Neurology Patient History and Intake Form ELECTRONIC FORM DIRECTIONS: PLEASE FILL OUT THE FRONT PAGE AT EVERY VISIT
Date If you need help completing this form, please ask a staff member for help. Give as many details as you know. Please note that while we may not be able to address all of the health problems listed on this sheet during this clinic visit, our knowledge of them may help us deal with your child’s needs more effectively.
Your relationship to child: Your name:
Signature of individual completing this form Relationship to patient Date Time
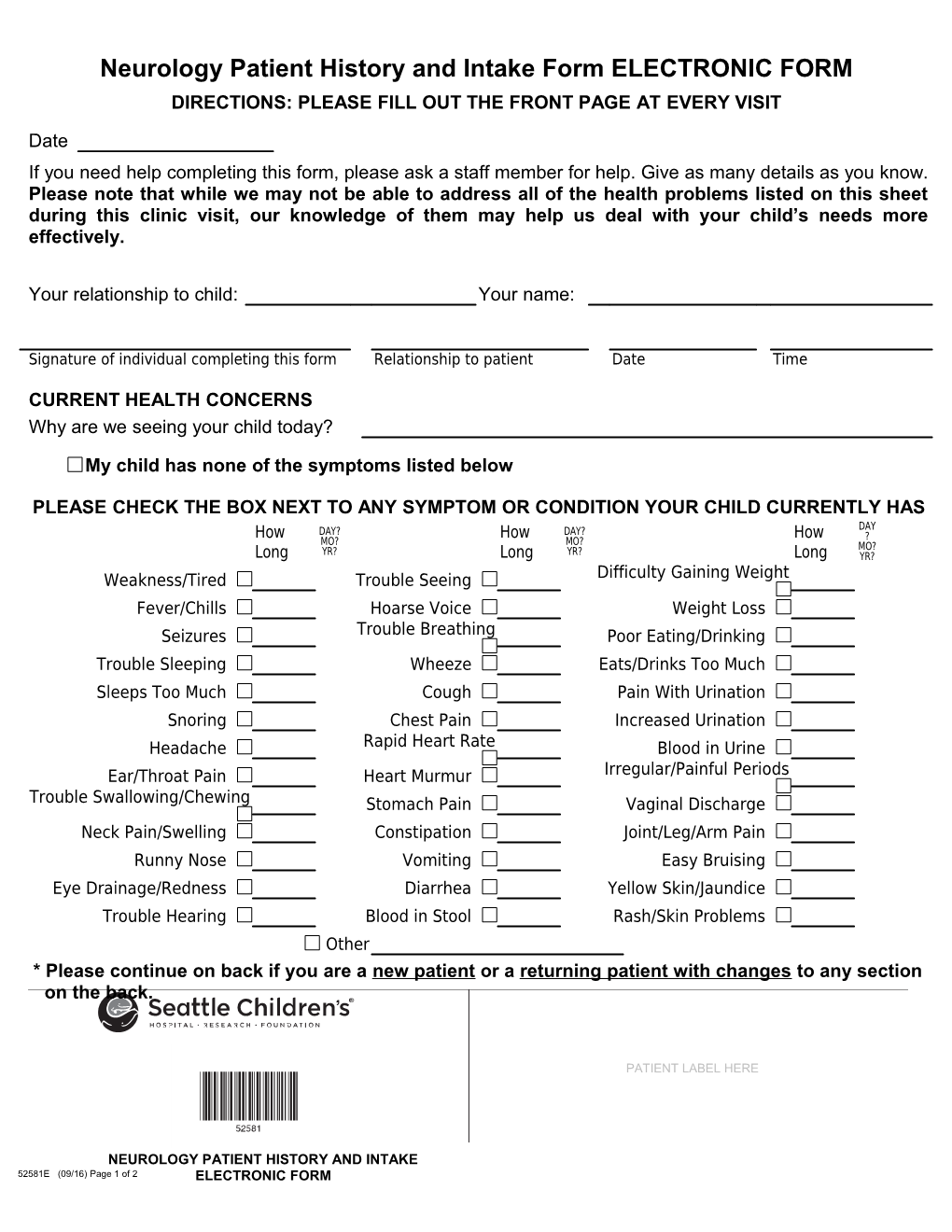
CURRENT HEALTH CONCERNS Why are we seeing your child today?
My child has none of the symptoms listed below
PLEASE CHECK THE BOX NEXT TO ANY SYMPTOM OR CONDITION YOUR CHILD CURRENTLY HAS DAY How DAY? How DAY? How ? MO? MO? MO? Long YR? Long YR? Long YR? Difficulty Gaining Weight Weakness/Tired Trouble Seeing Fever/Chills Hoarse Voice Weight Loss Trouble Breathing Seizures Poor Eating/Drinking Trouble Sleeping Wheeze Eats/Drinks Too Much Sleeps Too Much Cough Pain With Urination Snoring Chest Pain Increased Urination Rapid Heart Rate Headache Blood in Urine Irregular/Painful Periods Ear/Throat Pain Heart Murmur Trouble Swallowing/Chewing Stomach Pain Vaginal Discharge
Neck Pain/Swelling Constipation Joint/Leg/Arm Pain Runny Nose Vomiting Easy Bruising Eye Drainage/Redness Diarrhea Yellow Skin/Jaundice Trouble Hearing Blood in Stool Rash/Skin Problems Other * Please continue on back if you are a new patient or a returning patient with changes to any section on the back.
PATIENT LABEL HERE
NEUROLOGY PATIENT HISTORY AND INTAKE 52581E (09/16) Page 1 of 2 ELECTRONIC FORM PLEASE COMPLETE IF YOU ARE A NEW PATIENT OR RETURNING PATIENT WITH CHANGES CHILD’S HEALTH HISTORY Was your child born early or on time? On time Early If early, how many weeks early? Were there any Problems in the pregnancy or delivery? No Yes If yes, please describe below:
How much did your child weigh at How many days did your child stay in the hospital Hasbirth? your child ever been hospitalized? Noafter birth?Yes If yes, please describe below:
Has your child ever had any operations? No Yes If yes, please list date & reason below:
Does your child have any other chronic conditions? No Yes If yes, please describe below:
Has your child had any head injury? No Yes Is your child allergic to anything (medicines, food, other?) No Yes If yes, please describe below:
Do you have a primary care provider that handles your child’s immunizations? No Yes DEVELOPMENT/SCHOOL When did your First sit up First child…. alone? Walk? Say simple Speak in What grade is your words? What kind of gradessentences? does your Doeschild in?your child receive academic help or child get? developmental therapy? FAMILY HISTORY Please check the condition and identify family members who have any of the following: Condition Family Member Condition Family Member Heart Disease/High Blood Pressure Seizures Stroke Headaches Learning Problems Any other history of Problems with movements/tics family illnesses, stomach or Intestine Disease early deaths? SOCIAL HISTORY Who lives at home with the child? Biologic mother Biologic father Other Any stresses at home?
Does the child use tobacco, alcohol or other drugs? Was the child adopted? Yes No PATIENT EDUCATION In what ways do you prefer to learn about how to care for your child’s medical needs? Reading (written materials/pictures) Listening (one-on-one conversation) Watching (demonstration) Doing (practicing myself) Who helps care for your child? Do you have any needs (physical abilities, cultural, religion) related to your child’s care that will help us work together PATIENT LABEL HERE Ifbetter so, please with your child and family explain:
NEUROLOGY PATIENT HISTORY AND INTAKE 52581E (09/16) Page 2 of 2 ELECTRONIC FORM