Cardio January 29th, 9:00 AM Dr. Downey Matt Messa for K. Gadberry Page 1 of 5 Cardiac Muscle and Mechanincs Part 2
Cardiac Mechanical Function contrasted to Skeletal Muscle Skeletal Muscle usually operates close to L-Max, so that suggests that changes in preload are not usually very important If you change the resting length of the bicep muscle, you might be able to improve function slightly by altering the sarcomere length. As a reminder, in skeletal muscle, the two things that contribute to function include recruitment (the number of cells activated) and temporal summation (frequency of stimulation alters the force) The heart cannot use recruitment to enhance function because the number of myocardial cells that get activated with an action potential is set. The heart cannot use summation because the pacemaker sends one impulse at a time down the conduction pathway, and the action potentials are longer than in skeletal muscle Skeletal muscle contractility cannot be modulated like it can in the heart via catecholamines (epi and norepi)
Preload in the Heart Changes in preload are very important in the heart because it allows the heart to deal with varying amounts of filling prior to contraction That amount of filling is usually decided by the amount of blood that returns to the heart from the systemic circulation Preload determines the length of the sarcomere prior to activation
How does sarcomere length increase contractility force in the heart? Varying length of the sarcomere alters the overlap of actin and myosin This improves the excitation contraction coupling Please remember that changing sarcomere length may affect contractile force, but it has no effect on contractility
Factors that effect ventricular preload The most obvious one is venous return Heart Rate End systolic volume to which blood will be added Chamber Stiffness
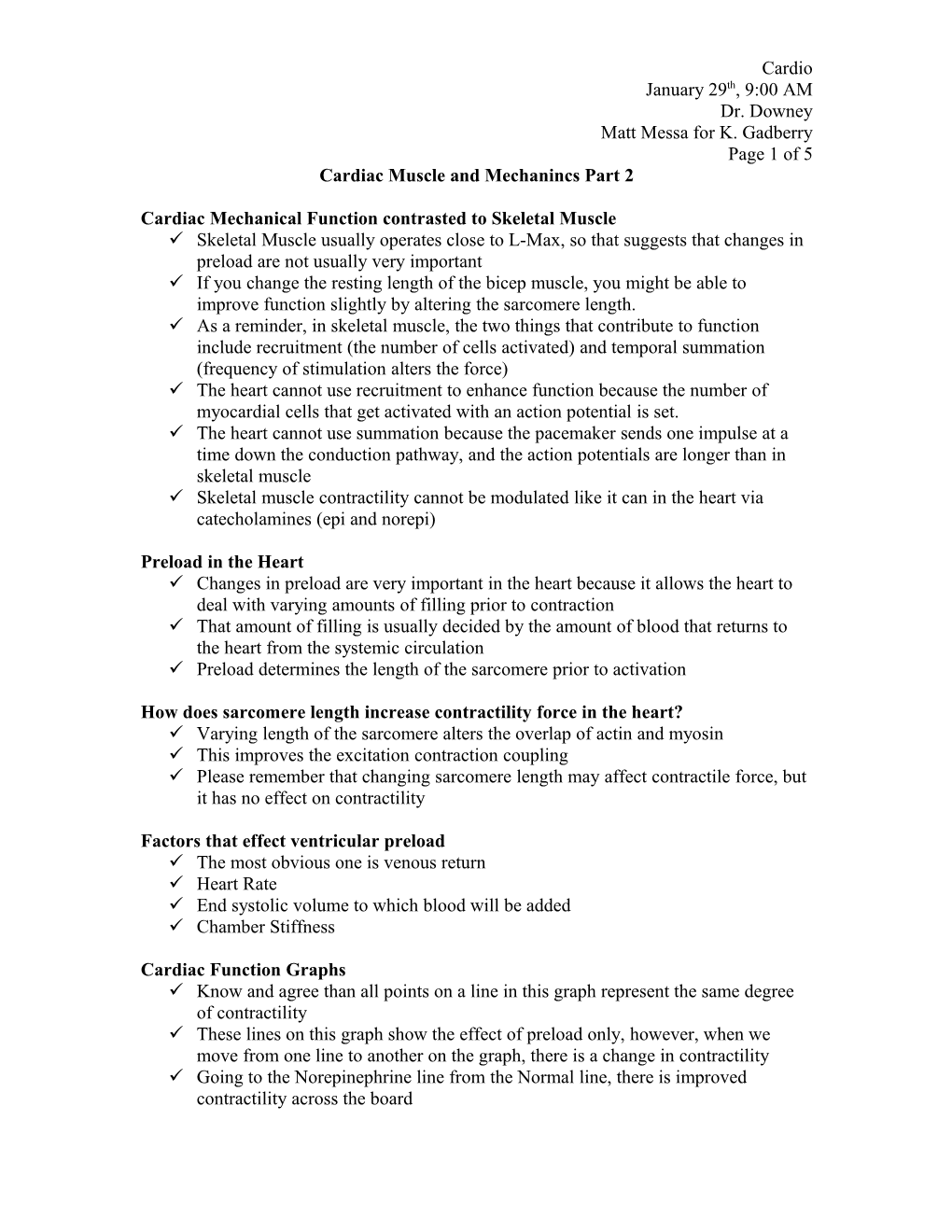
Cardiac Function Graphs Know and agree than all points on a line in this graph represent the same degree of contractility These lines on this graph show the effect of preload only, however, when we move from one line to another on the graph, there is a change in contractility Going to the Norepinephrine line from the Normal line, there is improved contractility across the board Cardio January 29th, 9:00 AM Dr. Downey Matt Messa for K. Gadberry Page 2 of 5 So Dr. Downey then asked if contractility will always be improved in the presence of Norepinephrine???? Norepi decreases preload but improves contractility. He then gave an example of a person who gets anxious and immediately starts to secrete Norepi while sitting at rest. Heart Rate has gone up, thus preload has gone down (because filling time is less), but cardiac output has not improved because peripheral venous return has not increased yet (because peripheral vasodilation has not started yet). On the line representing cardiac failure (possibly post MI), all points on the line represent depressed contractility compared to normal.
Effect of changes in preload on cardiac function. Effect of norepinephrine and heart failure are also illustrated. Norepinephrine raises ventricular contractility (i.e., stroke volume and/or stroke work are elevated at a given end-diastolic fiber length). In heart failure, contractility is decreased, so that stroke volume and/or stroke work are decreased at a given end-diastolic fiber length. Digitalis raises the intracellular calcium ion concentration and restores the contractility of the failing ventricle. Afterload He defined afterload here as the pressure that the blood has to contract against in systole He stated that he would go on to discuss afterload in more detail later
Tension-Length Relationship The ventricle is distended during diastolic filling Just like in skeletal muscle, the heart when confronted with a counterforce, must first produce an isometric contraction that does not actually result in fiber shortening Once the pressure generated by this isometric contraction exceeds the afterload (the pressure in the aorta), there will be an isotonic contraction that results in blood ejection Once the aortic valve closes, this will allow the ventricle to ISOMETRICALLY relax without changing length. The length will not go back to the pre-contraction length until the diastolic filling again occurs Cardio January 29th, 9:00 AM Dr. Downey Matt Messa for K. Gadberry Page 3 of 5 Ventricular Pressure-Volume Loops This is where we use another special graph to plot ventricular cavity pressure as a function of ventricular volume Good for examining relationships between preload, afterload, contractility, and heart rate You will notice that in this graph there is shown to be about 150ml of blood present at the end of diastole, termed “end diastolic volume” You should also recognize that the volume at the end of systole is not zero as one would expect. Instead, it is about 50-70ml EDV-ESV= Stroke Volume At point A, this is where the filling of the ventricle begins (mitral valve opens) You will also notice that there is even a slight pressure drop in the ventricle right as the mitral valve opens at point A. From B to C, you should notice that there is an increase in both ventricular volume and pressure. The pressure change is very small though because the normal myocardium is very distensible. The last short upward slope just before C represents atrial contraction. So what does this tell us? It tells us that the majority of the blood that enters the ventricles is not due to atrial contraction, but instead due to blood passively traveling through a conduit-like atria and an open mitral valve. At C, mechanical contraction has been initiated due to electrical excitation, so thus the mitral valve closes right after C, due to the ventricular pressure exceeding atrial pressure. So for a short time, the mitral and aortic valves both are closed!!, This is when the isometric (or better termed isovolumic phase) contraction occurs without any fiber shortening Notice the straight line from C to D that represents ZERO change in volume At D, the pressure in the ventricle now exceeds the pressure in the aorta (the afterload) and the aortic valve opens. This allows blood to be ejected into the aorta. As this happens, aortic pressure rises, but so does the ventricular pressure At F, when the pressure in the aorta exceeds pressure in the ventricle, the aortic valve closes Then from F to A, we have isovolumic relaxation where the size of the ventricular chamber does not enlarge. (notice the straight line from F to A representing no change in ventricular chamber size) The mitral valve opens once again at A and we do it all over again. Take the time to learn associations between the valvular events and what happens on the graph with respect to pressures (you will be able to read this graph when printed) Cardio January 29th, 9:00 AM Dr. Downey Matt Messa for K. Gadberry Page 4 of 5
Some important concepts regarding values on this graph Peak aortic pressures are very near the peak ventricular pressure at around 120 mm/Hg Diastolic ventricular pressures are not much above zero (maybe 10 mm/Hg) The pressure required to open the aortic valve occurs at point D on the graph and this represents normal diastolic blood pressure
End Systolic Pressure Volume Relationship (ESPVR) At any particular length of cardiac muscle stretching, there is a maximum isovolumetric pressure than can be generated for a particular preload and with a particular degree of contractility This graph below represents the absolute maximum isovolumetric pressure that can be generated by the ventricle at a given preload and contractility There is a point at which increasing preload does no longer increase ventricular pressure Cardio January 29th, 9:00 AM Dr. Downey Matt Messa for K. Gadberry Page 5 of 5
The End Systolic Pressure Volume Relationship (ESPVR) The line on the ventricular pressure - volume loop that defines the maximum isovolumic pressure that can be generated by the ventricle at a particular preload and a particular contractility. If contractility is increased, the ESPVR rotates upward and to the left.
LV Pressure ESPVR
LV Volume
So if a PVC were to occur (a premature ventricular contraction prior to maximum filling), the ventricle would not eject a significant amount of blood because the ESPVR is what dictates the amount of shortening of the muscle fibers. If you increase contractility by giving the patient a medication that does such, then stroke volume should increase