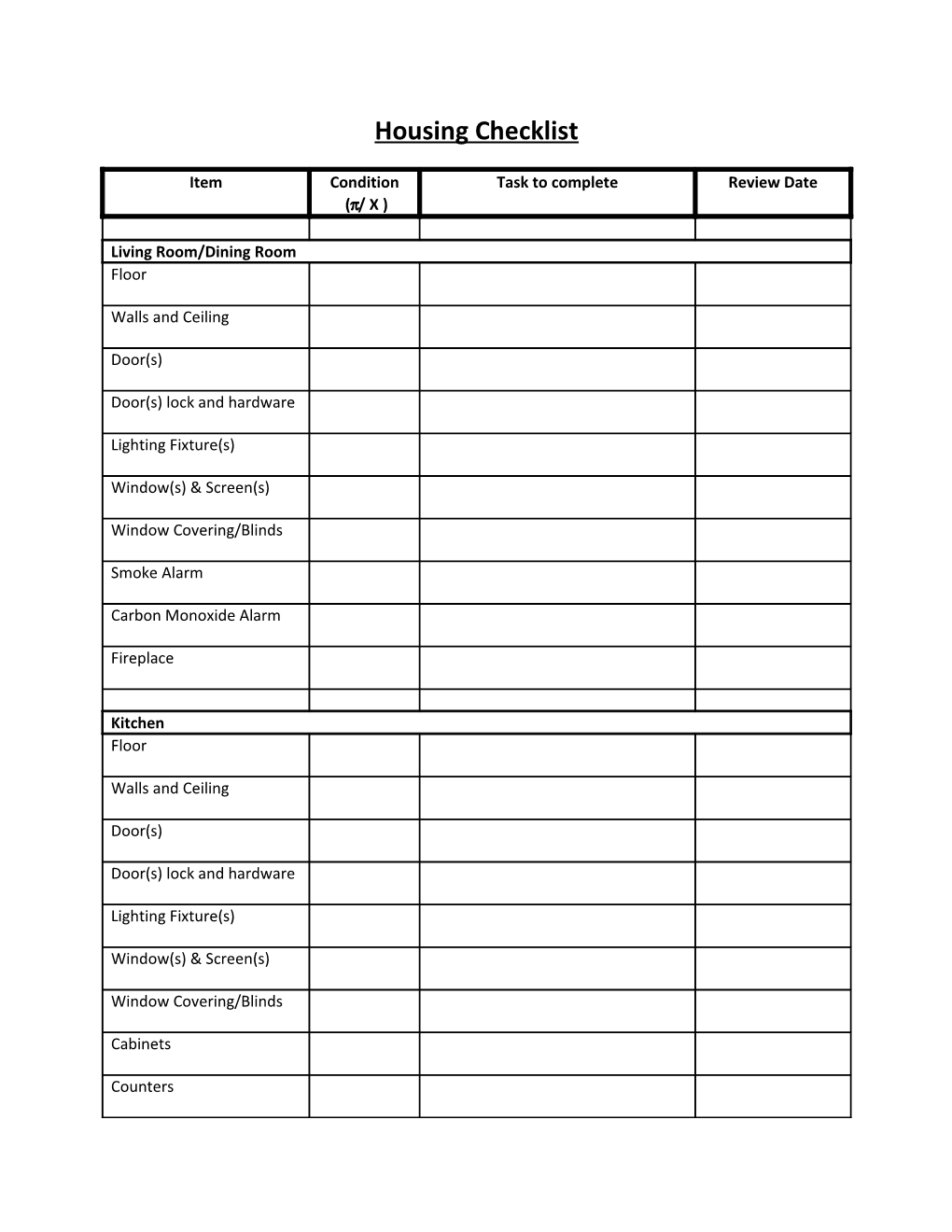
Housing Checklist
Item Condition Task to complete Review Date (/ X )
Living Room/Dining Room Floor
Walls and Ceiling
Door(s)
Door(s) lock and hardware
Lighting Fixture(s)
Window(s) & Screen(s)
Window Covering/Blinds
Smoke Alarm
Carbon Monoxide Alarm
Fireplace
Kitchen Floor
Walls and Ceiling
Door(s)
Door(s) lock and hardware
Lighting Fixture(s)
Window(s) & Screen(s)
Window Covering/Blinds
Cabinets
Counters Stove/Oven/Range Hood
Refrigerator
Dishwasher
Sink/plumbing
Bathroom(s) Floor
Walls and Ceiling
Door(s)
Door(s) lock and hardware
Lighting Fixture(s)
Window(s) & Screen(s)
Window Covering/Blinds
Sink/Plumbing
Bathtub/Shower
Toilet
Bedroom #1 Floor
Walls and Ceiling
Door(s)
Door(s) lock and hardware
Lighting Fixture(s)
Window(s) & Screen(s)
Window Covering/Blinds
Closet Bedroom #2 Floor
Walls and Ceiling
Door(s)
Door(s) lock and Hardware
Lighting Fixture(s)
Window(s) & Screen(s)
Window Covering/Blinds
Closet
Bedroom #3 Floor
Walls and Ceiling
Door(s)
Door(s) lock and Hardware
Lighting Fixture(s)
Window(s) & Screen(s)
Window Covering/Blinds
Closet
Hallway(s) Smoke Alarm
Carbon Monoxide Alarm
Floor
Walls/Ceiling Lighting Fixtures
Closet(s)
Other Heating/Cooling System
Washer
Dryer
Patio
Lawn
Parking Area
Comments:
______
______
Name Date
______
Name (Housing Case Manager) Date