PATIENTS FEEL VIOLATED IN HEALTH CARE: HOW CAN STAFF LEARN TO RECOGNISE WHEN VIOLATIONS OCCUR AND PREVENT VICTIMIZATION?
GENERAL AIM To develop and test a model of teaching health care staff to recognize abuse in health care (AHC), to handle it professionally once it happened, and to prevent AHC from happening.
Specific aims 1. To explore the awareness of AHC – according to Galtung’s model of the vicious violence triangle: direct events of violence, structural violence and cultural violence - from the staff’s perspective (definitions, own experiences) and from what can be learnt from official documents. 2. To explore direct events of AHC with focus on a potential conflict between staff’s learned belief system (structural and cultural violence) concerning AHC and their own moral values and resources. 3. To test a model to educate staff in handling AHC: protecting staff’s moral resources and modifying their learned belief systems (structural and cultural violence) by means of behavioural experiments e.g. Moral Agency Theatre. 4. To evaluate the effect of the educational model and revise theories accordingly.
OVERVIEW OF THE RESEARCH FIELD Until recently AHC was an almost unexplored research field. We have found studies about physician-patients communication (Ong, De Haes et al. 1995; Annandale and Hunt 1998), nurse-patient relations (Halldórsdóttir 1996), various kinds of assaults against patients e.g. abusive caring of demented patients (Eriksson and Saveman 2002), sexual involvement between physicians or psychotherapists and patients (Fahy and Fisher 1992; Dehlendorf and Wolfe 1998; Hetherington 2000), abuse of children in psychiatric care (Kaplan, Busner et al. 2001), and abuse within maternal care in developing countries (Jewkes, Abrahams et al. 1998; d'Olivera, Diniz et al. 2002). Except for our studies based on NorAQ and ViolEP (Swahnberg 2003; Swahnberg and Wijma 2003; Swahnberg, Wijma et al. 2004; Swahnberg, Wijma et al. 2004; Swahnberg, Schei et al. 2005; Swahnberg, Thapar-Björkert et al. 2005; Swahnberg, Wijma et al. 2005; Swahnberg and Wijma 2006; Swahnberg and Wijma 2006) (see below), we found no reports on patients’ lifetime experiences of abuse in any health care setting. Moreover, the field has so far only been explored from the patients’ perspective. In 1997 we performed prevalence studies within a Nordic research network on experiences of four kinds of abuse in female patients visiting five Nordic gynaecological clinics; emotional (EA), physical (PA) and sexual abuse (SA), and AHC (Wijma, Schei et al. 2003). The NorVold Abuse Questionnaire (NorAQ) was constructed and validated to operationalize those four kinds of abuse (Swahnberg 2003; Swahnberg and Wijma 2003; Wijma, Schei et al. 2004). Lifetime prevalence of AHC ranged between 13 and 28% in patients in the Nordic study, (Swahnberg 2003; Swahnberg, Schei et al. 2005). and was in Sweden 20%, Iceland 28% and in Norway 13% (Swahnberg, Wijma et al. 2004). At the different clinics 8-20% of all patients reported that they currently suffered from AHC (Swahnberg 2003). The reports on AHC concerned AHC in any kind of health care setting. A background of childhood abuse was associated to retraumatization in the health care system in adult patients: Adj OR: EA 3.9 (2.0-7.5); PA 1.7 (1.0-3.0); SA 3.5 (2.3-5.5); EA+PA+SA 8.9 (3.3-24.0), but still 2/3 of the victims of AHC were “new” victims (Swahnberg, Wijma et al. 2004). Further analysis in the Nordic sample revealed that bad health and experiences of
1 other kinds of abuse are the most important factors associated to adult experiences of AHC (Swahnberg, Schei et al. 2005). We also explored female patients’ experiences of AHC in a qualitative study; four categories emerged that describe AHC: felt powerless, felt ignored, experienced carelessness, and experienced non-empathy. These categories were summarised in the core category “Being nullified”. To be nullified implied loss of autonomy and human dignity to the patient (Swahnberg, Thapar-Björkert et al. 2005). Furthermore we developed the Violations of Ethical Principles Questionnaire (ViolEP) (Swahnberg, Wijma et al. 2005). In a study based on ViolEP the majority (73%)(306/420) had experienced that staff disobeyed ethical principles – autonomy, nonmaleficence, justice, and integrity - that should govern the health care. More than every second of them had perceived those events as violations (68%)(209/306)(Swahnberg, Wijma et al. 2005). We have recently also studied: prevalence of AHC among male patients with NorAQ at six clinics at the University Hospital, Linköping (n= 1767)(Swahnberg and Wijma 2006), validation of NorAQ (male version)(Swahnberg and Wijma 2006), and patients’ subjective accounts of AHC (see preliminary results below).
After extensive research on AHC from the patients’ perspectives, we now turn to the staff’s experiences and the structures/culture in which they work to find answers to the bothering questions: how can it be that patients experience abuse in an organisation aiming at helping sick people? Which mechanisms nurture/legitimate AHC? And how can AHC be prevented, i.e. how can non-traumatic behaviour in potential AHC situations be learnt and taught?
DESCRIPTION OF THE RESEARCH PROJECT Theory We have turned to ethics, sociology, cognitive theories and pedagogy to build the theoretical foundations of the study. Mechanisms of AHC Galtung describes the “vicious violence triangle” as a symbolic representation of the relations between direct, structural and cultural violence (Galtung 1990). He defines violence as “avoidable insults to basic human needs, and more generally to life, lowering the real level of needs satisfaction below what is potentially possible”(Galtung 1990) (p292). He means that direct events of violence (here AHC) are legitimised and nurtured by the two others, and that there generally speaking is a casual flow from cultural via structural to direct violence. Structural violence relates to four needs categories: survival, well-being, identity, and freedom. These categories are variations on the general theme of structurally built-in repression, and implies an unequal exchange between the “topdogs”, who get much more, measured in needs currency, out of the interaction than the others, the “underdogs”. To identify these processes a vocabulary is necessary, including terms as: exploitation, penetration (implanting the topdog inside the underdog), segmentation (giving the underdog only a very partial view of what goes on), and marginalisation (keeping the underdogs away from each other)(Galtung 1990). We will apply these theories on the information gathered in the project and evaluate whether or not this process helps understanding AHC, gives clues as to how AHC can be prevented, i.e. how non-traumatic behaviour in potential AHC situations be learnt and taught. Our hypothesis is that working on the structural and cultural level is a prerequisite to be able to prevent the direct events of AHC (Figure 1).
Glover discusses in his book “Humanity” why all the atrocities during the twentieth century could take place and be performed by “ordinary people”, and how this could be prevented
2 from happening again (Glover 2001). His answer is that a new, humanized ethics needs to be established when morals based on religious norms and values fade away. In this new, humanized ethics the key concepts are those “moral resources”, that are inherent in every human being. Moral resources are human responses (sympathy and respect) and moral identity (the type of person someone is or wants to be; character). By analysis of many examples from recent history he shows by which mechanisms human responses were eroded: propaganda against the dignity of victims by means of humiliation and cold jokes, fear, pressure to conform or obey, threats, a monopolising belief system, distance from the victims, narrowing the aim of the response to only a certain group of people, remoteness and unreality, and a deficit of moral imagination as to the consequences of the individual’s acting. Mechanisms that may neutralize moral identity are: passivity e.g. in the form of institutional momentum or moral inertia, the “habit of participation”, fragmentation of responsibility by division of labour and narrowing of attention to only bureaucratic matters, moral slide, weakened or silenced criticism and moral debate (Glover 2001). We hypothesise that Glover’s theories in general terms are applicable to AHC and will look for evidence if these mechanisms operate and can explain why AHC occurs. If so, we will use Glover’s ideas how moral resources may be strengthened as a basis on which to build the teaching interventions of the project (Figure 1). According to Glover’s theories, not only staff will be in focus of the explorative and intervening parts of the project, but also the belief system, i.e. the explicit (expressed in laws and policy documents) and the implicit one (expressed in interviews with staff and disclosed during field studies)(Glover 2001). This will help us to understand which aspects of structures/culture in health care weaken the staff’s moral resources and make it possible for AHC to exist. We hypothesise that a belief system concerning the necessity of economical cut down is a dominating belief system at present in health care, offering excuses for taking steps that otherwise would be regarded as immoral. Even if economical restrictions become necessary, there is a risk that such steps undermine staff’s moral resources; if left without debate. Teaching interventions According to Glover’s theory we will actively work with staff in order to rehabilitate/ reinforce their moral resources (Figure 1). When they earlier acted according to the prevailing belief systems against their core moral conviction that implies a conflict. The reason why they still did so, we hypothesise, is that the belief system was so firmly implanted in them that they saw no other choice. A potent medium to change a belief system is behaviour experiment (Beck 1995). We will use this fact by teaching staff Moral Agency Theatre (MAT), according to Boal (Boal 2000). This means here to act out short scenes, depicting a problematic situation of AHC. Staff interacts by replacing the characters in the scenes and improvising new ways to solve the problem. In this way the staff’s own moral resources will be used as the basis of the intervention tried out. As the experiments are done in a group of staff members, the solutions will be shared experiences, which will strengthen the participants’ moral identity. It is possible that the first explorative part of the study discloses that other interventions will also be appropriate. As the problem of AHC is unexplored scientifically in spite of its fairly high prevalence, there is not much to learn from literature about intervention methods. Moral Agency Theatre (MAT) has been used for several decades in training various categories of students and teachers and staff to implement other methods of problem solving in the area of virtue ethics in professional roles (Beauchamp and Childress 2001). We have personal experiences of teaching MAT to groups of medical students as a way of solving problems concerning violations of patients. These were very rewarding trials and highly appreciated by the students. Yet, this form of pedagogy to teach virtue ethics has not been much tried out in this specific context.
3 We will also use former victims of AHC, who are rehabilitated, as experts and use their knowledge to find out how an AHC situation, which has been observed or remembered by staff, could have been solved in non-abusive way (Wijma, Gustafsson et al. 2005). This will be an initial part of the process (post phase; Figure 1) weaved into the project; when the focus is to retrospectively analyse and find alternative ways to come out of an AHC situation that occurred. The next step will be to get the participants to recognise, while AHC is going on, that the patient may have experienced the situation as AHC, so they can afterwards react in an appropriate way to minimise the patient’s suffering (post-during phase; Figure 1) (Wijma, Gustafsson et al. 2005). The following step is to recognise what is happening (AHC) when it is about to occur and in time to find a non-traumatic way out (during phase; Figure 1). And the last step would be to prevent as far as possible such potential situations to arise by increasing the staff’s awareness about the different appearances of AHC (pre phase; Figure 1). Making the former victim the expert/teacher provides a role change, which may implicitly model staff to look for patients’ expertise in finding a way out in future, tricky situations.
As we hypothesise that the mechanisms behind AHC are generally valid, we plan to initiate a “twin” study in Iceland (IC). We are preparing for starting other similar studies in Trondheim, Norway and in Amsterdam, the Netherlands.
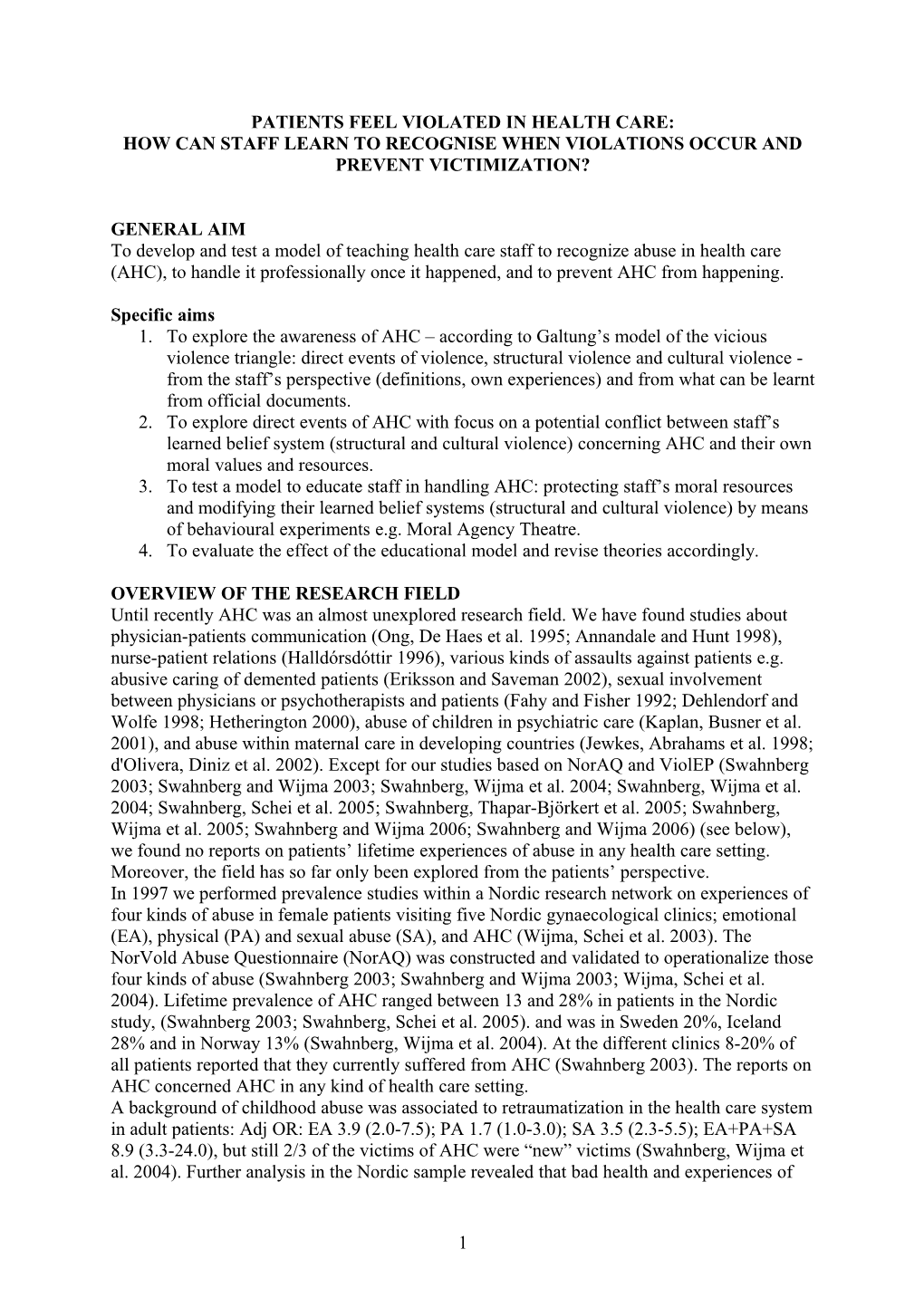
FIGURE 1
EXPLORATION INTERVENTION EVALUATION
T cultural modification of cultural violence moral belief systems violence H structrual belief systems structural conflict E necessary instaff own moral O belief systems direct events R direct events resources protection of Y implanted in staff staff’s moral resources staff’s moral resources behavioural experiments direct events
• Protect staff’s • Evaluate changes in A Explore moral resources Belief systems expressed • Explore staff’s moral I belief systems • Modify implanted in structures / by staff resources and conflict • M in structures / staff; belief systems Evaluate changes in staff’s S towards belief systems • explicit/implicit beliefs • Train alternative moral resources solutions
Phases: post during pre
M • Conclude from official documents Interviews staff, E • Conclude from official documents Interviews staff based on direct events Moral Agency Theatre • T • • Interviews staff H • Field study • Field study • Use knowledge • • Measurements* O • Interviews experts • Interviews experts of experts’ D (former victims) S • Measurements*
* to be developed within the project
4 Material and methods Sample Female and male staff (n total=60) in various medical professions at one gynaecologic and one obstetric ward in Iceland and Sweden (IC, SE) respectively. From this study population (the same throughout the project) participants will be recruited Methods Explorative part (Figure 1): Aims 1 and 2: A. Review of ethical principles expressed in official documents relevant to health care: e.g. professional ethical codes, curricula for graduate training, laws, ethical and medical (“vårdprogram”) policy documents (IC, SE) (PhD- stud. (XX), S. Thapar-Björkert (STB), K. Swahnberg (KS), B Wijma (BW), G Colnerud (GC)).. B. Interviews with female/male staff about their practising of those moral codes in every day’s work and obstacles for not following them, and about direct events of AHC, which they have heard about or taken part in (IC, SE) (XX,KS). C. Ethnographic field work with participant observations and interviews (see above) (Spradley 1980) (XX, M-L Honkasalo (MLH), KS, BW). D. Interviews with former victims of AHC who are now rehabilitated (SE) (“experts”) (XX, KS). E. Preintervention measure, with instrument which will be developed on basis of what comes out of interviews with staff (XX, GC, BW, KS). Intervention part (Figure 1): Aim 3: A. Using experts’ knowledge and B. Moral Agency. Theatre (Boal 2000) to find alternative ways of acting in AHC situations (XX, Susan Stocker (SS), BW, KS). Evaluation part (Figure 1): Aim 4: Evaluate the effects of interventions by means of repeated interviews (XX,KS). Postintervention measure, and rereview of official documents Generate theories based on our former ones and on the ongoing studies about the processes that create and maintain AHC. These theories may constitute the base for future strategies for AHC prevention (XX, STB, SS, GC, BW, KS)
Data collection will take place during 2007, analyses during 2008, and publications be written during 2008-09.
RELEVANCE OF THE PROJECT Moral phenomena are usually discussed in the context of educational or moral philosophy, yet there are few examples of empirical studies (Colnerud, 1997). It is provoking for health care authorities to learn that AHC exists and is prevalent both among female and male patients. Another factor that contributes to the uneasiness AHC creates is that it is difficult for a head of a ward to realise what he/she could do to prevent AHC. Thus acting may be delayed or totally avoided. This project tests and evaluates one model for handling AHC, based on a solid theoretical ground which gives one way of understanding the mechanisms of AHC. The mere fact that AHC is studied concretely makes it easier to accept, which is a prerequisite for preventive work. Knowing that AHC exists and not acting to prevent future experiences of abuse among patients is an impossible position to take for ethical reasons. This project may not serve the definite solution on the problem of preventing AHC, but it will present ideas how to enable staff to handle potentially traumatic situation in health care in a non-traumatic way, or how to minimise trauma once AHC occurred. Thus the project may get an eye-opener effect.
PRELIMINARY RESULTS The theoretical framework for AHC presented above has been applied it to two case studies (Wijma, Gustafsson et al. 2005; Wijma, Thapar-Björkert et al. 2006). We have recently also studied prevalence of EA, PA, SA, and AHC with a male version of NorAQ among male patients at six clinics at a university hospital in Sweden (n= 1767) (Swahnberg and Wijma 2006). The prevalence of AHC among male patients was 8%. The proportion of male patients currently suffering from abuse was highest for EA and AHC.
5 More than every second male patient who reported AHC also reported current suffering from The male version of NorAQ has been validated in this male patient sample (n=86). Questions about abuse proved good reliability and validity (Swahnberg and Wijma 2006). Finally we have just completed a qualitative study about male patients’ experiences of AHC. Compared to the female patients who felt nullified by AHC, our male sample expressed a crisis of confidence and much frustration. The narratives described feelings of distrust from staff as well as towards staff. The confidence seamed to be broken in both directions(Swahnberg, Thapar-Björkert et al. 2006).
INTERNATIONAL COLLABORATORS IN RESEARCH ON ABUSE Tora Stengrimsdottir, MD PhD, Reykjavik, Iceland. Prof B Schei, Women’s Health, Univ Trondheim, Norway. Prof M-L Honkasalo MD, Med Anthropology, Helsinki Univ, Finland. Ass. Prof. Suruchi Thapar-Björkert, Sociology, Univ. of Bristol, UK. Prof. N. Prakash, Sociology and Women’s Gender Studies, Birla Instit of Technol and Science, Pilani, Rajastan, India. Iryna Mogilevkina, MD PhD, Donetsk, Ukraina. Ass. Prof. Susan Stocker, PhD, Ethics University of Amsterdam, the Netherlands.
ETHICAL ASPECTS Our study requires informed consent from participants but not approval by a regional ethical board. There is a risk that some participants might find it uncomfortable to participate in the study. On the other hand, participation is voluntary, and the knowledge gained through the study can be of great importance for prevention and a general understanding of AHC. Thus our judgment is that the value of the research project legitimizes the distress that it might cause some of the participants. Moreover, knowing that AHC exists and is prevalent makes it ethically unacceptable not to try ways to prevent AHC/minimize the trauma caused.
GENDER ASPECTS Structural violence is located in social structures where individuals act towards one another according to their position. It is built into the functioning of bureaucratic systems and can nurture relationships of power and powerlessness. The embedded inequalities in social structures and relations are added to the fact that power inequalities exist between women and men. The impact of structural violence is thus gendered, and, very likely, so will future strategies for AHC prevention. In the research project about AHC three different hierarchical structures can be identified: 1 between female and male patients/staff; i.e. the patient is subordinated staff who has the power to help the patient; 2. between the different categories of staff in the health care system; 3. as one third of female patients reporting AHC has a background of childhood abuse they feel even more subordinated when they apply for help, and are easily retraumatized in the health care system. Gendered power inequalities are involved in all these three hierarchies. In the present study all three levels of hierarchical structures are studied and considered important.
PEDAGOGIC RELEVANCE The focus of this project is how virtue ethics in the field of ACH is learnt and can be taught in an interprofessional context. Its aim is to find models to protect staff’s moral resources in times of economical cut-down, which are supposed to create a moral conflict in staff. The results of this pedagogic try out will have a more general value than concerning merely AHC,
6 as models for handling moral conflicts probably can be applied to other moral conflicts arising in hierarchal structures. We perform the study in at least two countries, Iceland and Sweden, and want to make replicas also in Norway and in the Netherlands. But these two latter projects need the support from the present study to become accepted, in terms of e.g. grants or preliminary results. The main relevance of this project is that it tries out ways to handle the pedagogic challenge of learning and teaching morally acceptable ways to concretely act in potential AHC situations in a way which prevents or minimises trauma. This is an urgent task.
COLLABORATING UNIVERSITIES Linköping University, Faculty of Health Sciences, (Prof. B Wijma, K Swahnberg) and Faculty of Philosophy, (Prof. Gunnel Colnerud) Sweden. Thora Steingrimsdottir, Department of Gynecology, Landspitalinn, Reykjavik, Iceland Prof M-L Honkasalo MD, Med Anthropology, Helsinki University, Finland. Ass. Prof. Susan Stocker, ethics, University of Amsterdam, the Netherlands. Ass. Prof. Suruchi Thapar-Björkert Sociology, University of Bristol, UK.
CO-FINANCING FROM UNIVERSITIES Linköping University: Professor B Wijma 30% (SEC 350 000) employment in the present and in other pedagogic projects, Professor M-L Honkasalo 10% (SEC 74 000) employment in the present project, and Professor G Colnerud 10% (SEC 74 000) in the present project. Comment to the budget: the present budget includes extra salaries for supervision of staff in the Icelandic twin study. If this part of the study is not accepted the following reduction of salaries are to be made: T Steingrimsdottir 10%, SA Bóasdóttir 10%, S Stocker 10%, K Swahnberg 10%.
REFERENCES
7