stroop cholesterol, cognitive
at baseline; (secondary triglycerides function.
based on outcomes) , blood Prospective
ETDRS at baseline pressure, association
chart and 20 and anti- of
40 months. hypertensive retinopathy Total brain medication with steeper volume, use, 40-month white matter depression, (but not 20- volume, alcohol, and month) gray matter neuropathy. decline on volume, and Additional MMSE and abnormal adjustment Digit white matter for visual Symbol volume at acuity for Coding. baseline and analyses of Statistically
40 months. cognitive non-
function and significant
for total trend for
intracranial association
volume for of baseline
analyses of retinopathy
brain with greater volumes. increase in
white matter
abnormalitie
s during 40-
month
follow-up. Manschot et Patients with Cross- 122 Mean 66 ± 6 Presence Composite Age, sex, No al. [25] type 2 diabetes sectional, years versus score from and association
(2007) participating in observationa absence of 11 cognitive estimated of
the Utrecht l retinopathy tests, pre-morbid retinopathy
Diabetic based on estimate of ability with
Encephalopath scores on pre-morbid estimated
y Study; diabetic ability, lifetime
The retinopathy cortical decline in
Netherlands severity atrophy, and cognitive
scale white matter function.
(Wisconsin lesions Association Epidemiolog of
ic Study of retinopathy
Diabetic with
Retinopathy presence of
) at baseline cortical
atrophy
(analysis
additionally
controlling
for lipid-
lowering
drugs and
cerebral
infarcts). ACCORD, Action to Control Cardiovascular Risk in Diabetes; ACCORD-MIND, Action to Control Cardiovascular Risk in Diabetes-
Memory in Diabetes; ADVANCE, Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled
Evaluation; ETDRS, Early Treatment of Diabetic Retinopathy Study; MMSE, Mini-Mental State Examination.
{2 Column Table}
Table S3. Studies of markers of macrovascular disease and cognitive function in type 2 diabetes
Study Sample Design Numbe Baselin Macrovascular Cognitive Adjustme Association
r e mean disease measures nt with cognitive
age variables function Bruce et Patients with 8-year 302 Mean ‘Cerebrovascular Dementia and None Cross- al. [14] type 2 retrospectiv 76 ± 5 disease’ (stroke MCI identified sectional
(2008) diabetes e, years and TIA), ‘CHD’ from screening analyses:
participating observation (MI, angina, instruments/clinic increased
in the al coronary artery al interview prevalence of
Fremantle bypass, and cerebrovascul
Diabetes evidence of MI on ar disease
Study; ECG), and across
Australia peripheral arterial cognitive
disease at baseline groups, with
and 8 years earlier highest
prevalence in dementia group, followed by
MCI group and unimpaired group.
Increased prevalence of
PAD in group with any cognitive impairment
(in model controlling for sex, duration of diabetes, and stroke) and in group with dementia
(in model controlling for age, sex, and duration of diabetes).
Prospective analyses: cerebrovascul ar disease
(unadjusted analysis) and
PAD (model controlling for age, sex, duration of
diabetes, and
waist-hip
ratio) 8 years
earlier both
associated
with poorer
cognitive
outcome. No
findings for
CHD. Bruce et Patients with 8-year 205 Mean Cerebrovascular Dementia and None No al. [21] type 2 retrospectiv 75 ± 4 disease and MCI identified association.
(2008) diabetes e, 2-year years peripheral arterial from screening
participating prospective, disease assessed 8 instruments/clinic
in the observation years prior to al interview at
Fremantle al baseline cognitive baseline and at 2- Diabetes assessment year follow-up.
Study; ‘Cognitive
Australia decline’ defined
as downward
conversion
between
‘normal’, MCI,
and dementia. Chen et al. Patients with Cross- 101 Mean ABI and cIMT MCI identified on None Lower ABI
[9] (2011) type 2 sectional, 63 ± 8 the basis of and higher
diabetes; observation years screening cIMT in
China al instrument group with
MCI
compared
with group
free of MCI. Chen et al. Patients with Cross- 157 Mean cIMT MCI identified on None Higher cIMT
[11] type 2 sectional, 55 ± 7 the basis of in group with (2012) diabetes; observation years cognitive MCI
China al screening compared
instrument with group
free of MCI.
Inverse
correlation
between
cognitive
scores and
cIMT. Cukierma Patients with Cross- 2,977 Mean Stroke, ‘CVD’ Digit Symbol Age Association of n-Yaffe type 2 sectional 63 ± 6 (stroke, MI, angina Coding (primary stroke with et al. [13] diabetes analysis of years with ischemic outcome), lower
(2009) participating trial on changes, and MMSE, Rey cognitive
in ACCORD- blood coronary Auditory Verbal function.
MIND; pressure, procedure) Learning, and Association of
North lipids, and Stroop CVD (without America glycemic (secondary stroke) with
control outcomes) lower verbal
memory but
higher MMSE
scores. de Galan Patients with 5-year 11,140 Mean Stroke, MI, major At baseline and Age, sex, Cross- et al. [35] type 2 prospective 66 ± 6 coronary event 2-year intervals: education, sectional,
(2009) diabetes trial on years (non-fatal MI, MMSE followed and unadjusted
participating effects of death from by clinical treatment analyses:
in ADVANCE intensified coronary event), interview for allocation association of
arm on blood and major CVD patients with stroke and
glycemic pressure event (MI, stroke, MMSE <24 or major CVD
control; control and and cardiovascular suspected event with
Australia intensified death) during dementia. lower
glycemic follow-up ‘Normal’ cognitive
control cognitive function. No
function defined finding for as MMSE ≥28; MI.
‘mild Prospective dysfunction’ as analyses
MMSE = 24-27; (adjusted):
‘severe baseline mild dysfunction’ as and severe
MMSE <24. impairment
Additional use of (versus
MMSE as unimpaired) continuous associated measure. with increased
risk of major
CVD event,
stroke, and
major
coronary
event during follow-up.
Lower MMSE
at baseline
associated
with increased
risk of major
CVD event. Feinkohl Patients with 4-year 1,066 Mean MI, stroke, angina, MMSE, Age, sex, Cross- et al. [51] type 2 prospective, 68 ± 4 ABI, and cIMT at composite score cholestero sectional
(2013) diabetes observation years baseline from seven l, blood analyses:
participating al cognitive tests, pressure, stroke,
in the and estimate of smoking, angina, and
Edinburgh pre-morbid and MI associated
Type 2 ability estimated with lower
Diabetes pre- cognitive
Study; morbid function.
Scotland ability Prospective analyses:
stroke, higher
cIMT, and
lower ABI
associated
with increased
late-life
cognitive
decline and
increased
estimated
lifetime
decline. Manschot Patients with Cross- 122 Mean ‘Any Composite scores Age, sex, Association of et al. [20] type 2 sectional, 66 ± 6 macrovascular on five cognitive and infarcts with
(2006) diabetes observation years event’ defined as domains from 11 estimated steeper
participating al MI, stroke, or cognitive tests, pre- estimated in the Utrecht surgery/endovascul estimate of pre- morbid lifetime
Diabetic ar treatment for morbid ability, ability decline in
Encephalopat coronary, carotid cortical atrophy, processing
hy Study; or peripheral and white matter speed.
The arterial disease. lesions Association of
Netherlands Cerebral infarcts any
on MRI. macrovascular
event with
steeper
estimated
lifetime
decline in
processing
speed and
memory. Manschot Patients with Cross- 122 Mean ‘Any Composite score Age, sex, ‘Any et al. [25] type 2 sectional, 66 ± 6 macrovascular from 11 cognitive and macrovascular (2007) diabetes observation years event’ (MI, stroke, tests, estimate of estimated event’ and
participating al and pre-morbid pre- infarcts both
in the Utrecht surgery/endovascul ability, cortical morbid associated
Diabetic ar treatment for atrophy, and ability with steeper
Encephalopat coronary, carotid, white matter estimated
hy Study; or peripheral lesions lifetime
The arterial disease) cognitive
Netherlands and cerebral decline.
infarcts on MRI. Finding on
Measurement of ‘any vascular
cIMT. event’
attenuated
following
exclusion of
patients with
stroke. For
‘any vascular event’, but not
infarcts,
association
persisted in
final model
adjusting for
age, estimated
pre-morbid
ability,
hypertension,
smoking, and
lipid-lowering
drugs. No
finding for
cIMT. ABI, ankle brachial index; ACCORD-MIND, Action to Control Cardiovascular Risk in Diabetes-Memory in Diabetes; ADVANCE,
Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation; CHD, coronary heart disease; cIMT, carotid intima-media thickness; CVD, cardiovascular disease; ECG, electrocardiogram; MCI, mild cognitive impairment; MI, myocardial infarction; MMSE, Mini-Mental State Examination; MRI, magnetic resonance imaging; PAD, peripheral arterial disease; TIA, transient ischemic attack. {2 Column Table}
Table S4. Studies of natriuretic peptides and cognitive function in the general population and in type 2 diabetes
Study Sample Design Number Baseli Natriuretic Cognitiv Adjustment Association
ne peptide e variables with
mean measures cognitive
age function Daniels et Rancho Cross-sectional, 950 Mean NT-proBNP, MMSE, Age, sex, ‘High’ NT- al. [52] Bernardo observational 77 ± 8 categorized as Trail- education, proBNP
(2011) Study; USA years ‘high’ (≥450 Making hypertension, group likely
pg/mL) versus Test, and body mass to score low
‘low’ (<450 Category index, exercise, on MMSE
pg/mL) and Fluency. alcohol, and Trail-
additionally as ‘Low’ smoking, Making
quartiles of the performa cholesterol, and compared
distribution nce on creatinine with ‘low’
each group.
defined Findings as similar when
MMSE excluding
≤24, participants
Trail- with stroke
Making and
≥300 cardiovascul seconds, ar disease. and Findings for
Category Category
Fluency Fluency
≤12 restricted to words. largely
Cognitiv unadjusted e tests analyses. additiona Additionally lly used increased as prevalence quartiles of scoring in
of lower
respectiv quartiles of
e cognitive
distributi scores with
on. increasing
quartiles of
NT-proBNP
(unadjusted
analyses). Feinkohl et Patients with 4-year 1,066 Mean NT-proBNP at MMSE, Age, sex, Association al. [51] type 2 prospective, 68 ± 4 baseline composit cholesterol, of higher
(2013) diabetes observational years e score blood pressure, baseline NT-
participating from and smoking proBNP
in the seven with steeper
Edinburgh cognitive late-life
Type 2 tests, and cognitive Diabetes estimate decline and
Study; of pre- steeper
Scotland morbid estimated
ability lifetime
decline.
Finding on
4-year
decline lost
statistical
significance
when
controlled
for
estimated
pre-morbid
ability or for
stroke, cIMT, and
ABI. Kerola et Kuopio 75+ 5-year 464 Mean BNP at baseline Diagnosi Age, education, Association al. cohort; prospective, 80 ± 4 s of AD, and of higher
[53] (2010) Finland observational years VaD, and hypertension BNP with
MMSE lower
MMSE and
with steeper
decline on
MMSE
(unadjusted
analyses).
Association
of higher
BNP and
increased
risk of AD and VaD
diagnosis
during
follow-up
(adjusted
analyses). Hiltunen et Kuopio 75+ 5-year 601 Range BNP at baseline Diagnosi Cross-sectional Presence of al. cohort; prospective, 75-96 s of analyses: age, any
[54] (2013) Finland observational years dementia sex, dementia
medication, associated
heart failure, with higher
and blood BNP in
pressure. youngest
Prospective tertile and
analyses: age, lower BNP
education, and in oldest
hypertension. tertile. Higher
baseline
BNP
associated
with
increased
risk of
dementia
during
follow-up in
youngest
tertile only. Tynkkynen National 14-year 7,158 Mean NT-proBNP at Medical Age, sex, Higher et al. [56] FINRISK prospective, 48 ± baseline records cholesterol, baseline NT-
(2015) Study; observational 13 for body mass proBNP
Finland years diagnosis index, ischemic associated
(range with any heart disease, with 25 to dementia and diabetes increased
74) or AD, or risk of any
dementia incident
medicati dementia
on across all
participants.
Finding
driven by
males. No
finding on
incident AD. Vaes et al. Leiden 85+ Cross-sectional, 274 All 90 NT-proBNP MMSE. Height, weight, No
[55] (2009) cohort; observational years categorized ‘Poor renal function, association.
The old according to sex- cognitive hemoglobin,
Netherlands specific tertiles of function’ and
distribution defined cardiovascular
as medication MMSE
<19. ABI, ankle-brachial index; AD, Alzheimer’s disease; BNP, brain natriuretic peptide; cIMT, carotid intima-media thickness; FINRISK,
Finland Cardiovascular Risk Study; MMSE, Mini-Mental State Examination; NT-proBNP, N-terminal pro-brain natriuretic peptide;
VaD, vascular dementia. {2 Column Table}
Table S5. Studies of depression and cognitive function in type 2 diabetes
Study Sample Design Nu Baselin Measuremen Cognitive measures Adjust Association with
m e mean t of ment cognitive function
be age depression variabl
r es Cukierma Patients Cross-sectional 2, Mean Scores ≥10 Digit Symbol Coding Age Association of n-Yaffe with type 2 analysis of trial 97 63 ± 6 on 9-item (primary outcome), depression with et al. [13] diabetes on blood 7 years Patient MMSE, Rey Auditory lower MMSE
(2009) participatin pressure, lipids, Health Verbal Learning, and scores. No
g in and glycemic Questionnair Stroop (secondary findings for other
ACCORD- control e or self- outcomes) cognitive tests.
MIND; reported
North depression
America Katon et Patients 3- to 5-year 19 Range ICD codes ICD codes for dementia in Sociod Co-morbid al. [60] with type 2 retrospective, ,0 30-75 for diagnosis hospital records, restricted emogra depression/diabet
(2012) diabetes observational 00 years of to incident cases occurring phic es associated with participatin depression/u 3 to 5 years after baseline factors, increased risk of
g in the se of anti- clinical dementia
Diabetes depressants risk diagnosis
and Aging in hospital factors, compared with
Study; records health diabetes alone.
USA risk
factors,
and
health
use Sullivan Patients 40-month trial 2, Mean Scores ≥10 Digit Symbol Coding Age, Association of et al. [61] with type 2 on blood 97 age 63 on 9-item (primary outcome), sex, depression at
(2013) diabetes pressure, lipids, 7 ± 6 Patient MMSE, Rey Auditory ethnicit baseline with
participatin and glycemic years Health Verbal Learning, and y, steeper cognitive
g in control Questionnair Stroop (secondary educati decline across
ACCORD- e at baseline outcomes) at baseline and on, cognitive tests.
MIND; 20 and 40 months glycem North ia
America treatme
nt arm,
blood
pressur
e
versus
lipid
treatme
nt arm,
blood
pressur
e
treatme
nt,
lipid
treatme nt, clinical center, cardiov ascular event, body mass index,
HbA1c
, cholest erol, smokin g, alcohol
, and insulin
use Trento et Patients Cross-sectional, 49 Mean Zung Self- MMSE Age, Statistically non- al. [58] with 2 observational 8 68 ± 7 Rating sex, significant trend
(2012) diabetes; years Depression duratio for association of
Italy Questionnair n of higher depression
e diabete scores with lower
s, MMSE scores
HbA1c
, and
insulin
use Watari et Patients Cross-sectional, 40 Range Clinical MMSE, 12 cognitive tests Age, Statistically non- al. [59] with type 2 observational 30-80 interview to resulting in composite sex, significant trend
(2006) diabetes; years. diagnose scores of and for lower overall
USA Mean depression attention/processing speed, educati cognitive function
60 ± 12 memory, executive on and statistically
years. function, verbal memory, significant lower and non-verbal memory attention/processi
ng speed in co-
morbid
depression/diabet
es group than in
no
depression/diabet
es group. ACCORD, Action to Control Cardiovascular Risk in Diabetes; ACCORD-MIND, ACCORD-MIND, Action to Control
Cardiovascular Risk in Diabetes-Memory in Diabetes; ICD, International Classification of Diseases; MMSE, Mini-Mental State
Examination.