Accessing social capital and ‘goods’ online: the contingent role of the Internet in parenting someone with Rett syndrome
by
Jo Hope
Submitted for the Degree of Doctor of Philosophy
School of Social Sciences Faculty of Arts and Human Sciences
VOLUME I: MAIN BODY OF THESIS
Supervisors:
Dr Christine Hine Dr Sarah Earthy
Word count: 84,769
© Jo Hope 2015 Declaration
This thesis and the work to which it refers are the results of my own efforts. Any ideas, data, images or text resulting from the work of others (whether published or unpublished) are fully identified as such within the work and attributed to their originator in the text, bibliography or in footnotes. This thesis has not been submitted in whole or in part for any other academic degree or professional qualification. I agree that the University has the right to submit my work to the plagiarism detection service TurnitinUK for originality checks. Whether or not drafts have been so-assessed, the University reserves the right to require an electronic version of the final document (as submitted) for assessment as above.
Signature: ______
Date: ______
2 Abstract
Our current understanding of the use of online support and information among parents of people with rare syndromes is fragmented, both theoretically and methodologically. This thesis aimed to provide a more coherent picture by using Bourdieu’s concepts of capitals, habitus and fields to explore the interplay between the social differentiation of online support use and its role within the wider caring practices of parents of people with Rett syndrome. A mixed mode, mixed method approach was used. Parents were recruited through a charity’s mailing list and communication channels and through relevant online support sites. 190 parents completed a survey about Internet and online support use. Twenty of these parents took part in detailed interviews about their use of online peer support sites. Age most strongly differentiated the use of the Internet for caring-related information and support. Time-related variables (age of parent, age of child and years since diagnosis) strongly differentiated the use of online peer support and fewer years since diagnosis was associated with gaining greater benefits from online peer support. Use of online peer support in everyday caring practices was dynamic and changed in relation to alternative sources of social capital, current need and level of relevant expertise. Interviewees with adult children had lower information and support needs overall and online support sites, used predominantly by younger carers, offered them few useful ‘goods’, except keeping abreast of developments in research and treatment. Wealthier parents tended to use blogs to read and trade information. There was a suggestion that more educated interviewees accessed a range of primary sources of information while less educated parents relied upon online peer support as a primary source of information. These findings demonstrate the importance of exploring online caring and health practices within a wider social, historical and personal context.
3 Acknowledgements
My husband, Jason, has been incredibly patient and supportive throughout my PhD, taking on a greater share of housework and acting as a sounding board as I’ve worked through numerous iterations of my argument. My mum, sister Kate, and step-sister Liz have been incredibly generous with their time in proofreading my final draft. My dad, step-mum, mum, and step-dad have all provided practical support to help me protect my PhD time. My supervisors, Christine Hine and Sarah Earthy, have provided exactly the right amount of advice and I feel lucky to have benefitted from their input. Other researchers in the department have provided useful feedback at critical times (thank you to Rob Meadows, Ian Brunton-Smith, Jo Moran-Ellis, Rachel Brooks and Andy King). I have benefitted in all kinds of ways from the support and company of my fellow PhD students: Lorraine Locke, Linnéa Österman, Richard Green, Richard Fletcher, Alex Seal, Miriam Dunst, Judith Sleney, Tara Knights, Sophie Sarre, Eva Martinez-Cruz, Peter Johnson, Fiona Wadie, Cornelia Wilson, and Michelle Webster. I could not have carried out this research without the support of some extremely important people and organisations. The Economic and Social Research Council (ESRC) funded my research through the South East Doctoral Training Centre (SEDTC). Rett UK, particularly Debbie Main, supported me in recruiting their members to my study, allowed me access to an anonymised version of their database, and invited me to an event to meet parents and pilot my questionnaire. Moderators of some key online support sites were kind enough to allow me to post information about my study online. Finally, and most importantly, warm thanks are due to the parents who contributed to my research (by completing a survey, completing a form about why they decided not to complete a survey, offering me advice about my survey, taking part in an interview or showing an interest in my work). I appreciate all of you taking the time to support this research and I hope that I have done justice to your experiences.
4 Contents: Volume I
This thesis is presented in two volumes. The main body of the thesis is presented in Volume I. The Appendices are presented in Volume II.
Contents: Volume II Appendices………………………………………………………………………………………………..291 Details available in Volume II
5 List of Tables
Table Page 1.1 Current diagnostic criteria for Rett syndrome (Neul et al., 2010) 15 3.1 Ties by formality and direction (Ferlander, 2007) 55 3.2 Ties by strength and diversity (Ferlander, 2007) 55 4.1 Research questions, relationship to Bourdieu’s concepts and methods used 82 4.2 Hypotheses to be tested in Stage 1 86 4.3 Recruitment channels for survey respondents 95 4.4 Comparison of individual data from Rett UK database with sample 96 demographic data 4.5 Household information comparison between Rett UK members and survey 98 respondents 4.6 Demographic details of interviewees by mode of interview chosen 106 5.1 Frequencies and percentages of use of the Internet among key groups 119 5.2 Frequencies and percentages of use of generic online support and advice 121 among key respondent groups 5.3 Frequencies and percentages of use of online peer support among key 123 respondent groups 5.4 Relationships between key variables and use of online support and 125 information among survey respondents 5.5 Percentage of use of each platform for support and information related to 127 caring for a child with Rett syndrome 5.6 Use of different platforms by age, income and education 128 5.7 Social differentiation of the use of different online platforms by income, 129 education and age 5.8 Rated generic online support as ‘important’, ‘very important’ or ‘essential’ 132 by age, income and education group 5.9 Social differentiation of the use of different online platforms by income, 132 education and age
6 Table Page 5.10 Benefits experienced from online peer support by age, income, education and 134 occupation 5.11 Social differentiation of the benefits of reading online peer support sites and 135 groups 5.12 Benefits experienced from contact with another carer on an online support 138 site by age, income and education 5.13 Benefits experienced from contact with another carer on an online support 139 site by occupation 5.14 Social differentiation of online support use within income, education, age of 141 parent and occupational groupings 5.15 Descriptive statistics on key variables by age group of respondent 143 5.16 Strength of relationship between age of respondent and key variables of 144 interest 5.17 Social differentiation of use of the Internet and online sources of information 146 and support by key variables 5.18 Social differentiation of use of different online platforms and benefits gained 148 from online support sites and groups 5.19 Frequencies of use by age of child, where age of child is most strongly 149 associated with differentiation 5.20 Frequencies of use by years since diagnosis, where years since diagnosis are 150 most strongly associated with differentiation 7.1 Use of different modes of support by survey respondents 226
7 List of Figures
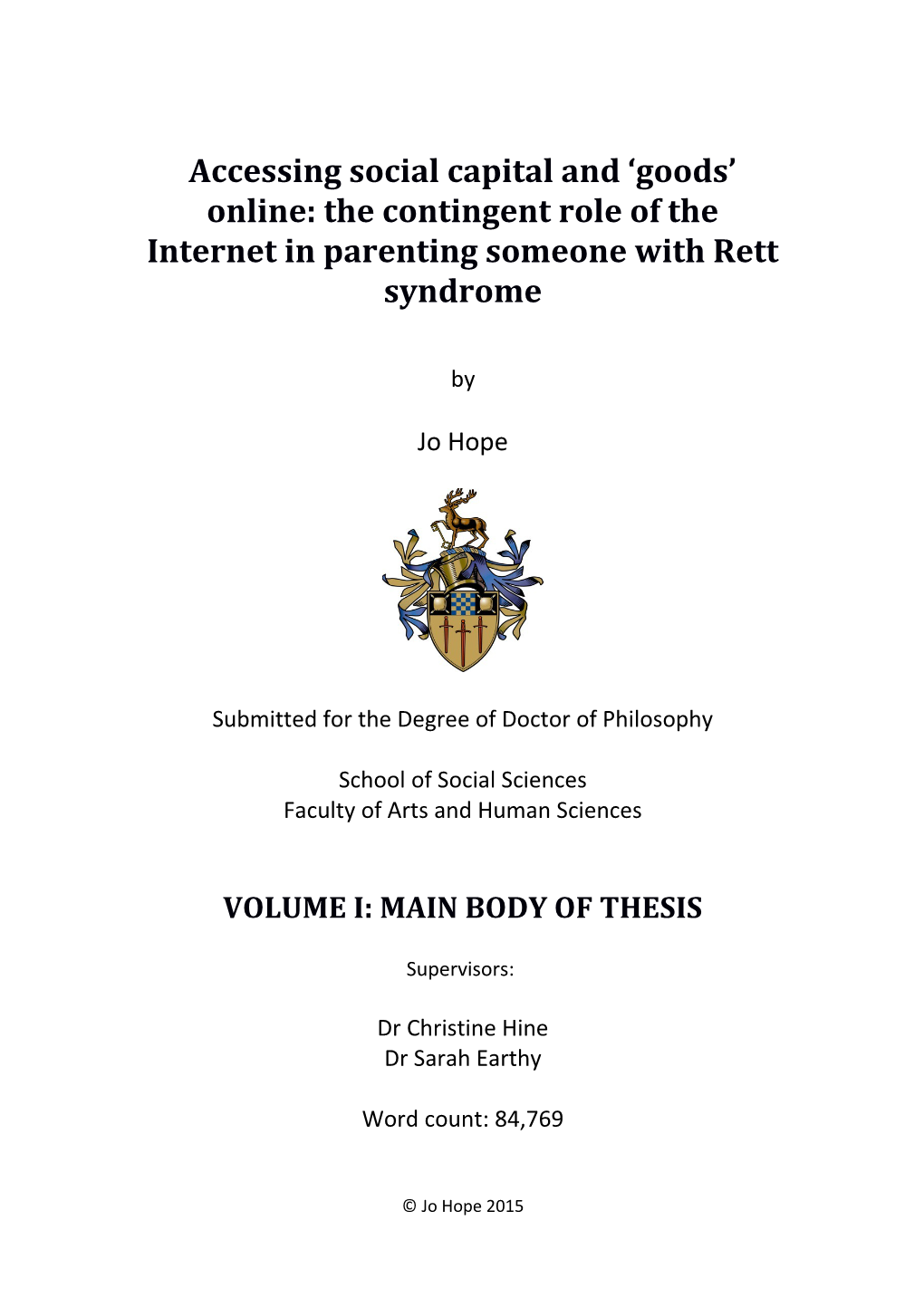
Figure Page 1.1 Timeline showing technological, social, research and medical context for 21 survey respondents 6.1 Amassing expertise and social capital and repairing biographical disruption 161 – parents’ changing needs over time
8 Chapter 1. Why now and why Rett syndrome? Understanding the context of this research
This chapter has three aims: to outline the rationale for my research, to orient readers to the socio-historical context of Rett syndrome and to describe how this thesis is organised. In section 1.1, I outline briefly why there was a need for this research and the broader significance of my findings. In section 1.2 I provide a brief introduction to the socio-historical context of caring for someone with Rett syndrome. Finally, section 1.3 summarises the content of the following chapters in this thesis.
1.1 The need for this research now
The development of the Internet has changed the wider landscape of parenting and health, both in terms of providing wider access to a range of health information (Nettleton, 2004) and opportunities to seek advice from remote peers (Davidson, 2008; Saukko, 2009; Valentine & Skelton, 2008). These developments may be particularly pertinent for parents of people with rare genetic syndromes, following the rapid development of new technologies and research in the wake of the Human Genome Project, and the ‘explosion’ of syndrome-specific sources of online support and advice (Skinner & Schaffer, 2006). Online peer support sites can provide information and advice to parents of people with rare syndromes and disabilities (Huws, Jones, & Ingledew, 2001; Jones & Lewis, 2001; Leonard et al., 2004; Schaffer et al., 2007). However, as I argue in Chapters 2 and 3, our understanding of how the use of online support and information fits into wider information-seeking, online and caring practices is fragmented along methodological, theoretical and ultimately epistemological lines. This has limited our understanding of how the use of online
9 support and information fits into a wider social and historical context, and how and why carers’ use of online support and information might be socially differentiated. In this thesis I take a novel methodological and theoretical approach to this field, described in Chapters 3 and 4. This brings together approaches and ideas from Internet research, the sociology of health and illness and the theoretical work of Pierre Bourdieu. My aim was to provide a more coherent understanding of whether the use of online support and information is socially differentiated, how it fits into wider everyday social practices and to shed new light on the interplay between structural and micro differences in the use of online support and information among parents of people with a rare syndrome. As discussed in Chapter 4, the focus on a single case study group meant I could avoid some of the pitfalls of previous research, where differing experiences and a different socio-historical context makes drawing conclusions across groups difficult. The research findings, reported in Chapters 5-7 and summarised in Chapter 8, provide a rich and coherent picture of how parents’ use of online support is influenced by a range of intersecting factors, and how combining this with an understanding of social differentiation can produce results that shed light on the dynamic use of a range of information and support over a carer’s career. The following section describes my choice of case study group – parents of people with Rett syndrome. This acts as an orientation for the reader into the social, historical, technological, support and medical context within which caring practices are and have been carried out by parents of people with Rett syndrome.
1.2 The choice of parents of people with Rett syndrome as a case study
This section describes both the process of choosing this case study group as well as orienting readers to the socio-historical context of Rett syndrome and how it might influence the information and support-seeking needs of parents.
10 1.2.1 Why Rett syndrome? In previous employment I have worked with people with profound and multiple learning disabilities and their families and developed a reasonable awareness of the kinds of caring dilemmas parents face with little local support or information. I became interested in the use of the Internet among parents of people with rare syndromes while working at the learning disability charity Mencap and contributing to a working group on the development of an online parents’ forum. While carrying out my Masters in Social Research at the University of Surrey, I created a research proposal for an online methods assignment that I later developed into this research. I was particularly interested the experiences of parents of people with a rare syndrome, whose information needs I felt were distinct, for the reasons cited above. This raised interesting questions about how parents of people with rare syndromes involving high and complex caring demands may use online information and particularly what role online peer support might play in their wider information seeking and caring work. There were a number of reasons why I felt that parents of people with Rett syndrome were a particularly suitable case study group to explore these issues. Firstly, profound and multiple learning disabilities (PMLD) in females are often associated with Rett syndrome (Kerr, 2002). Secondly, Rett syndrome is very rare, with an estimated prevalence of 2500 females in the UK (Neurological Alliance, 2003), with male prevalence much lower and estimates not available (Kerr, 2002). This reduces the likelihood of parents having local peer support. Thirdly, Rett syndrome has been found to occur randomly in 99.2% of cases (Mari et al., 2005) meaning examination of social differentiation of the use of online support is a meaningful exercise. Fourthly, there are a number of online support sites aimed at parents of people with Rett syndrome as well as sites and email groups for parents of people with special needs or PMLD. Fifthly, Rett syndrome is at the forefront of a new wave of research into the theoretical reversal of neurological symptoms in genetic syndromes (Guy et al., 2007). It is likely that genetic research will continue to develop and challenge our understanding of various syndromes and conditions, both rare and common, and raise the possibility of new treatments and approaches to medical intervention and support. I therefore felt that parents of people with Rett
11 syndrome would also provide some timely insights into the role of online information and support in the wider caring practices of carers of people with neurological syndromes at a time of great social and technological change.
1.2.2 The shifting nature of the diagnosis of Rett syndrome The characteristics of what is now called Rett syndrome were first described in a German academic paper in 1966 by Andreas Rett and in the late 1970s by Japanese researchers, Ishikawa and colleagues (1978) (Smeets et al., 2011). However, it was not until 1981 that Hagberg, a Swedish clinician, shared his findings at the Manchester Meeting on Child Neurology (Smeets et al., 2011) and subsequently published a paper for an international journal audience (Hagberg, et al., 1983). This led to a more widespread knowledge of the syndrome (Lotan et al., 2010; Smeets et al, 2011) and to the formation of the International Rett Syndrome Association in America in 1984 (now the International Rett Syndrome Foundation) (IRSF, 2008) and of the Rett Syndrome Association (now Rett UK) in the UK in 1985 (Rett UK, n.d.). The diagnostic description of Rett syndrome has changed over time and Table 1.1 is a reproduction of the most recent criteria developed by clinicians (Neul et al., 2010). As can be seen in Table 1.1, these criteria allow for a wide-ranging typical diagnosis and a range of atypical manifestations.
12 Table 1.1 Current diagnostic criteria for Rett syndrome (Neul et al., 2010)
Consider Rett syndrome diagnosis when postnatal deceleration of head growth is observed
Required for typical or classic Rett syndrome A period of regression followed by recovery or stabilisation 1. All main and all exclusive criteria 2. Supportive criteria are not required, although often present in typical Rett syndrome
Required for atypical or variant Rett syndrome 1. A period of regression followed by recovery or stabilisation 2. At least 2 of the 4 main criteria 3. 5 out of 11 supportive criteria
Main criteria 1. Partial or complete loss of acquired purposeful hand skills 2. Partial or complete loss of acquired spoken language1 3. Gait abnormalities: impaired (dyspraxia) or absence of ability (apraxia) 4. Stereotypic hand movements such as hand wringing/squeezing, clapping/tapping, mouthing and washing/rubbing automatisms
Exclusion criteria for typical Rett syndrome 1. Brain injury secondary to trauma (peri- or postnatally), neurometabolic disease or severe infection that cause the neurological problems 2. Grossly abnormal psychomotor development in the first 6 months of life2
Supportive criteria for atypical Rett syndrome3 1. Breathing disturbances when awake 2. Bruxism4 when awake 3. Impaired sleep pattern 4. Abnormal muscle tone 5. Peripheral vasomotor disturbances 6. Scoliosis/kyphosis5 7. Growth retardation 8. Small cold hands and feet 9. Inappropriate laughing/screaming spells 10. Diminished sensitivity to pain 11. Intense eye communication and eye-pointing behaviour
1 This includes babbling 2 This means major normal milestones are not met, e.g. head control, swallowing, social smiling 3 Some of these criteria may not manifest until someone is older, in which case, ‘probably atypical Rett syndrome’ should be the diagnosis and should be reassessed as they get older. 4 Teeth grinding 5 Forms of severe curvature of the spine 13 Regression is a key feature required for all kinds of diagnosis, which means that an atypical form known as ‘early onset seizure variant Rett syndrome’ was excluded from this description of Rett syndrome. It is important to note that the diagnosis of even typical Rett syndrome can range in severity in terms of, for example, ability to use a limited amount of spoken language or retain any mobility. In addition, for atypical kinds, the supportive criteria may not be observable in young children, so a definitive diagnosis may not be possible until a child is older. An important aspect of diagnosis noted in the accompanying article is that as Rett syndrome has now been found in boys, boys who meet the typical diagnosis of Rett syndrome should now be given this diagnosis (Neul et al., 2010). The development of gene technology and identification of gene mutations involved in Rett syndrome has led to a range of challenges and changes to how it is conceptualised and diagnosed (Smeets et al., 2011). Numerous mutations are related to symptoms of Rett syndrome and mutations on a particular gene (MECP2) are also found in other neurological syndromes. This has led to disagreements about whether Rett syndrome should be diagnosed by genetic test or clinical assessment (Neul et al., 2010). At the time of carrying out my research, the NHS policy was to make a clinical diagnosis first, with the possibility that a blood test ‘can be carried out’ to look for the specific genetic marker (NHS, 2012). The technology for testing for genetic markers of Rett syndrome has also changed over time, meaning that certain kinds of mutations that were not detectable until the turn of the century are now routinely sought if initial tests don’t find an obvious genetic mutation (Smeets et al., 2011). In summary, parents’ experiences of the diagnosis of Rett syndrome take place in shifting and contested contexts. The diagnosis itself may not be definitive as it may be given provisionally and be subject to change. Given the continuing developments in genetic diagnosis of Rett syndrome, it is also possible that a definitive diagnosis may later be changed if it is found to be characteristic of a particular genetic profile.
14 1.2.3 Difficulties in anticipating the prognosis of Rett syndrome As well as variations in symptoms and severity of symptoms, Rett syndrome is not a static condition, so attempts have been made to create a stage model of the syndrome, which have been summarised by Smeets and colleagues (2011). Characteristics of these stages are described in more detail in Appendix 1. Stage I involves some developmental problems that are usually within the parameters of what is considered to be normal development, so unlikely to be considered unusual by medical professionals. Stage II, which involves rapid regression and loss of skills is, as argued by Neul and colleagues (2010), the hallmark of Rett syndrome. It is a very distressing period for parents. The loss of the young child, who had appeared to be developing normally, has been described vividly by Beth Johnsson in her blog for The Independent:
the little girl you have watched turn miraculously from a baby into a toddler, who can say ‘mummy’ and ‘duck’ and babble incessantly to her dolls, who can crawl and is just starting to toddle around delightfully unsteadily, who can turn the pages of her favourite books and grasp an open cup firmly with two hands – this girl is gone. (Johnsson, 2013)
Stage III is a mixture of loss of motor skills, an ‘awakening’ and some regaining of skills, however some children move directly from Stage II to Stage IVB. Stages IVA and IVB involve deterioration (muscle wastage, degeneration of tissue and ‘frozen rigidity’), however eye-pointing communication is still preserved even at this stage (Hagberg, 2002; Smeets et al., 2011, p. 116). The differing manifestations of the stages mean there is a great deal of variation in how these stages develop in individuals. The length of some stages can vary considerably (e.g. one stage can last up to decades), some stages can be skipped entirely and there is symptom variation within the stages themselves. Nonetheless, these descriptions are the best current outline of how the syndrome develops and changes over time and are well cited in the literature.
15 A current area of interest is whether specific genetic profile can predict the manifestation of Rett syndrome (see research undertaken by the International Consortium of Rett Syndrome Clinical Researchers6). However, Halbach and colleagues (2012) suggest that clinicians should be careful about using a genetic profile as a way of predicting an individual’s prognosis because while they have found correlation between the specific characteristics of Rett syndrome and genetic profile, the severity of the syndrome varies greatly. Predicting the lifespan of somebody with Rett syndrome is problematic, given the range of associated health problems and a high relative incidence of unexplained and sudden death (Kerr et al., 1997). However, one person with Rett syndrome has been recorded as surviving to 79 years old (Lotan et al., 2010). There is therefore a great deal of uncertainty in the current research, meaning the severity of the impact of Rett syndrome on an individual is currently impossible to predict. This means that trying to understand the meaning of the diagnosis for one’s child is very difficult.
1.2.4 The care needs of people with Rett syndrome Hagberg’s (2002) list of common symptoms (updated by Smeets et al., 2011) is helpful in outlining the most common likely support needs of people with Rett syndrome. These symptoms include serious medical problems that require continual (and potentially increasing) care support (severe curvature of the spine) and which, in some cases, can lead to sudden death (irregular breathing). Some of these symptoms will be particularly distressing for carers to manage on a daily basis (like long – sometimes days-long – episodes of unexplained screaming, seizures that may or may not be epileptic, and eating and digestive problems). Other symptoms will be very demanding and difficult to manage, raising ethical dilemmas in caring practices (hand stereotypes, sleep problems, teeth grinding, and impaired perception of pain).
6 See http://www.rettsearch.org for details.
16 1.2.5 A future possibility of treatment? The most dramatic and high profile development in recent research has been the apparent reversal of the observable effects of Rett syndrome-like behaviours in mice, where the expression of the MECP2 gene was artificially deactivated and then reactivated (Guy and colleagues, 2007). This suggested that the neurological impact of the MECP2 mutation may not be permanent and irreversible, although it “do[es] not suggest an immediate therapeutic approach” to Rett syndrome (Guy et al., 2007, p.1147). In the wake of this finding, a number of charities were set up in the UK and elsewhere to fundraise for further research. In the UK, Reverse Rett, formally the Rett Syndrome Research Trust UK, works in partnership with the US-based Rett Syndrome Research Trust “to speed treatments and cures for Rett Syndrome and related MECP2 disorders” (Reverse Rett, n.d.). Current strands of (animal and cell) research funded by Reverse Rett include learning more about the detailed cell mechanisms behind Rett syndrome, searching for ways to increase MeCP2 protein, finding ways to bypass MeCP2 and finding ways to treat the individual symptoms of Rett syndrome (Reverse Rett, n.d.). Since this research began a new organisation, Cure Rett, was founded that aims both to raise money to provide support for families and for researchers “to develop treatments and find a cure for Rett Syndrome” (Cure Rett, n.d.) In terms of treatments for specific symptoms of Rett syndrome, there has been considerable progress in research into the heart and breathing-related problems in Rett syndrome and the neuronal mechanisms underlying them (Smeets et al., 2011). At the time of carrying out this research, the search for a cure was ongoing. It is beyond my competence as a researcher to assess the feasibility of a ‘cure’ for Rett syndrome, so I can only note that this is a complex area of current research that is difficult for a non-specialist to understand. This means that many parents (barring those of course who are specialists in relevant fields) will need to rely upon intermediaries to communicate the meaning of these strands of research and are likely to come to different understandings and beliefs about what ‘the cure’ might mean for their child. The field of ‘cure’ research therefore has the potential to
17 be a very emotive but also very complex topic for parents attempting to understand the meaning of the diagnosis for their child.
1.2.6 Mapping the socio-historical experiences of different carers In summary, Rett syndrome is still a relatively new diagnosis. Gaining a diagnosis of Rett syndrome can be difficult and is subject to change over time. Tests for Rett syndrome have developed over time and now can include a genetic component. The prognosis of Rett syndrome, particularly the onset and severity of symptoms, is currently unpredictable. Research into ‘the cure’ is in its early stages although there had been advances in the treatment of specific symptoms. Available support and information sources have changed over this period, as have the communication channels available for parents wishing to make contact with peers and useful organisations. In order to provide a context for the remainder of this thesis, Figure 1.1 summarises the important milestones in the development of relevant research, technology and support related to Rett syndrome and places the experiences of survey respondents within this context. As can be appreciated, parents with children of different ages are likely to have had quite different experiences of gaining a diagnosis, of attempting to understand the meaning of Rett syndrome for their child, of the kinds of information and support available, and of access to information through different communication channels.
1.3 The structure of this thesis
This chapter has provided a context for the rest of the thesis, by arguing for the development of a better and more coherent understanding of the role of online support and information in the wider caring practices of parents of people with a rare syndrome. It has provided some contextual background about the case study group of parents of people with Rett syndrome, putting forward a case for why they are a significant group that can add to our wider understanding of the role of online
18 support and information in the caring practices of people with a range of rare syndromes, particularly those where the genetic basis is being researched.
19
1963 2013
Figure 1.1 Timeline showing technological, social, research and medical context for survey respondents
20 Chapter 2 develops my argument that our current understanding of the use of online support and information among parents of people with rare syndromes is limited and fragmented, and suggests how approaches within the fields of Internet research and the sociology of health and illness could be combined to address aspects of this fragmentation. Chapter 3 explores the utility of Bourdieu’s concepts of social and cultural capital, fields and habitus for carrying out this research. It ends with a set of research questions that aim to develop a more coherent approach to understanding the interplay between structure and agency in the use of online support and information among parents of people with a rare syndrome. Chapter 4 describes the mixed method, mixed mode approach used to explore the research questions outlined in Chapter 3. Chapters 5-7 present the findings. Chapter 5 presents data on the social differentiation of the use of online support and information among survey respondents. Chapter 6 describes how the use of online support and information in this sample is contingent upon habitus, social and cultural capital, expertise and needs. Chapter 7 explores the position of online information and support seeking within existing power structures and in relation to existing inequalities. Finally, Chapter 8 brings together the findings in the light of the research questions posed in Chapter 3. In this final chapter I summarise how the data presented in this thesis has added to our current understanding of the use of online support and information in the wider caring practices of parents of people with rare syndromes.
21 Chapter 2. Fragmented understandings: the role of online support and information in the caring practices of parents of people with a rare syndrome
Skinner and Schaffer (2006, p. 16) noted how the “explosion of new knowledge and technologies stimulated by the Human Genome Project” and the increase in information accessible through the Internet “has resulted in countless Web sites devoted to expert and lay knowledge of specific genetic disorders and to advocacy and support groups formed around them.” The wider availability of such sources has been hailed by some sociologists as a positive development, empowering patients and carers (Nettleton et al., 2005). Thus online support has been considered as valuable to members of isolated (Davidson, 2008; Valentine and Skelton, 2008) and geographically dispersed groups (Saukko, 2009; Zaidman-Zait and Jamieson, 2007), for parents with high caring responsibilities and parents who also work full-time (Zaidman-Zait and Jamieson, 2007). Some commentators have argued that these sources may be particularly valuable to parents of people with rare syndromes. Zaidman-Zait and Jamieson (2007) highlighted the importance of the Internet for information about rare genetic syndromes, including details of treatment and behavioural modification strategies that may not be known by doctors and other health professionals consulted by parents. In terms of online peer support groups, they suggest that these might be particularly beneficial for parents of children with disabilities who may have limited access to offline social support and sources of information (Zaidman-Zait and Jamieson, 2007) Similarly Gundersen (2011) argued that parents of people with rare syndromes may encounter a lack of expertise among local health professionals. However, as is argued below, our current understanding of the role of online support and information in the caring practices of parents of people with a rare syndrome is fragmented, both methodologically and theoretically. As a result, it fails to take full account of the wider social context within which Internet use and health and caring practices occur. In particular it tends to ignore alternative sources of
22 support and information, the social differentiation of the use of the Internet and information in wider caring practices, and the existing knowledge and skills of parents. The first section of this chapter outlines arguments for researching the use of the Internet as it is embedded in everyday life. The second section describes how the use of the Internet continues to be socially differentiated and how much of the research into the everyday use of online information and support fails to take this into account, limiting the conclusions that can be drawn. The third section explores our current understanding of how online health and support seeking relates to everyday caring practices, highlighting the theoretical and methodological limitations of these findings. The final section describes how a more coherent methodological and theoretical approach could improve our understanding of the role of online support and information in the lives of parents of people with a rare syndrome. It is suggested that this could be achieved through the use of Bourdieu’s concepts of capitals, habitus and fields and the application of mixed methodology to explore use in a case study group of parents of adults and children with Rett syndrome. The following chapter explores Bourdieu’s concepts in more detail, outlining how they have been used in Internet research to date and how they will be applied in this thesis to explore the role of online support and information within this group of parents.
2.1 Use of the Internet and e-health in everyday life
As access to the Internet has increased in some parts of the world, theories about its place in society have developed and changed, reflecting, to a certain extent, its status as a banal part of everyday life (Hine, 2015). This has been reflected in a number of calls to treat the Internet and interactions online as embedded within everyday life, both within Internet studies and the sociology of health and illness.
23 2.1.1 The Internet in everyday life A number of scholars in Internet studies have suggested that researchers treat the Internet as part of everyday life. As will be seen below, this is associated with a focus on mundane use. This perspective avoids the polarised utopian and dystopian perspectives, which tend to suggest that access to the Internet is either democratising and transformational or that it harms social relationships. In an influential book Haythornthwaite and Wellman (2002) argued for a recognition of the ‘everyday’ nature of online activities in the ‘second age of the Internet’ (Haythornthwaite and Wellman, 2002, p. 4). They posited that this reflected a number of factors that had led to the greater embedding of the use of the Internet within everyday life. These were: increased access to the Internet; more time spent online; greater use at home; greater use for work outside working hours; greater use in education; a felt sense of needing to ‘keep up’ by being online; and a change to a ‘networked society’. As part of this work they critiqued research that explored the use of the Internet in and of itself, which they argued created a false dichotomy between the online and offline, such as studies of ‘online communities’. Instead they argued that our understanding of the Internet needs to be embedded in wider considerations of social connections, technologies and demographic characteristics, while remaining aware of the impact of not being online in a world where Internet use is becoming more embedded. This analysis was also alive to (then only just emerging) differences in the differentiation of how the Internet is used by those with access, such as time spent online, the purposes to which it is put, and how these might be socially differentiated and lead to further ‘digital divides’. However, as will be argued here, much research – particularly into online support groups – has continued to ignore the embeddedness of the use of such groups in everyday life. This strong propensity to treat the Internet as a separate realm has led to a number of reiterations of this argument. For instance, Baym (2009) echoed Haythornthwaite and Wellman (2002) in arguing for the importance of seeing the use of the Internet as a mundane, everyday part of human communication. She noted how many of the polarised ideas about the Internet reflected cultural concerns about technology and should be considered as part of this wider trend:
24 Most communication technologies throughout history have raised issues about the quality of interaction, the nature of community, the status of relationships, the authenticity of identity, the safety of children, and the limits of trust and privacy (Baym, 2009, p. 720).
Baym (2009) argued that research into individual sources of peer interaction (boards, newsgroups, chat rooms, social network sites) have provided much information about what happens within them, but that “we know next to nothing about how individuals and groups link these contexts to one another as they traverse the Internet” (Baym, 2009, p. 721). Instead, she argued, the use of such support should be understood as interwoven with offline activities and as part of an increasingly multimodal way of communicating with other people, and the underlying dynamics, not the medium of communication, should be the focus of research. As we shall see next, these concerns and this approach have been reflected in discussions about understanding the role of the Internet in modern health and caring practices.
2.1.2 Theories about the relationship of online information and support to everyday life Over the last decade, a small number of sociologists have argued that the use of online health information meshes with wider information and support seeking practices (Nettleton et al., 2004; Orgad, 2005; Wyatt et al., 2010; Ziebland, 2004). They have argued that research into online health practices tends to be based on decontextualised survey findings or qualitative descriptions of the experiences of active users of online peer support forums (Wyatt et al., 2010; Orgad, 2005), which, as will be described below, continues to be an issue in much of the literature today. The literature in this field has been dominated by a preoccupation with the impact of the status of lay health information online, shared through a range of online peer support sites, and the effects on lay-professional relationships. Nettleton
25 (2004), summarising a range of literature in the sociology of health and illness (e.g. Hardey, 2001; Webster, 2002), argued that we have moved from a period of ‘mechanical’ to ‘informational’ medicine, which has developed in concert with changes in technology. Citing Lash (2002), she argued that there is an ‘e-scape’ where “[t]he spaces, sites and locations of the production of medical knowledge are now more diffuse and are invariably mediated by means of digital technologies” (Nettleton, 2004, p. 673). In this e-scape, experiential, lay knowledge is presented alongside biomedical and commercial information, including sites, newsgroups and chat rooms managed by a range of institutions (charities, professional associations, commercial companies and pressure groups) and individuals. She argued that this impacted on how people manage illness, with a shift from doctors to ‘expert patients’ managing illness and the rise of evidence-based medicine, which has led to a more collaborative model of doctor-patient relationship. Ziebland (2004), drawing upon the work of Muir Gray (2002), discussed the role of the ‘expert patient’. She raised the possibility of whether “[o]ne of the consequences of the changing relationship between patients and doctors, a decline in trust and easier access to health information may be the emergence of a felt imperative to be (or present oneself as) an expert and critical patient, able to question one’s doctors and nurses and locate effective treatments for oneself” (Ziebland, 2004, p.1792). However, other commentators, at different times, have been more critical of the wider impact of the Internet on everyday health practices. Henwood and colleagues (2000) critiqued the depiction of the rise of the ‘informed patient’ (after Bury, 1997, similar to the 'expert patient' discussed above), which was thought to lead to a greater responsibility by patients to negotiate and consider treatment alternatives. They discussed how Giddens's (1991) work on patients as ‘reflexive consumers’ had been used by others to describe how the Internet is used in a positive way to empower patients (such as Hardey, 1999), but questioned whether this role was uncritically and automatically taken up by all patients. In a later paper, Henwood and colleagues (2003) argued that this was a form of technological determinism, where the mere presence of information online was assumed to increase empowerment. They presented empirical data in this paper demonstrating
26 that this ‘informed patient’ role was not adopted by all women seeking help relating to the symptoms of the menopause in their study. Nettleton and colleagues’ (2005) paper, cited above, summarised approaches to lay health information online as ‘celebratory’, ‘concerned and dangerous’ and ‘contingent.’ ‘Celebratory’ responses are broadly utopian, where lay expertise is valued, there is greater democracy and where there can be resistance to dominant medical practices, such as mass immunisation. ‘Concerned and dangerous’ perspectives come mostly, but not only, from the health literature, and can be concerned with either misinformation or increasing demand on services. In this perspective, non-health professionals using the Internet for health information are seen as lacking the ability to assess the credibility of information. The third, ‘contingent’ perspective was espoused by Nettleton and colleagues (2005) and drew together the views of others cited here, including Henwood and colleagues (2003) and Ziebland (2004). This perspective allowed that lay people can make informed decisions and argued that the other two perspectives are overstated. Nettleton and colleagues (2005) explicitly linked this to the ‘everyday use’ of the Internet perspective (e.g. Haythornthwaite and Wellman, 2002). The ‘contingent’ perspective allowed variation in the extent to which people want to be ‘empowered’, argued that use is enmeshed with alternative sources of support and supports an enriched relationship with professionals, which elsewhere they have argued is related to having a shared lexicon or frame of reference (Nettleton et al., 2004). However, these exhortations to consider the everyday, embedded use of the Internet have not always been heeded. For example, in an analysis of the conceptualisation of social networking sites (SNSs) in the clinical health literature, Koteyko and colleagues (2015) found that these papers continued to characterise online information as being inherently empowering or risky, echoing earlier technologically deterministic explanations. They reiterated calls for research to take “into account the diverse and multiple factors that shape health-related behaviour […] instead […] focusing on why, when and how these new technologies contribute to the everyday management of illness,” focusing on how they modify rather than revolutionise health practices (Koteyko et al., 2015, p.13). However, even in the social sciences, largely atheoretical lists of benefits, divorced from a wider social
27 context, continue to be published. For example, Ziebland and Wyke (2012), while highlighting the continuing lack of theoretical and methodological bases for researching the impact of online peer support sources on health outcomes, produced a comprehensive but ultimately rather dazzling list of potential benefits and harms, loosely presented under broad thematic headings. Although there was an acknowledgment of the tendency for this research to reproduce existing idealised or negative ideas about what online peer support could offer, the description of accounts of net use and associated fears and risks of harm were uncritically presented as examples of the impact of online peer support, with little attention paid to how these accounts might reproduce wider narratives about the Internet, such as the idea that “overengagement with online communities can be detrimental to life ‘off-line’”’ (Ziebland and Wyke, 2012, p. 240). In a break from discussions on lay health, Kivits has argued for the influence of other practices to be taken into account in understanding the use of the Internet in health. In 2009 she argued for the use of a mediated health perspective, which takes into account the everyday use of media, everyday health practices and everyday information seeking (Kivits, 2009). More recently she argued that the sociological perspective on e-health, in the era of Web 2.0, could enter a new phase where the role of technology is acknowledged alongside the embeddedness of online health experiences in everyday life (Kivits, 2013). This is an interesting aspect that is largely unexplored in the current sociological research, which does not tend to differentiate between different sources of peer support. This chimes with Seale's (2005) reminder to consider the impact of algorithms on searches online and the emergence of multidisciplinary work that seeks to avoid the sociological ‘black boxing’ of technical aspects of the web (Halford and Carrigan, 2014). As will be seen below, the consideration of aspects of technology – particularly the different mediums through which information is accessed online – has, as yet, been largely neglected in this field. However, there has been a much more significant blind spot in current research into the use of online support and information in everyday health practices. While scholars in Internet studies have emphasised the need to consider the continuing social differentiation of access to and use of the Internet
28 (Haythornthwaite and Wellman, 2002; Hine, 2015), this is rarely considered in discussions about the use of the Internet in everyday health practices. The next section presents evidence of social differentiation in Internet use in the UK and summarises what is currently known about its impact on the use of health and caring resources.
2.2 Everyday use – but not for everybody? The social differentiation of Internet and e-health use
As access to the Internet has increased in the UK and US, attention has turned from an original ‘digital divide’ (between those with and without access) to a focus on differentiated use in terms of how the Internet is accessed, the skills required, the experience of using the Internet and the kinds of technology used to access it. However, as will be demonstrated below, access to the Internet in the UK remains highly socially differentiated in terms of age, income and education. This section summarises current empirical research into the social differentiation of access to the Internet, use of the Internet more generally and use of the Internet specifically for health and caring purposes. As will be seen, there is strong evidence for continuing differentiation in terms of who is and is not online, their experiences of being online and their use of different online platforms. The evidence is weaker in terms of use of the Internet for health and caring information and support but still suggestive of social differentiation. It is therefore argued that any exploration of the use of online support and information should take into account the impact of differentiated use of the Internet and the potential differentiation of the use of online health and caring resources.
2.2.1 Social differentiation in use of the Internet
29 Access to the Internet The Oxford Internet Surveys (OxIS) run by the Oxford Internet Institute, have been measuring use of the Internet in the UK since 2003. They use multi-stage probability samples of 2000 UK residents, meaning their findings are generalisable to the UK population as a whole, although their response rates have dropped in recent years to around 50 per cent. Nonetheless, they remain the authoritative source of information about use of the Internet in the UK. The latest findings of the OxIS were collected in 2013, at the same time as the data presented in this thesis, so provide a particularly relevant context for this thesis. OxIS data shows that use in the UK population rose from 59 per cent in 2003 to 78 per cent in 2013. Among people who have never used the Internet or who have stopped using the Internet, the majority (91% and 71% respectively) do not intend to get online within the next year, meaning that there may be a group of people who will remain offline for at least the immediate future. Although the proportion of current users is high, this masks large disparities in use among some groups, where in some cases the majority remain offline. As a whole, therefore, Internet users in 2013 “remain[ed] disproportionately likely to be young, well educated and wealthy” (Dutton and Blank, 2013, p. 19). Older people are the most excluded, with half as many as in the general population – 39 per cent - using the Internet (Dutton and Blank, 2013). Despite gains in the lowest income group, household income still has a positive relationship with level of Internet use, where only 58 per cent of people in the less than £12,500 bracket used the Internet in the last OxIS, with use moving up to 88 per cent in the next earnings category (£12,500-£20,000), while use is almost ubiquitous among people earning over £40,000 (Dutton and Blank, 2013). Similarly, the difference between those who have no qualifications and all other groups is striking, with only 40% of people with no qualifications being online (this increases to 84% among people holding basic qualifications). The OxIS includes questions about reasons for giving up the Internet or not using it. Reasons for not using it include costs, skills, difficulties getting access and lack of interest. However, among people who have given up use of the Internet, the main reason is lack of interest, which is cited by 96 per cent of retired ex-users.
30 However, 67 per cent of retired people also cite that it is ‘not for people of my age.’ Although Dutton and Blank (2013) argued that this is analogous to a lack of interest, this seems more like a sense of exclusion than a choice, which is an aspect that will be explored in more detail in the following chapter in relation to social capital.
Differentiation in how the Internet is used As noted above, research has moved beyond explorations of the differentiation of access to the Internet into explorations of how use of the Internet may be differentiated among those with access. Since the turn of the millennium, there has been discussion of how, as access increases, use of the Internet may become socially differentiated. This is often termed ‘digital inequality.’ For example, in a much-cited and influential paper, DiMaggio and colleagues (2004) laid out a compelling argument for the development of differentiated access to the Internet among users. In this argument they drew upon pre-Internet conceptions relating to the social reproduction of existing inequalities: Bourdieu’s concept of cultural capital (Bourdieu and Passeron, 1977), as well as the “knowledge gap” hypothesis (Tichenor et al., 1970), where people of higher socioeconomic status can adopt new technologies earlier and, due to having higher education, can use new information from a range of sources more effectively. DiMaggio and colleagues (2004) highlighted five areas of inequality: technical apparatus, autonomy of use (which is related to ease of access aspects, such as location and monitoring of use), skill in using the Internet, availability of social support from more experienced users and variation in the purposes for which it is used. A similar argument was made by Hargittai (2008), who cited Bourdieu (1973) as an influence. She suggested that this greater ability to utilise the Internet would lead to the accrual of different forms of capital (financial, social, human and cultural), increasing existing inequalities. Hargittai (2008, p.943) also provided an interesting counter to the current discussions about digital inequality versus digital choice, arguing that “[w]hile it may be that some people opt out of ICT use based on an informed understanding of all that the Internet has to offer, much more likely is that people do not realize the many necessities and benefits of digital media.”
31 A number of studies have supported aspects of differentiation within DiMaggio and colleagues’ (2004) initial framework. In a review of surveys of American users from 2000 to 2008, Schradie (2011) provided a good overview of the multiple factors discussed in the literature that describe differences in how one uses the Internet. These include equipment, quality of online experience, frequency of use, location of use and cultural aspects related to class. More recent studies have investigated the links between social stratification and the level of digital skills. One example was a test carried out under experimental conditions by van Deursen and van Dijk (2010). This explored the social differentiation of skills related to using the Internet and finding information. They tested ‘operational’ skills (operating a web browser, using search engines and using Internet-based forms), ‘formal’ skills (navigating through hyperlinks, not becoming disorientated when navigating within and between sites), and content-related skills, which related to finding information and using the Internet in a goal-oriented way. They found that older people did not perform as well on tasks related to operational and formal Internet skills but did not differ in content-related skills. They also found that more educated people, with easier access to the Internet, had higher levels of all skills. However, they found no differences related to socioeconomic status or availability of specialist social support with online skills. It is possible that these differences were related to the type of software available in the lab, or to the task design, but they are interesting in terms of attempts to explain the mechanisms that might influence the quality of use. In the UK, a number of aspects of OxIS data support some of the contentions of DiMaggio and colleagues (2004) and Hargittai (2008). Firstly, those who use multiple devices to access the Internet use it in qualitatively different ways from others (Dutton and Blank, 2013). The OxIS identify such people as ‘next generation users’ (NGUs), defined by their use of a mobile phone plus two other devices to access the Internet (from a choice of tablets, readers or three or more computers) (Dutton and Blank, 2013). They argued that this kind of access makes the use of the Internet “more central to the life and work” of such individuals (Dutton and Blank, 2013). They are of interest here both because they use the Internet more for information seeking and for producing content and because 90 per cent of next generation users earn more than £40,000 per year, with the gap between users
32 widening over time. So while ‘next generation use’ is increasing dramatically (it moved from 47% in 2011 to 67% in 2013), so are the gaps between those who access the Internet in this way and those who do so in a less fluid way. This suggests the potential for an online inequality in terms of greater ‘everyday’ or ‘meshed’ use that can be traced back to inequalities that are likely to relate to ability to afford to buy multiple devices. Secondly, certain aspects of online skills and experience are related to economic position and occupation. For instance, the length of time someone has used the Internet and has had access at home is about three years higher among those who earn £30,000 than among those who earn less than £12,500 per year. Similarly there were strong relationships between use of the Internet at work, and occupation (Dutton and Blank, 2013), meaning that for some occupations, use of the Internet is something that can be developed as part of one’s job, while for others, this can only happen in other spheres. The relationship between occupation and Internet use was broadly related to occupation, with higher ranked occupations, requiring more education and experience associated with greater use of the Internet at work. However there was a slight anomaly among health professionals and people working in culture, media and sports, who were less likely to use the Internet at work than others closer to them on this scale. Thirdly, self-rated ability to use the Internet is much lower among retired people (49%) than among the general population as a whole (74%), perhaps reflecting the later adoption of use of the Internet among this group (Dutton and Blank, 2013). Fourthly, the use of the kinds of mediums used in peer online support was socially differentiated. Use of social networks, posting on a message board, participating in chat rooms, and reading and writing blogs were all found to increase with income and reduce with age (Dutton and Blank, 2013). However, this perspective has not been without its critics. Halford and Savage (2010) argued that Hargittai (2008) still positioned the Internet as a ‘neutral good’ and only explored how structure influenced its use in a deterministic way. They argue for a more nuanced understanding of the links between structural inequalities and Internet use. This is supported by Helsper's (2008) findings, which
33 established positive links between social disadvantage (based on an index including health, employment, income and education) and digital disadvantage (access, quality of access, attitudes towards the Internet and activities undertaken online). However, there were exceptions to these findings, meaning that some socially excluded groups could overcome digital exclusion. Age and having children appeared to be a factor in engagement among these groups, with some of those ‘unexpectedly engaged’ younger, with children at home, and some of those ‘unexpectedly disengaged’ older and without children at home. In fact, it could be argued that Dutton and Blank’s (2013) findings support this idea, in that the structural differences described above do not represent 100 per cent of users in each demographic category and they instead presented a model of the ‘Cultures of the Internet’, which were derived from a multivariate analysis of various attitudes to using the Internet (Dutton & Blank, 2013). This created four attitudinal continuums on which respondents varied: seeing the Internet as an enjoyable escape, as creating efficiency and saving time, as facilitating social contact, and as creating problems. These were used to create five different styles of interacting, although there is overlap between them – from those high on the first three aspects, who are generally positive about multiple uses of the Internet (e-Mersives), through to Adigitals, who see the Internet as mostly problematic. These styles of interacting tended to reflect “tendencies for different cultures to be associated with particular social and demographic characteristics, but they are far from deterministic” (Dutton and Blank, 2013, p. 7). Nonetheless, they do have some relationship with structural differences, most notably age differences, where e-Mersives are mostly aged under 24 while Adigitals tend to be over 45. Helsper (2012, p. 415) recently argued that ‘there is almost no theoretical work regarding the factors that make digital engagement successful in improving people’s everyday lives’. Similarly, Halford and Savage (2010, p. 937) have argued that attempts to analyse the connections between digital and social inequalities are “limited, even restrictive”. However I believe that it is possible to acknowledge both structural inequalities and also the ability to transcend these, as suggested by the evidence in this section. As I will argue in Chapter 3, these nuances can be accommodated by using Bourdieu’s concept of habitus (Bourdieu, 1984). This is often misinterpreted as being overly deterministic, but it allows for some social
34 movement (within constraints) where power and valuable convertible assets are determined by social context, or field, rather than being set by education or income (Bourdieu, 1998). The next section explores what is known about the social differentiation of the use of online information and support in relation to health and caring practices.
2.2.2 The social differentiation of online information and support seeking in caring and health practices There is still relatively little information available about the social differentiation of the use of online support and information, and particularly the use of online peer support, in wider health and caring practices. This section presents some of the strongest evidence in these fields, but as will be seen, the research is limited and differs across generic information and peer support sources.
Health and information seeking online: evidence of differentiated use and benefits The OxIS data provides some fairly compelling evidence of structural differences in both health information seeking online and the ability to accrue benefits from these activities, which are broadly supportive of the idea of the reproduction of existing inequalities through digital inequality. Use of the Internet for health information was relatively high – perhaps even a commonplace or ‘everyday’ use for some people, with sixty-nine per cent of Internet users having ever searched for health information online in 2013, down marginally from 71 per cent in 2011. Nearly twice as many next generation users (NGUs) agreed the Internet was an essential source of information (41%) when compared to first generation users (24%) and non and ex- users (1%), although it is hard to establish whether this belief drives use or vice versa. In terms of accruing unequal benefits online, 47 per cent of NGUs found information to improve their health, while only 30 per cent of first generation users and 10 per cent of ex-users had. Similarly, those in higher education were more able to realise benefits online such as saving money, finding out about an event, finding information to improve health and finding a job, which Dutton and Blank (2013) argued supported the concept of the ‘knowledge gap’ outlined above. 35 Social differentiation of use of the Internet for information among carers Currently, little is known about the use of the Internet among carers, neither in terms of access to the Internet nor use of the Internet for information or support related to caring. The best study of Internet use among carers is now ten years old (reported in Blackburn and Read, 2005; Blackburn et al., 2005; and Read and Blackburn, 2005). This was based on a survey of 3014 carers who were recruited from three county databases and a national charity database. It should be noted that this survey had a low response rate (40%), with male carers and carers younger than 30 years old likely to be underrepresented when data was compared with national statistics on carers. However, given the difficulties of identifying carers in the wider population, and the constraints on participation among this group, this is a reasonable source of information, although it may not be possible to generalise to all carers in the UK. Findings were that similar demographic differences in overall Internet use were present in this sample as in the rest of the population when compared with contemporary Office for National Statistics data (ONS, 2003, cited by Blackburn et al., 2005). Fifty per cent of respondents had ever used the Internet and there was lower use of the Internet among carers aged over 55, women, people not in paid employment and carers, people living in accommodation they did not own and – in a new finding – parents providing care for more than 20 hours per week. Among Internet users, Blackburn and Read (2005) reported that 72 per cent of parents who had ever used the Internet in their sample had used it to get ‘direct information related to caring’. However, this contradicts findings reported in Read and Blackburn (2005), which claimed that 52 per cent of carers had used the Internet to gain this kind of information. Different base figures are quoted, so it is difficult to assess which is the accurate figure and it was not possible to establish how the 52 per cent figure was calculated. Barriers to using the Internet included lack of time to go online to find information and to develop digital skills, reflecting some of the inequalities outlined above. In the same study, among carers given trial access to a PC with some training and support in using it, some parents noted a preference for using the telephone, which was felt to be less impersonal. Porter and Edirippulige (2007) carried out a large online survey on parents’ use of online information to support caring for children diagnosed with hearing loss
36 in Australia. Their focus, similar to mine here, was on social patterning and how this related to usage. This survey suffered from serious limitations in coverage of this sample group, again related to the lack of a central sampling frame. Letters were sent to 229 gatekeeper organisations and service providers who offer services to deaf children and their families and information was posted on five websites. They sent reminder letters to only 47 organisations and not to other organisations due to costs. 166 parents completed their survey. They found that parents with a university level education more frequently used the Internet when seeking information. Interestingly, increasing level of education was found to be associated with increased numbers stating that online information had ‘a major influence on their decision making’. They found that there was little difference between use every day or use every few months, but that 23 per cent of people with university degrees were more likely to use the Internet several times a week or a month compared with other groups. The remaining study that referred to potential social differentiation among parent-carers has been qualitative, so it is not possible to generalise at all from this data. Nevertheless, it provides evidence to support the above findings and is indicative of a potential digital inequality. In Skinner and Schaffer's (2006) qualitative study of parents of children with suspected genetic disorders, 83 of the hundred families had used the Internet in relation to their child’s diagnosis, with fewer from lower income and lower education families having done so. These findings, though limited, appear to reflect similar social differentiation of use of both the Internet and of the Internet for caring (or health) purposes, as found in the general population.
Social differentiation of online peer support sites and groups In a recent scoping review, Paterson and colleagues (2013) were unable to locate information about the social differentiation of the use of online social support among parents of children with chronic illnesses and disabilities. This information is certainly scarce and the remaining studies described in this section are methodologically limited, so cannot be generalised to a wider (admittedly hidden) population and are somewhat contradictory. 37 Blackburn and Read (2005, p.510) found that among carers who used the Internet, 36 per cent used it for ‘making direct contact with relevant organisations or individuals in similar circumstances.’ However, this conflates contact with carers by email with the use of online groups. It does not give any idea of how many carers read messages posted by other carers without making direct contact, or even of how many parents are contacting carers rather than organisations. No information was given about the social differentiation of these parents. Porter and Edirippulige (2007) found that parents with a university education were significantly more likely to participate in online support groups, but information about the perceived utility of these groups was not given. Leonard and colleagues (2004) surveyed users of RettNet, an email listserv for parents of people with Rett syndrome and others with an interest in the syndrome. This research explored use by parents only. It was limited in that it focused only on current users of this listserv, who may have differed from ex-users and parents who used other forms of information and support. Nonetheless, it provided a picture, though now dated, of current and probably regular users of this source. RettNet is run by the IRSF, a US organisation, so the majority of the 119 respondents were US-born, with only two respondents born in the UK. Although respondents had varying levels of education, over half held a degree and among those working, the majority were professionals. This suggests that, as in Porter and Edirippulige's (2007) findings, use was relatively high among professional groups and those with higher education qualifications. However, Leonard and colleagues (2004) found hours spent on RettNet were not related to the age of respondent or family member with Rett syndrome, education, work status, availability of assistance, adequacy of existing emotional support or child’s functioning level. Respondents who were not in employment, living in rural areas, who joined for emotional support or friendship or to share feelings were significantly more likely to spend longer on RettNet. Part-time workers, salespeople, paraprofessionals and those not employed rated its value significantly higher than professionals, managers and clerical workers, suggesting a (slightly unclear, but present) relationship between social status and perceived value – suggesting that this source was valued less by professionals than by other groups.
38 The rated utility of information on the group was also high among younger parents (this approached significance), while those who had joined to befriend other relatives or for emotional support were significantly more likely (p< .05) to find it helpful. This suggests a greater relevance for parents who may lack alternative sources of peer support. These findings, though limited, presented an interesting picture. On the one hand they suggested that more educated parents and professionals used online peer support than other groups (as they do with more generic information online and the Internet). However, on the other hand they suggested that older parents in professional, clerical or management roles valued the group less than other parents. It not possible to establish from this data whether this relates to the quality of information on this particular email list or to sources of online peer support overall, a distinction that is discussed in greater detail in the following section, which attempts to piece together what is known about online information and support seeking in everyday health and caring practices.
2.3 The role of online peer support and information in modern caring practices: the current state of the research
At the beginning of the chapter I outlined some of the possible benefits of the use of online support and information for parents of people with rare syndromes. Yet it is argued in this section that our understanding of the role of online support and information in the lives of this group remains fragmented, both methodologically and theoretically. Research is summarised in terms of key themes in the literature that have the potential to shed light on the role of online support and information in everyday caring and health practices and how these might be socially differentiated. This section concludes with a summary of the limitations of this body of research and the final section of this chapter outlines how this thesis aims to provide a more coherent and less fragmented picture.
39 2.3.1 The role of online lay information in everyday caring practices A number of studies have summarised the kinds of lay health information exchanged in online peer support forums for parents of people with rare syndromes and disabilities, but these have often been methodologically limited. Studies of posts on online peer support forums have shown that a range of topics are discussed on such forums, including making sense of diagnosis and what it means for prognosis, medical issues, child development, treatment, specialist equipment, services, policies, professionals, discrimination, stress, upcoming events, useful resources, and personal stories about experiences (Huws et al., 2001; Jones and Lewis, 2001). Posters also appear to collaborate to solve problems relating to everyday support and report a reduced sense of isolation (Huws et al., 2001). However, assuming these benefit all parents – or even all parents who use the Internet - is a form of technological determinism (after Henwood et al., 2003). Such observations cannot tell us whether such benefits are socially differentiated, experienced in the same way by parents who read but do not post or whether they have any impact on wider caring practices. Research that explores the use of particular boards or groups (through surveys or qualitative interviews) are similarly limited in terms of understanding the role of online peer support among all potential beneficiaries. Where these have been carried out they have – unsurprisingly - tended to find high levels of satisfaction with online support (Baum, 2004). Benefits include problem-focused support, emotional support, practical ideas (Baum, 2004), getting information, sharing experiences, venting emotions (Han and Belcher, 2001) a sense of being understood, feeling less isolated, being reassured that one’s feelings are normal, and support in making decisions (Baum, 2004; Han and Belcher, 2001). However, this kind of research has also highlighted the importance of particular kinds of information traded in such groups. For example, in their study of the RettNet email listserv group, Leonard and colleagues' (2004) respondents highlighted the particular importance of information about medication (84%), Rett syndrome research (79%), equipment (72.3%), symptoms of Rett syndrome (71.4%), physiotherapy, occupational therapy and speech therapy (68.9%), feeding and nutrition (66.4%), genetic issues (64.7%), school
40 (62.2%) and emotional support (62.2%). Sixty-nine per cent of respondents with children of school age indicated that RettNet helped them deal better with their child’s educational needs (particularly regarding relevant legislation). Eighty-three per cent reported that they felt the information was accurate. Seventy-one per cent noted that medical and practical information gleaned was of equal value. Disadvantages included the time involved (58%), repetition of topics (30.3%), misinformation (27.7%) and being offended (17.7%). Those who rated RettNet less favourably noted that it lacked relevance to people outside the US, the number of emails was excessive and subjects discussed were limited. As highlighted above, this particular source was read by more educated parents and those in professional occupations (at least among survey respondents), but was rated as most useful by non-professionals, younger parents and those who joined to befriend other parents. This may indicate that parents with access to alternative sources of information or support found this particular board less useful. However, this cannot be confirmed without more in-depth information about these factors. Overall, studies that have focused on the views of current users of particular forums (either by observing posts or surveying or interviewing users) reflect the views of the ‘converted’, rather than the wider views and practices of carers who have stopped using such sites or are unable or choose not to use them. They also cannot tell us how the use of such sources meshes with other sources of support and information. A handful of studies have explored the benefits of online information and support among wider caring populations. These have used qualitative research methods, mainly focusing on interviews and are summarised below. These are among the most valuable sources of information about the use of online peer support among parents of people with rare syndromes, but, as will be argued below, this body of research still has limitations. Lowe and colleagues (2009) analysed secondary accounts of interviews about pregnancy and antenatal screening. However as the interview did not specifically enquire about Internet use, this may not have captured the full range of women’s online experiences. Their findings supported many of the suspected potential benefits of the Internet for parents of children with rare syndromes described above,
41 particularly that the Internet provided access to additional information that went beyond what was offered by health professionals and in traditional sources of information, such as pregnancy books and resources. Similarly, Lowe and colleagues’ (2009) interviewees reported that reading about other parents’ experiences helped them feel less alone and helped them to judge their own emotional reactions, although this could have a positive or negative impact. Skinner and Schaffer’s (2006) and Schaffer and colleagues' (2007) papers were based on a wider ethnographic study of how parents of children suspected of having a genetic syndrome used, sought and interpreted information in their wider caring practices. Their data was based on the experiences of 100 of the 106 families they had recruited, who had used the Internet either directly or by proxy. Parents combined use of both scientific information and lay health information, with lay health information conceptualised by Schaffer and colleagues (2007) as a form of ‘case history’, to make sense of the meaning of the diagnosis in their child’s own life. In echoes of the findings related to understanding prognosis in online observation studies (Huws et al., 2001; Jones and Lewis, 2001) this involved trying to establish whether one’s child was likely to be a typical or milder case and to learn everyday strategies for managing their child’s development and health and overcoming challenges, for instance in behaviour management. Parents of children with rare syndromes, who reported that prognosis information from health professionals was inadequate, were particularly likely to seek this information (Skinner and Schaffer, 2006). These ‘online case histories’ were also used as ways of assessing the likely benefits of new and experimental treatments and to decide when to fight for a particular treatment that had been denied. Lowe and colleagues (2009) reported similar findings, with the Internet used to explore the meaning of diagnosis in relation to potential treatments and medical decisions. This use of online lay experience is redolent of a form of ‘apomediation’ described by Eysenbach (2008), where parents’ views are perceived as forms of review, much like consumer ratings, and as independent of vested interests. This searching out of treatments and information seen as affecting their child’s prognosis appeared to be very strongly felt as an obligation, reflecting earlier ideas about the ‘felt obligation’ of becoming an expert or informed patient (Rose, 2001, cited by Schaffer et al., 2007; Ziebland,
42 2004). Most recently, Gundersen (2011) presented interview data about the role of the Internet in adjusting to diagnosis among parents of people with a rare syndrome. As in other research presented above, parents initially used the Internet to try to understand the prognosis of the syndrome for their child, as diagnostic information was limited and rather broad in its scope. However, Gundersen (2011) also found evidence of some parents actively seeking information about possible diagnoses with one parent who secured a particular diagnosis as a result of carrying out her own research. In Skinner and Schaffer’s research (2006, p. 20), parents reported that when they were able to “demonstrate scientific literacy at the beginning of a clinic visit”, following research online, professionals provided more detailed accounts about conditions and their impact. This recalls Nettleton and colleagues’ (2004) finding that a shared lexicon improves lay-professional relationships. Similarly, in Gundersen’s (2011) research, parents’ realisation that their local health professionals knew little about their child’s syndrome led to them preparing research ahead of consultations to counterbalance an initial sense of a lack of power. Online support was used to explore alternatives to suggested treatment, with views sought from researchers, other clinicians and peers. This information was then used to support discussions with clinicians. For example, some parents reported that they had gained experimental treatment due to research presented by other parents as part of online advocacy networks (Skinner and Schaffer, 2006). There were hints of differentiation in how parents used the Internet in both studies, but these were not explicitly examined in relation to social differences or mechanisms. Skinner and Schaffer (2006) noted that most parents used the Internet as a supplementary source of information alongside support from health professionals, but that the Internet became a primary resource for parents who reported having inadequate information, having not had their concerns taken seriously. These included how parents used online information to gain power in medical negotiations and to assess the credibility of online resources. There were differences in what the Internet offered different parents, from it being an additional resource to it being used to campaign for further research and raise awareness. However, this was only discussed in relation to the first digital divide, not in
43 differences in how parents used the Internet as outlined above. Further limitations to this work are: that it was carried out in the US, where the care and health systems operate in a very different way; that all parents had children aged under 18, so were likely to be more engaged in using the Internet; and that online support and information was treated as a single entity, without exploration of how it might be used differentially across different sites by different parents.
2.3.2 Relationship of information and support seeking to current need Schaffer and colleagues (2007) described how parents’ use of the Internet was led by need, with some parents seeking diagnoses or challenging diagnoses with their own online research, using it for an intensive period following diagnosis to understand prognosis, or using it for making decisions about treatment options. Use appeared to reduce once they felt they had gained sufficient knowledge. However, about one in ten of the parents continued to stay online to keep abreast of research and become actively involved in online peer support and advocacy groups, posting advice and information. These parents, significantly for this study, tended to be parents of children with the most rare conditions, or those who searched for alternatives to suggested treatment plans (Skinner and Schaffer, 2006). This suggests that although there may have been a felt obligation to be an expert carer, this diminished over time for parents of children with less rare conditions or who may have had greater trust in their local health professionals.
2.3.3 Relationship to other sources of information and support Lowe and colleagues’ (2009) interviewees used a wide range of materials, including offline resources (such as support from charities, some of which were discovered online). This suggests the meshing of online and offline sources of support even in this situation, and the complementarity of online information. Similarly, Leonard and colleagues (2004) found that users of RettNet had mostly gained information from the organisation that hosted this email listserv, the IRSA (92%). Seventy-eight per cent used the Internet for support and 68 per cent used offline forms of information (books, videos and leaflets).
44 Gundersen’s (2011) interviewees included people who had sought similar information offline before they had Internet access. The kind of information sought over time mirrored that sought online in that it changed from being an intensive search for information about diagnosis and prognosis to being about treatment and support. Parents actively avoided contact with families with the same syndrome initially, as this was felt to be too difficult to face soon after the diagnosis. Gundersen (2011) also found suggestions in the data that the availability of offline support, through connections with specialist clinics, made online support contact unnecessary for some parents. In her study, the parents who made use of online support were the only two parents who had been denied access to such clinics. However, this research describes the experiences of parents within the Norwegian setting, where parents of children with rare syndromes are offered the opportunity through their health centre to use the services of medical centres specialising in specific rare syndromes. Although a specific clinic for Rett syndrome exists in the UK, access is not routinely offered through the NHS.
2.3.4 The reproduction of biomedical narratives and flight from online peer support sources Lowe and colleagues (2009) found that parents using the Internet for support after receiving a genetic diagnosis following antenatal screening did not challenge biomedical models, but used information from other parents to support them to understand the diagnosis, feel less isolated and make medical decisions. Jones and Lewis (2001) reported that the posts on a support group for parents of people with Down’s syndrome focused on a number of themes, including celebration for small achievements and seeing the child before the disability, which was seen as a counter-narrative to the pathological biomedical model, although present in offline interactions (e.g. Cunningham, 1996). Huws and colleagues (2001) noted that some discussions on an international discussion group about autism included searches for causes of autism and discussions of unconventional cures, although some parents were sceptical of such claims.
45 The two papers based on online observation reported the occurrence of conflicts online between posters, which had precipitated people leaving an online group (Han and Belcher, 2001; Jones and Lewis, 2001). This is another aspect of the use of online peer support that could be better understood through an exploration of how online and offline support interact and an examination of the interface between individual’s views and the views shared online at a micro level. This could be particularly important in terms of understanding the potential of online support groups and forums as places where more subversive ideas can – or cannot – be exchanged.
2.3.5 Limitations of findings Most of these studies did not explore the social differentiation of use (Lowe et al., 2009; Schaffer et al., 2007). Gundersen’s (2011) study was limited in its coverage of the social differentiation of Internet use among interviewees. She uncritically presented Hardey’s (1999) assertion, critiqued in the following section, that access to the Internet “democratises access to health and diagnostic information” (Gundersen, 2011, p.81). Although there was acknowledgment of differentiation by education level in preferences for sources of information and suggestions of variation in information-searching skills (unexplored) this was not examined in detail, due to the nature of the data gathered (qualitative, with a small sample of 10 parents). Explorations of the uses of online peer support sites either took a micro approach, exploring use of one particular site, or treated all online peer support sites as a single entity. This masks how use of these sites might change over time and either substitutes one site to stand for all sites or ignores subtle differences between different sites that might affect use, such as who uses them, the kinds of narratives they present and the type of information available. Each of these approaches presents only a partial view of the full role of online support and information and how it relates to existing sources of support, social differentiation and the existing expertise of parents.
46 A key issue with these studies is that they explored the use of online support and information only among parents of children with rare syndromes and disabilities. As outlined above, use of the Internet and digital skills reduce with age. Age may also be related to a greater possession of existing expertise and support. A differential use of online support in wider health practices by older people is suggested in other sociological health studies, where use was limited among patients with an average age of 55 (Wyatt et al., 2010), who preferred to use other sources of support. These differences may be particularly important in the use of online peer support sites, given the higher use of social networks overall by younger people (Dutton and Blank, 2013). Before concluding this section of the chapter, it is important to acknowledge that there is a large parallel debate about the nature and existence of ‘virtual communities’ (e.g. Nieckarz, 2005) that is not covered here due to space constraints. The important distinction to be made is that the approach taken here is analogous to conceptualisations of sites as potential forms of ‘community support’ that can only become communities if there is regular interaction, as outlined by Zhao and Elesh (2007). This is a helpful distinction as it allows differentiation between the kinds of support available to those who contribute actively to online support spaces and the kinds of support available to those who read without contributing, which, it is argued here, has been under-researched. In addition, as outlined above, my aim is to explore the place of online support and information as part of wider caring practices rather than focusing on the active, regular use of a single site or group.
47 2.4 Putting it all together: towards a coherent understanding of the role of online support and information in the caring practices of parents of people with a rare syndrome
Online support and information has been described as being particularly useful for parents of people with rare syndromes, whose local health professionals may lack the specialist information they require. Due to the rareness of the syndrome, such parents are unlikely to have peers living close to them with whom they can consult. Some rare syndromes, like Rett syndrome, are associated with high caring needs resulting from the serious health problems that people with this diagnosis experience and having a profound disability that severely affects communication. Such factors are likely to increase the possible isolation of parents of people with Rett syndrome. However, as argued in Section 2.1, health and sociological research has reflected wider, early research into the Internet by tending to present the use of online information and support as either dangerous - spreading misinformation and threatening the positions and authority of health professionals - or as inherently transformative, bringing democracy and resistance to prevailing power bases and biomedical explanations of illness. It has also been argued that part of this wider accessibility to information has transformed people into expert or informed patients, whose new-found expertise will create a more collaborative method of working while exacting a toll of greater responsibility on individuals for their own health and the health of their children. However, these stances have been critiqued as being too technologically deterministic and for uncritically assuming that all people are willing and able to take up the mantle of the expert patient. More recently there have been arguments to reconcile these extreme positions, where patients have been acknowledged to be variable in the degree to which they embrace empowerment and to use multiple forms of information and support. However, the initial binary positions are still presented in much health and some sociological research. Some papers still uncritically present lists of benefits available online without considering varying levels of engagement and uptake. Two criticisms of the current theoretical
48 positions remain: firstly the lack of engagement with the everyday aspects of technology; and secondly the continuing social differentiation of access to and use of the Internet. Section 2.2 presented recent findings on this continuing social differentiation. It outlined theories and factors related to the digital reproduction of social inequalities, such as experience, skills and use of mobile technologies. It was argued that structural inequalities should be assessed alongside differences in use at the micro level. The limited evidence available on the social differentiation of the use of health and caring information and support online suggests the existence of corresponding social differentiation in the use of the Internet, including among carers. However, the relationship between the use of online peer support and structural inequality is more complex, with greater use among professionals and more educated groups, but lower benefits experienced by such groups, although this is based on very limited evidence. Section 2.3 presented evidence relating to the use of online support and information in everyday caring practices. These suggested a range of potential benefits of lay health information in online peer support sites, although most of this research does not explore the social differentiation of the use of and benefits experienced by different social groups. Research using current users of specific online support groups was critiqued for presenting the views of the ‘converted’, while other research that treated all peer online support sites as essentially the same was criticised for not taking into account differences between sites, which may cater to different audiences or offer different kinds of information or support. While some parents appeared to use information online to challenge local health decisions, not all did and there were few clues as to the differences between these parents. Research has suggested that parents’ level of current need is related to the use of online support. However, while some parents appeared to feel the need to be expert carers, others did not. Again this was not explored in terms of social differentiation because the research was qualitative. There was also evidence of the use of multiple sources of support and information among some parents, including similar information seeking offline for parents who had not had online access at the time of their child’s diagnosis. There was also some suggestion that parents with offline
49 specialist peer support were less likely to engage with online peer support, but this again was anecdotal as it was observed in a qualitative sample. Finally, the evidence suggests that biomedical narratives are not challenged in online peer support sites, although children’s achievements were explored and there were conflicts between parents that led to some parents claiming to leave the site (in posts), although the nature of these conflicts were not explored. Three critical issues were identified with this literature. Firstly, almost all studies failed to explore how the use of online support and information might be socially differentiated. Secondly, a micro focus on individual groups or a blurring of multiple sites presents only a partial view of use and how this interacts with available sources of information. Finally a focus on parents of children with rare syndromes is misleading as parents of adults are likely to have differing levels of expertise, to use the Internet differently and to have access to a range of existing sources of support and information. The age factor was highlighted as being particularly important when exploring the benefits of online peer support, as these mediums tend to be used more by younger people, at least in the general population. These issues come from two sources, identified within the discussions above. Firstly, these studies tend to be methodologically fragmented, either only exploring posts online, exploring overall trends with little exploration of how these fit into everyday practices or focusing on everyday use with qualitative research that cannot explore the relationship with larger structural differentiation. Secondly, the research is theoretically eclectic and fails to explore how structural differences may influence and impact upon micro everyday practices. In this thesis I attempt to overcome this methodological and theoretical fragmentation in the following ways. Firstly, methodologically, by exploring the role of online support and information in a single case study group of parents of people with a rare syndrome, using a mixed methods approach that considers both structural differences and micro everyday use of multiple online sites and groups. Secondly, by using Bourdieu’s concepts of fields, habitus and capitals, I bring together structural and micro aspects of the use of online support and information in everyday caring practices, exploring how they interrelate.
50 The next chapter describes these concepts, outlines and critiques how they have been used in existing Internet research and presents the framework used to explore data in this thesis.
51 Chapter 3. Bourdieu and the use of online support and information in everyday caring practices
In Chapter 2 I argued that the Internet has become embedded in wider social practices, including health and caring practices. I proposed that research into the use of online support and information among parents of people with rare syndromes – particularly the use of online peer support – is still methodologically and theoretically fragmented. Although some studies explore the embeddedness of online support and information sources in everyday caring practices, the social differentiation of the use of the Internet in caring practices has been insufficiently explored from a sociological perspective. As I suggested in the previous chapter, research in this field lacks coherence in exploring how structural differences in the use of the Internet interrelate with the use of online caring information and support, particularly online peer support. In this chapter I outline how I will use Bourdieu’s concepts of capitals, fields and habitus to explore the use of online support and information among carers of people with a rare syndrome, Rett syndrome. In section 3.1 I outline how the concept of social capital has been used to explore the role of online and offline social networks, highlighting the relative neglect of Bourdieu’s conceptualisation. In section 3.2 I describe key relevant aspects of Bourdieu’s wider theory that are particularly pertinent for exploring the links between the social differentiation of Internet use and its use in everyday caring practices. In section 3.3 I summarise and critique how Bourdieu’s concepts are beginning to be applied to examinations of the use of online support and information and provide an argument for how they will be operationalised in this thesis. Finally, in section 3.4 I describe the limitations of research into this field to date and present my research questions, which aim to address these gaps.
52 3.1 Social capital online and offline and the neglect of Bourdieu’s conceptualisation
Field (2008) has argued convincingly that the current significance and understanding of social capital is based on work undertaken by Bourdieu (1986), Coleman (1988, 1994) and Putnam (2000, 2002). Although all three authors concur on the centrality of social ties, they take very different theoretical stances. Broadly speaking (because a full outline is beyond the scope of this chapter) the different depictions of social capital can be conceptualised in the following ways. Coleman (1988, 1994) argued that social capital lies within ties between people and is a resource that can be drawn upon within a closed community. This community will be embedded in wider social networks with a high level of trust and outstanding mutual obligations. Putnam's (1993, 2000, 2002) conceptualisation of social capital exists at a macro level and is measured through civic engagement. He argued that social capital develops from horizontal networks that lead to civic engagement and that it provides ‘public goods’ (benefits), accessible beyond the immediate network. In stark contrast to both, Bourdieu (1986) argued that social capital disproportionately benefits members of elite groups, leading to the reproduction of inequalities in society. Perhaps as a result of these diverse conceptualisations, social capital has become a rather muddy concept (Ferlander, 2007; Hawe and Shiell, 2000; Woolcock, 2001). Further research has built upon how social capital connections function and what they can offer people who are members of social capital networks. These are outlined here briefly as they are a useful way of exploring the benefits (or ‘goods’) accessible via social capital networks. Ferlander (2007) has provided a useful summary of these terms, which are reproduced from her original tables in Tables 3.1 and 3.2, below.
53 Table 3.1 Ties by formality and direction (Ferlander, 2007)
Level of formality and direction of ties Formal ties Informal ties Horizontal ties Voluntary associations Family, relatives, friends, neighbours and colleagues
Vertical ties The church, work hierarchies Criminal networks, clan and network ties between relations and street gangs citizens and civil servants Reproduced from Ferlander (2007, Table 1, p.117)
Table 3.2 Ties by strength and diversity (Ferlander, 2007)
Level of strength and diversity Strong ties Weak ties Bonding (horizontal) ties Close friends or immediate Members with similar interests family with similar social or social characteristics within characteristics, e.g. social voluntary associations class or religion
Bridging (horizontal) ties Close friends or immediate Acquaintances and members family with different social with different social characteristics, e.g. age, characteristics within voluntary gender or ethnicity associations
Linking (vertical) ties Close work colleagues with Distant colleagues with different hierarchical different hierarchical positions positions and ties between citizens and civil servants. Reproduced from Ferlander (2007, Table 2, p.118).
In Table 3.1, formal ties exist within settings such as voluntary associations. Informal ties are interactions that happen outside formal settings, although this, rather puzzlingly, includes colleagues. Horizontal ties are with peers while vertical ties exist
54 between the levels of a hierarchy (Coleman, 1990 and Putnam, 1993, cited by Ferlander, 2007). In Table 3.2, strong ties are “intimate… with immediate family and close friends… tend to be multi-stranded and regularly maintained”. Weak ties are “non-intimate… with acquaintances… tend to be single-stranded and maintained infrequently” (Ferlander, 2007, p.118). Bonding and bridging ties are ‘horizontal’. Bridging ties link those with different characteristics, working as a “sociological WD-40” according to Putnam (2000, p.23). This can “generate broader identities and reciprocity” (Putnam, 2000, p.23). Granovetter (1973) argued that bridging ties allow social mobility and increase social cohesion. One of Putnam’s (2000) main concerns is the supposed decline of bridging capital. By contrast, bonding social capital occurs within homogenous groups, cementing differences and creating out-groups (Putnam, 2000). Both bonding and bridging capital can occur within the same group (Putnam, 2000). Bourdieu’s (1986) conceptualisation of social capital appears to reflect bonding ties, between like people that tend to exclude others. Thus in online forums we might expect to see the clustering together of like individuals to the mutual benefit of members and exclusion of outsiders. The strength of ties is not made clear, but it is possible that a range of strong and weak ties could co-occur within an elite social setting, depending on the level of maintenance of each connection. Ferlander (2007, p.116) further suggested that social support is a key benefit of social capital and outlines four different forms this might take (after Cohen & Wills, 1985), which are used in this thesis as a way of exploring the ‘goods’ available through online peer support sites. These are: ‘informational support’ (problem- solving advice and information), ‘instrumental support’ (practical, such as chores or financial aid), ‘emotional support’ (providing empathy), and ‘companionship’ (spending time with someone). ‘Instrumental support’ could be seen as partly reflected within the concept of economic capital and will be conceptualised as such within this thesis. Bourdieu’s (1986) description of the benefits of social capital does not give precedence to ‘emotional support’ or to ‘companionship’, although these could be argued to be part of the work undertaken to maintain and build bonds. The concept of ‘emotional support’ is included here as it is one of the key benefits of
55 online peer support that was cited in research summarised in the previous chapter, while companionship will be explored within interview accounts. Bourdieu’s theory has historically been relatively neglected in terms of research into offline (Field, 2008) and online activities (Zhao and Elesh, 2007), despite the evidence of continuing social differentiation of Internet use. This is a situation that persists today, while Putnam's (1993, 2000, 2002) conceptualisation has dominated theoretical discussions of the use of both online and offline networks. The particular appeal of Putnam’s (2000) theory online, as well as reflecting its wider dominance offline (particularly in the American literature), may be because Putnam (2000) discussed the potential of the Internet for providing ‘virtual social capital’ (Putnam, 2000, pp.169-180). He noted that it was still too early to make definitive predictions about how online social capital might operate. However, he supported the view, prevalent at the time, that since online communication (then) lacked visual cues and sometimes allowed anonymity, that this was “in many respects an egalitarian” platform for communication that might lead to the flattening of offline hierarchies (Putnam, 2000, p.174). This was similar to the utopian perspective outlined in Chapter 2, which emphasised democratisation of knowledge. He also noted that the asynchronous nature of the Internet and this ability to “[liberate] our social ties from the constraints of time” might become one of its most significant impacts, while noting the barrier of socially differentiated access (Putnam, 2000, p.174). However, following research contemporary to his account, he also suggested that people may become more aggressive online and that this may lead to difficulties building trust. Citing Galston (1999), Putnam further argued that the combination of anonymity and fluidity in online interactions might breed ‘drive-by’ relationships and that “[i]f entry and exit are too easy, commitment, trustworthiness, and reciprocity will not develop.” (Putnam, 2000, p.177). Putnam (2000, p.178) also highlighted a working paper by van Alstyne and Brynjolfsson (1996) that suggested that the Internet fosters the development of membership of single-interest groups that are “homogenous, not in demographic terms, but in terms of interest and outlook” (Putnam, 2000, p.178). Therefore he also provided some support to the dystopian view that it would damage the quality of relationships.
56 Reflecting the muddiness of the use of social capital as a concept in the wider literature (Field, 2008), there is a body of research purporting to reflect Putnam’s (2000) views, which lacks this level of nuance. Instead it tends to position online social capital as an implied or stated threat to offline social capital, which is given a privileged position, perhaps reflecting wider social anxieties about technological changes in communication described by Baym (2009) in Chapter 2. In effect, such research positions these two mediums of access to social capital as distinct and antagonistic, rather than meshed and potentially complementary and crosscutting as argued in Chapter 2. Bourdieu did not describe how social capital (or any aspect of his wider theory) related to the use of the Internet, but I argue in the following two sections that his conceptualisation of social capital has great potential for examining the links between social differentiation of Internet use and the everyday use of the Internet in wider caring practices.
3.2 Bourdieu’s concepts of capitals, fields and habitus
Bourdieu’s concept of social capital is an integral part of his wider theory of how different forms of capital combine to enable elite groups to maintain their supremacy (Bourdieu, 1986). Given the focus here on the embedded nature of social practices, it seems fitting to describe social capital within the wider context of Bourdieu’s writing rather than artificially separating it from his wider work. The concept of habitus is central to Bourdieu’s work both in terms of how inequality tends to be perpetuated in the face of social changes like the widening of educational opportunities. It is particularly useful here as a way of connecting and exploring how structural differences in the use of the Internet may influence the everyday use of the Internet in the wider caring practices of parents of people with Rett syndrome. Habitus is a ‘disposition’ towards the world that is influenced by socialisation (Bourdieu, 1998, p.8). Habitus allows an interface between an individual’s history (personal and collective) and their actions, which, it is argued,
57 “tend to reproduce” existing social structures (Bourdieu and Wacquant, 1992, p.123). It is an important theoretical concept because it breaks down the classical subjective and objective, or micro and macro dichotomies to explain how social structures such as class derive from existing inequalities and tend to be perpetuated by processes of both socialisation and wider social interactions.
This system of dispositions – a present past that tends to perpetuate itself into the future by reactivation in similarly structured practices, an internal law through which the law of external necessities, irreducible to immediate constraints, is constantly exerted – is the principle of the continuity and regularity which objectivism sees in social practices without being able to account for it; and also of the regulated transformations that cannot be explained by the extrinsic, instantaneous determinisms of mechanistic sociologism or by the purely internal but equally instantaneous determination of spontaneist subjectivism. (Bourdieu, 1990, p. 54)
Habitus is not used by actors in a conscious sense, but sets a context within which certain ways of acting seem natural to the actor (Bourdieu, 1990). A common criticism that has been used to reject Bourdieu’s approach is the claim that he does not allow for the agency of social actors (e.g. Halford and Savage, 2010). Yet Bourdieu (1998, p. viii) has argued that agents are “eminently active and acting”, but act within constraints of which they may not be aware, instead perceiving ‘illusory freedom’. Additionally, as will be described below, fields, where struggles to gain symbolic capital (a kind of power) take place, allow for the challenging of power and the changing of power structures over time. Bourdieu argued that cultural and social capital are disguised forms of economic capital. (Bourdieu, 1986). Economic capital is anything that is “immediately and directly convertible into money and may be institutionalised in the form of property rights” (Bourdieu, 1986, p. 16). The concept of cultural capital was created as a way to explain the unequal educational achievement of children from different social classes (Bourdieu, 1986). Cultural capital can be ‘embodied’, representing knowledge and dispositions gained primarily through socialisation, can
58 include objects, including machines, or can be institutionalised, such as through educational qualifications, which privilege some forms of learning over others. It is acquired, often unconsciously, through the family and as it is disguised is often perceived by others as competence and is converted into symbolic capital as a form of authority (Bourdieu, 1986). Higher economic capital can be converted into greater cultural capital through a number of means, not only through paying for education and equipment, but also the availability of greater free time to acquire additional cultural capital due to an elongated period before offspring need to be financially independent. Linguistic capital is a type of cultural capital that relates to the competency of language use by an individual, gained through education or upbringing (Bourdieu and Wacquant, 1992). Some social spaces require a high level of linguistic capital that effectively excludes those who do not possess commensurate competence (Bourdieu and Wacquant, 1992). Support forums relating to rare syndromes and disabilities, which can share complex medical and genetic information, might therefore exclude parents without the requisite level of linguistic – or indeed cultural capital acquired through education. For instance, parents who hold qualifications involving some level of research expertise will possess a type of cultural capital that allows them to make sense of primary resources, such as some research papers. Social capital is “the aggregate of the actual or potential resources which are linked to possession of a durable network of more or less institutionalized relationships of mutual acquaintance and recognition – or in other words, to membership in a group” (Bourdieu, 1986, p.21). These function as connections that allow people to “obtain very unequal profits from virtually equivalent (economic or cultural) capital, depending on… [how much] they can mobilize by proxy the capital of a group” (Bourdieu, 1986, p.256). Therefore those with the most connections to people with the highest stocks of desired economic, cultural or symbolic power benefit the most. It is therefore in the interests of those who have high stocks of social or other capital to limit their association with others who do not possess commensurate volumes of relevant capital(s) or who do not have links to others who possess them (Bourdieu, 1986). Access to useful social capital is therefore limited to other members of a wider elite group who are connected through “mutual
59 acquaintance and recognition” (Bourdieu and Wacquant, 1992, p.119). Such groups can “[bring] together, in a seemingly fortuitous way, individuals as homogenous as possible” (Bourdieu, 1986, p.250), for instance in certain social settings. Access to groups and to their social capital is managed in a number of ways that are not deliberately employed but reflect the preferred social behaviours of that group. Manners, which include ‘bearing and pronunciation’, can indicate that one belongs to a group (Bourdieu and Wacquant, 1992). Reciprocity is important for building and maintaining social capital, with continual exchanges demonstrating that one fits into the group. These exchanges also have the effect of reproducing the group. There is a pressure to reciprocate, with “durable obligations subjectively felt” (Bourdieu, 1986, p. 52). A plenipotentiary who has the mandate to speak for all members, can expel members who are seen to discredit the group (Bourdieu, 1986). This concept presents a number of interesting possibilities for exploring the use of online peer support forums. As discussed in the previous chapter, there is evidence that social networking sites and other mediums used to gain peer support (discussion boards, chat rooms, Facebook) are socially differentiated, with greater use by younger and wealthier individuals (Dutton and Blank, 2013). This may both influence who is welcomed and supported within such groups (or expelled by the plenipotentiary, a role that could be played by a group administrator) and who does and does not benefit from membership of such groups. It will be remembered from Chapter 2 that there was some limited evidence that an online support group was considered as less useful among professional and older parents (Leonard et al., 2004), and that about two thirds of retired ex-users of the Internet argued that it was ‘not for people of my age.’ Using Bourdieu’s (1986) conceptualisation of social capital, these findings could be seen as examples of how certain online spaces may offer limited ‘goods’ to older parents. This could explain why younger parents rated RettNet as more beneficial than older parents (Leonard et al., 2004), given that they were more likely to be new parents and to have a relatively low base of knowledge related to caring for a child with Rett syndrome. Bourdieu (1998) describes how levels of different capitals influence how individuals are situated within a theoretical ‘social space’. In Distinction (Bourdieu, 1984) this is represented by a quadrant, with total capital (combining cultural and
60 economic capital) on the vertical axis and the combination of levels of economic and cultural capital represented within four quadrants (for instance, low economic capital and high cultural capital). One’s position in this social space is thus defined by the “two principles of differentiation… economic capital and cultural capital” (Bourdieu, 1998, p. 6). Onto this social space can be mapped different practices across choices made in terms of music, sport, food and politics. Their relation to particular classes and positions in the social space is peculiar to a particular time and place and can change. The important aspect is that they serve as a way of distinguishing oneself from others who hold a different social position. The closer one is to someone else here, the greater affinity they will feel. One’s position in this social space is thus influenced by a combination of one’s social position (class, which is relational) and one’s dispositions (habitus), which are expressed (distinguished) through one’s preferred practices:
To each class of positions there corresponds a class of habitus (or tastes) produced by the social conditioning associated with the corresponding condition and, through the mediation of the habitus and its generative capability, a systematic set of goods and properties, which are united by an affinity of style (Bourdieu, 1998, pp. 7–8)
The way (and whether) somebody uses the Internet, their use of particular sites and their use of devices might all be conceptualised as forms of practice that distinguish them from others, while partly reflecting structural differences. An important aspect of practices is expressed through taste (aesthetic, political and so on), which Bourdieu argued is related to cultural and economic capital, but which also has a generational element (Bourdieu, 1984). Thus, Dutton and Blank’s (2013) ‘Cultures of the Internet’ types could be conceptualised as examples of clusters of online practices that tend to distinguish, for example, younger from older users of the Internet. Each form of capital can be converted into other forms of capital. For example, social capital requires time, as does cultural capital, and both are more available to those who have greater economic capital and can pay others to perform services for
61 them. Learning to use equipment that will save time also requires an initial investment in time to learn and maybe to purchase equipment, which can also be made possible through having a certain level of economic capital. Having greater cultural capital also allows more yield from time (Bourdieu, 1986). As will be discussed in the following section, this has been connected to differences in the use of the Internet in terms of the development of skills and use of different technologies. Capital is deployed within different ‘fields’, which are areas of social activity that can be seen as analogous to a game, where there is a struggle to gain symbolic capital and there are ‘goods’ of value to the participant in the game (Bourdieu and Wacquant, 1992). However this competition is not always dependent on the conscious use of strategies (Bourdieu, 1993). In Bourdieu and Wacquant (1992), Bourdieu argues that in any field there is a dominant habitus, and a match between an individual’s habitus and the kinds of capital revered and held in this field helps a player to gain a high status or ‘symbolic capital’. In each field (and subfield), the importance of the forms of capital varies and can change over time. There are rules that are not made explicit in the same way as in a true game. The competition between players in this field produce what is at stake within this field. By participating, players demonstrate that they have doxa (belief) in the game, accepting that it is legitimate and worth the investment of their time and efforts (this is known as ‘illusio’). The way that players are able to operate depends on their position in the group. Participants ‘jockey’ for position by using and converting different forms of capital to gain advantage – i.e. to gain ‘symbolic capital’. However, players can also change the rules of the game if they can discredit the kinds of capital possessed by their opponents. Again Bourdieu emphasises the role of (constrained) agency, where agents are ‘bearers of capitals’ with “a propensity to orient themselves actively either toward the preservation of the distribution of capital or toward the subversion of this distribution.” (Bourdieu and Wacquant, 1992, p.108) – players may challenge the rules or play within them. In The Field of Cultural Production, Bourdieu (1993, p. 162) defines a field as “a separate social universe having its own laws of functioning independent of those of politics and the economy”. Each field has “its specific relations of force, its dominants and its
62 dominated… [and is] endowed with particular institutions and obeying specific laws” (Bourdieu, 1993, p. 163). A field is a social structure that, like habitus, is created by specific social conditions. Modern notions can become so widely accepted – becoming “constitutive of our cultural universe” that they are seen as ‘a given’ and used to interpret events outside the society that produced these notions (Bourdieu, 1993, p. 162). For example, historians of art and literature applying definitions of ‘the writer’ and ‘the artist’ retrospectively, which may not fit the practices of the time studied (Bourdieu, 1993, p. 162). These perceptions are so insidious that it is difficult to imagine a society where these things are not a given, but it is misleading to use modern yardsticks to judge past cultures. Each field within a particular socio- historical context has particular forms of struggle for symbolic capital. For instance, in the case of a writer in the literary field, these are related to whether one can be identified as a writer or not. Fields can be considered to exist “at different levels of aggregation”(Bourdieu and Wacquant, 1992, p.104). For example, the literary field can be divided into subfields such as the novel or the theatre, universities into departments, or the housing market into house builders or construction firms. Each of these subfields “has its own logic, rules and regularities” and each move from a wider field into a subfield is “a genuine qualitative leap” (Bourdieu and Wacquant, 1992, p.104), so while they are connected to the wider field, they can be seen to function as separate entities. As will be discussed in the next section, there is some debate in Internet research about whether or not the Internet should be considered to be a field or a subfield. Symbolic capital, which is “commonly called prestige, reputation, fame… is the form assumed by… [the] different forms of capital when they are perceived and recognised as legitimate” within a certain field (Bourdieu, 1991, p. 230), and will result in acquiring the goods that are available as a result of succeeding in this field. This thesis builds upon McKeever and Miller's (2004) research, which is instructive in terms of how Bourdieu’s work can be used to explore wider caring practices. They used Bourdieu’s work (Bourdieu and Wacquant, 1992b; Bourdieu, 1977, 1978, 1984, 1986, 1990, 1995) to explore how parents gained symbolic capital for their children with profound and severe physical and learning disabilities within the medical field (McKeever and Miller, 2004). They found that some parents were able to ‘jockey’ for
63 position within the medical field by borrowing the capital of more powerful others (e.g. other health professionals) in order to improve their and their child’s position. This research adds to McKeever and Miller’s (2004) work by exploring the role of online support within these wider caring practices and struggles for symbolic power. As will be recalled from Chapter 2, two pieces of research suggested that, through showing ‘scientific literacy’ and reading information gained online, parents were able to increase their power in the medical field (Gundersen, 2011; Skinner and Schaffer, 2006).
3.3 Bourdieu online
There is a tendency for some researchers to cite Bourdieu in passing, usually in relation to social capital, with no further exploration of how much his particular conceptualisation of social capital fits their data (e.g. van den Hooff et al., 2004). However, a number of papers in recent years have made serious attempts to integrate Bourdieu’s concepts into a framework to explore use of the Internet or online peer support. These studies have been critiqued below in relation to how they have operationalised Bourdieu’s concepts of capitals, habitus and fields. Some extensions to this work are suggested, which link the conceptualisations used here to the literature discussed in Chapter 2.
3.3.1 Reframing social differentiation online: the role of Bourdieu’s capitals A set of papers have used Bourdieu’s capitals to try to account for how online and wider social inequality might reproduce one another. However these papers are limited in their use of Bourdieu’s concepts, either theoretically or empirically. As I argue in this section, I believe the wider concepts outlined above can be combined to provide a more coherent theoretical and methodological approach to exploring social differentiation in this research. As outlined in Chapter 2, some commentators have linked Bourdieu’s capitals with digital inequality. This research is recapped here, with a little more detail about their use of Bourdieu’s work. DiMaggio and colleagues (2004) noted that
64 conceptualisations of inequalities online could be understood in terms of access to cultural capital (Bourdieu and Passeron, 1977), the development of cultural distinction among those with fewer economic resources (Bourdieu, 1984) and the concept of ‘overselection’ in making early adopters unrepresentative (Bourdieu and Passeron, 1977). They suggested that this, along with the “knowledge gap” hypothesis (Tichenor et al., 1970), could explain inequalities in terms of technical apparatus, autonomy of use (ease of access), online skills and support from experienced users (social capital). Hargittai (2008) noted the potential of using Bourdieu's (1973) conceptualisation of cultural capital as a way of interpreting the link between parental education and the ‘Internet savvy’ of young people found in an earlier piece of research (Hargittai, 2007). However this was not developed explicitly in later papers, although the influence of this concept is clear. For instance, in Hargittai and Hinnant (2008) and Zillien and Hargittai (2009) it was found that people from higher socioeconomic backgrounds used the Internet more for what they termed ‘capital-building activities’, including accessing information about saving money and improving health. Although there is not an explicit link with Bourdieu’s capitals, this remains an interesting interpretation, which could be considered to reflect the economic, cultural and social capital gains made through online connections by different groups of parents. This work therefore informs the use of capitals in this research. Zhao and Elesh (2007) argued that Bourdieu’s (1986) concepts of social, cultural and economic capitals (with an emphasis on social capital) provide the best framework for exploring inequalities in access to social capital online. They suggested that Bourdieu’s (1986) description of social capital as something available to homogenous groups (linked to the concept of bonding ties here) provides an accurate conceptualisation of the social stratification of the Internet. They also suggested that the ability to convert one form of capital into another can help more privileged groups to gain greater benefits from the Internet. However, like the other papers cited here, they failed to explore the wider potential of Bourdieu’s work (particularly the role of habitus and fields) in understanding the role of capitals in the use of the Internet.
65 Drawing on digital inequality data, Helsper (2008) argued that capitals should be used as a way to conceptualise exclusion, although the model used was based on later conceptualisations of Bourdieu’s (1986) work, which add additional capitals (political, civic and personal) to his framework. These ideas were further developed in a communications paper that attempted to bring together a number of interdisciplinary concepts (Helsper, 2012). Here she proposed a model that depicted a two-way relationship between digital and more general social exclusion. This drew on the work of Wellman and colleagues (2002), which suggested that online and offline life and connections were integrated. Helsper’s (2008) description of social resources referred to the social capital theories of Coleman (1990) and Putnam (1995) but not to Bourdieu’s conceptualisation. Her adoption of a definition of cultural capital as ‘the shared norms that guide behaviour within a group’ (Durieux, 2003, summarised by Helsper, 2008, p.20) seems closer to Bourdieu’s conceptualisation of habitus and although Bourdieu’s concept of fields is alluded to, its operationalisation (into economic, social, cultural and personal) actually appears closer to his concept of capitals. Therefore it lacked specificity because while it used some aspects of Bourdieu’s capitals, it neglected or misinterpreted others and integrated elements of different – and I believe, irreconcilable - conceptualisations and approaches. The key relevance of this paper is therefore in how it suggested that cultural and economic capital and social connections can accrue across online and offline settings. As such, it relates to a later discussion about the Internet being a subfield of wider offline fields, although this idea is not explored in Helsper’s (2008, 2012) papers. North and colleagues (2008) used case studies to argue that cultural capital gained through socialisation influenced the tastes and habitus of teenagers in terms of how they used the Internet. This account was instructive in this research as it drew more broadly on Bourdieu’s concepts of habitus and tastes to explore how the Internet is used as a practice in everyday life. A number of writers have discussed the possible merits of Bourdieu’s concept of technical capital in conceptualising online skills (Brock et al., 2010; Gilbert, 2010; Halford and Savage, 2010; Zhang, 2010). This was described in The Social Structures of the Economy (Bourdieu, 2002) in relation to skilled manual labour (for example,
66 building skills). However I disagree with these writers that it is necessary to use this concept. Firstly, it refers to a form of cultural capital that is specific to technical, non- academic skills, such as building (Bourdieu, 2002). I believe it can therefore offer little in analysing the unequal social differentiation of online skills, which are related to a different set of skills, different forms of cultural capital and proliferate among wealthier groups. Secondly, as I argue in the final section of this chapter, these variations can be explained adequately through the concepts outlined in the previous section, specifically habitus, economic, cultural and social capital and their conversion into goods and symbolic capital in different fields. There are a number of limitations in terms of how the concepts of social, cultural and economic capital are operationalised in these studies. Some of these papers are theoretical and do not include empirical attempts to assess the theories put forward. As outlined above, some misinterpret Bourdieu’s concepts or muddy them with conflicting theories. Finally, in most cases the concept of capitals is used in isolation, without making reference to other useful concepts such as habitus and fields. As demonstrated in section 3.2, Bourdieu’s concepts of capitals are integral to his wider theory, with the implications of his social capital concept (Bourdieu, 1986) markedly different from those proposed by Coleman (1988, 1994) and Putnam (1993, 2000, 2002). However, there is also great potential in these studies for how the concepts of cultural, economic and social capital might be used to draw together the disparate explanations of social digital divides into a single coherent framework. For example, the purchasing of devices that allow easier and more frequent access to online support spaces for ‘next generation users’ (Dutton and Blank, 2013) could be conceptualised as a Bourdieusian conversion of economic capital, via cultural capital, into social capital. Similarly, the digital skills described by van Deursen and van Dijk (2010) (summarised in Chapter 2) could be interpreted as forms of cultural capital acquired by professional groups that increase the availability of total social capital resources available to them. The ability to free up time by the use of economic capital (Bourdieu, 1986) may also mean wealthier groups can spend longer building social capital online and learning new skills in using digital technologies. All of these advantages, if explored at both a micro and macro level, could provide explanations
67 for how the use of different forms of online support and information may confer wider advantages on some groups over others. Possession of cultural capital, in the form of education, may help to explain why the use of online support and information appears to provide greater benefits to more educated people, as discussed in Chapter 2. Among carers this could include the ability to read and assess some primary research independently. This ability to explore these primary sources may make the use of online peer support sites less valuable., which may explain Leonard and colleagues (2004) findings about the lower value ascribed to an online support group by professional and older parents. The possession of particular ‘goods’ in the form of knowledge and expertise, and the age makeup of online support groups may influence the use of such groups by older parents in particular, who are also likely to have less developed Internet skills than younger groups (Dutton and Blank, 2013). A key difficulty, which is not discussed in detail in the studies mentioned above, is how to understand the nature of online peer support sites in relation to social capital. As noted in the previous chapter, following Zhao and Elesh (2007), a distinction is made in this thesis between the benefits available to people who post on forums and those who read forums without contributing. Zhao and Elesh (2007) also argued that online support spaces may comprise professional or other homogenous groupings or require evidence of one’s legitimate membership in such a group through an administrator. However, this may be more difficult to establish among parents of people with Rett syndrome and parent gatekeepers of Facebook Groups may not have the time to verify whether somebody fits within the membership criteria outlined in the Group description. Bourdieu’s (1986) concept of social capital therefore needs developing when exploring the kinds of capitals needed to gain useful ‘goods’ in an online peer support site or group. Drawing upon the previous section, such goods might include evidence about treatment to take to one’s doctor to gain greater symbolic power in negotiations, a strategy to deal with everyday caring difficulties or information about a grant for house adaptations. In the case of parents who are members of a group but do not post, the goods available will be restricted to what is being discussed within a group or site, or what is searchable, in mediums where this is possible. It will effectively be the same
68 as finding information on static websites (and therefore analogous to finding information from offline sources too). Although it would be possible, if one can physically access the online support space, to gain useful information (informational support), it is not clear how emotional support or companionship support expressed between contributing parents might help those who do not actively contribute to a forum. It is conceivable that isolated parents who are caring for a daughter or son with the same rare syndrome might draw some kind of reassurance from reading the accounts of other parents who are in similar circumstances and facing the same difficulties, although the quality of this sense of support may well be different. However, there are ways that information might be restricted for those who do not post. Firstly, reading posts on any kind of site (or indeed any kind of information, online or offline) may be limited to those possessing a certain level of linguistic capital. Sites of interest to parents of people with Rett syndrome are likely to contain at least some technical jargon (relating to genetics, medical terminology or specialist treatments or resources). Secondly, as noted by Zhao and Elesh (2007), there may be some control over membership and sanctions for not participating, particularly where there are large groups with bounded membership that is visible to all members (for example, in a private Facebook Group, where membership has to be granted and all other members can see who else is part of the group and potentially not contributing). However, as noted above, this may not be policed when groups are run by parents rather than professionals, due to a lack of time. Thirdly, lack of knowledge with regard to understanding how to use a forum (or low online skills) or a lack of time to learn that cannot be freed up by the use of economic capital may provide another barrier that might lead people to read without contributing. For parents who post, there is the possibility of asking other members of the group for specific advice. However, for those posting within a group, there may be symbolic struggles to prove oneself a worthy member of the group, a need to meet certain obligations (perhaps relating to making exchanges of useful information) and the possibility of becoming involved in a symbolic struggle. Each form of social capital described above has built-in sanctions against people acquiring the benefits of social capital without contributing to the group through building a reputation,
69 being a visible member of an activity or through exchange. However, this is difficult to police online, particularly in public sites and groups that can be viewed without a membership requirement and even in large membership-only groups with shifting active membership. This problem is likely to increase with the growing ability to monitor sites through RSS feeds accessed through third-party software or applications. Wasko and Faraj's (2005) research on why people chose to post on a technical support forum when they knew others could ‘freeload’ is enlightening here because it showed that people would post if they felt it improved their professional reputation, if they felt they had something worthwhile to contribute and if they were central players in the active network of contributors and had connections to many others in that network. This is consistent with the idea of ‘community support’ as outlined above in Zhao and Elesh’s (2007) research, where the central, active group may experience some form of ‘community’ but where those who do not contribute can experience some form of freely available community support. However, this is problematic in terms of Bourdieu’s conceptualisation of social capital, because it means that people with lower levels of important capitals in the online subfield will be able to benefit from others’ expertise, rather than it being used to benefit only those who hold commensurate capitals or useful ‘goods’.
3.3.2 Habitus and use of the Internet Robinson (2009) used habitus and Bourdieu’s concept of skholè to explore socially differentiated uses of the Internet among teenagers at an American school. Skholè refers to the ability to ‘play seriously’ among French academics in terms of spending time reflecting upon ideas that others cannot due to time constraints (Bourdieu, 1998). Robinson (2009) used this to explain the difference between the use of the Internet between teenagers with low quality and limited access (task-oriented: “a taste for the necessary”) and those with high, easy access (less targeted: “playing seriously”). In test of use of search engines to find particular information, the less task-oriented students performed more successful and sophisticated searches, cross- referencing multiple sources and running several searches at once. She connected this theoretically to conversions of economic capital into higher quality access and
70 time to spend developing relevant cultural capital, which I believe make the same point in a more economical way without needing to draw from Bourdieu’s wider theory in relation to academia. These ideas were further developed in Robinson (2011) where although she made no further explicit reference to Bourdieu’s work, it is clearly influential in concepts such as ‘information capital’. As with the Helsper (2012) paper outlined earlier, Robinson (2011) also acknowledged the embeddedness of the Internet in wider practices, this time by acknowledging the range of available online and offline sources of information used by her participants. Lewis (2006) compared the use of the Internet for health by students and by teenagers using a charity for people who are homeless or in need of support. She demonstrated that while both groups used the Internet to seek health information, their approaches to health related to wider social experiences where health ‘choices’ were framed by a different set of social and cultural experiences. This reflected differences in perceptions of certain behaviours such as smoking and perceptions of control over health, where a more fatalistic approach was taken by the less privileged teenagers. She argued convincingly that this reflects ‘health habitus’, which calls into question the universality of the reflexive, individually responsible individual described by Beck (1992). This approach, although not explicitly discussed in Chapter 2, has informed notions of the ‘informed’ or ‘expert’ patient described there and connects to Giddens’ (1991) work on patients as ‘reflexive consumers’ (Lewis, 2006). Lewis (2006) suggested that the reflexive individual described by Beck (1992) may more accurately reflect the bourgeois or middle class experience. This recalls the findings of Henwood and colleagues (2003) discussed in Chapter 2, where women seeking advice on hormone replacement therapy (HRT) varied in their willingness to research information online and found it difficult to challenge health professionals when they did find contradictory information. This is suggestive of a possible age-related difference in ‘health habitus’ where lay-professional relationships were concerned, although there may be socioeconomic differences in information seeking that were not explored. Hale (2013) used a secondary data analysis of a health survey to explore the connections between socioeconomic groups, Internet access quality, and online and offline health behaviours. He used Bourdieu's (1990) concept of habitus to explore
71 how differentiated use of the Internet and health behaviours linked to ‘online health behaviour’, a broad category bringing together rather disparate aspects of use of the Internet for health (to buy medicines or vitamins online, to take part in online peer support, to use the Internet or email to contact a doctor, to track diet or exercise, to keep abreast of personal health information, such as test results). He found links between offline and online health behaviours, suggesting an overarching habitus in relation to health and that a higher level of education was associated with more online health behaviours. Wealthier people scored more highly on a composite measure combining confidence in finding health information (offline) and trust in using online health information. Although the measure for online health behaviours was a little broad and data was gathered before the greater use of ‘next generation’ mobile devices, this hints at the possibility of a connection between online and offline practices in information and health that influence the use of the Internet for health information. Meyen and colleagues (2010) used qualitative interviews to explore how aspects of habitus were reflected in use of the Internet overall and how the Internet was used to build or maintain cultural capital (which they described as knowledge, particularly relating to one’s career) and social capital. They created a typology that took into account these aspects as well as demographic characteristics. They found that age was related to online habitus through ‘Internet socialisation’, reflecting whether people had grown up using the Internet. They also argued that professional groups, or those striving for such positions, tended to use the Internet more to develop supportive cultural and social capital. However, although they argued convincingly that qualitative research is required to explore how use of the Internet reflects wider habitus, the use of qualitative research alone limits the strength and applicability of their conclusions relating to social position.
This research demonstrates the utility of habitus as a concept to capture how online health and caring practices may reflect wider habitus in information seeking and health practices. It also provides a way of conceptualising how, at a micro level, use of the Internet is used differentially both for different purposes and in terms of the use of technology and frequency of use. These papers also demonstrate how it is
72 possible to explore habitus both from quantitative and qualitative perspectives, using attitudinal measures and interview data respectively. As will be argued below, I believe an exploration of habitus and its links to wider structural inequalities can only be achieved through using a mixed methods approach, which combines the benefits of both approaches taken in the studies cited above.
3.3.3 Meshing the online and offline: conceptualising online sites and groups as subfields Bourdieu did not specifically tackle the use of the Internet in his writing. This means that he did not explore the status of the Internet in relation to fields. Although the Internet has recently been conceptualised as a field, within the rather specific example of meme production (see Julien, 2014), the approach taken here is consistent with Sterne's (2003) argument that the treatment of technology should reflect Bourdieu’s use of the camera and television within his work “[a]s part of the habitus, [where] technologies and their techniques become ways of experiencing and negotiating fields” (Sterne, 2003, p.385). Sterne (2003) argued that technology, including the Internet, should not be seen as separate from society, but as part of society. Treating the Internet as a subfield is thus consistent with the findings reported so far, which have emphasised the mundane, everyday use of the Internet as part of everyday practices (e.g. Haythornthwaite and Wellman, 2002; Hine, 2015) and suggested that the use of online support and information should be understood within wider health, caring and social practices. In line with this argument, a number of researchers have conceptualised online support spaces and sites as subfields that operate within wider social fields. Smith and Stewart (2012) explored the wider bodybuilding field through posts on the subfield of an online muscle enhancement forum, providing a detailed description of the power hierarchies and currencies of influence used within them. They outlined examples of the use of economic capital (ability to buy machines and drugs to achieve symbolic capital), field-specific cultural capital (knowledge about steroids, training methods and willingness to go to extremes), and social capital (regular posting and support for each other’s efforts) as ways of improving one’s social
73 position within the subfield. A key limitation of the above study is that they focused solely on online posts. This does not allow a systematic exploration of how the possession of existing offline capital can influence support available in different online support spaces for different people. Those who are effectively excluded from accessing or participating in some online spaces by not having the appropriate capital or habitus are not represented in such research. Finally, an understanding of how narratives relate to fields can help to conceptualise the role of habitus in distinguishing different online subfields. In their research on blogs about Black womanhood, Brock and colleagues (2010) highlighted how blog comments allowed people to challenge and perhaps influence privileged narratives. This could be conceptualised as a symbolic capital struggle within an online subfield, where the boundaries of accepted discourse and therefore ‘rules of the game’ in that subfield, are challenged. Frank (2014) argued that the dominant illness narrative used in a medical subfield reflects the dominant habitus in the wider field. Thus narratives used in certain online support spaces may suggest the influence of a particular offline field, for example in the use of biomedical narratives within an online support forum, as found in Lowe and colleagues (2009). Through this such narratives could provide a clue to the habitus of this subfield, whether parents’ own habitus fits or does not fit with this particular habitus and how this impacts on use of this particular site or group. Taken together, these studies suggest three conceptual approaches to exploring the use of online peer support sites in wider caring practices. Firstly, it is possible to conceptualise the conflicts that occur on online support forums as examples of struggles for symbolic power. Secondly that it is possible to assess individual habitus fit with an online subfield through the perceived narratives on that subfield. Thirdly, that it is possible to explore how online subfields relate to offline subfields, such as charities, medicine and genetics, through the ‘goods’ and voices represented there.
74 3.4 Reframing the use of online support and information in the everyday caring practices of parents of people with Rett syndrome
This final section highlights the gaps in the literature that I aimed to address in this thesis and concludes with my four research questions. The following chapters describe how the research was carried out and present the results in the light of the literature discussed in these preliminary chapters. Throughout this and the previous chapter, a number of limitations and gaps were identified in the literature. These are summarised next in order to provide a context for the contribution of this thesis and to frame the use of Bourdieu’s theory to provide a coherent approach that addresses these limitations. As argued in Chapter 2, research into the use of online support and information among parents of people with rare syndromes remains methodologically and theoretically fragmented. This is particularly true with regard to the role of online peer support, the social differentiation of this form of online lay support and its use among older parents. This is partly due to the use of either quantitative or qualitative research approaches, which can only provide a partial picture of either social differentiation or micro practices. This research is also limited in that it tends either to conflate all forms of online peer support together or to focus on use of a single forum, neither of which can provide an illuminating view of use of multiple online sources within wider caring practices. As a result research into this field is theoretically limited in exploring the interplay between structural differences in the use of the Internet and the use of online information and support in everyday caring practices, particularly the role of online peer support. Research into rare syndromes has tended to look at less rare syndromes where parents will already hold knowledge (e.g. Down’s syndrome) or a range of rare syndromes that are likely to differ in terms of care needs. This chapter has explored the use – and neglect – of Bourdieu’s concepts of social, cultural and economic capital, habitus and fields in Internet research. This use
75 has also been rather fragmented, with the employment of only one or two concepts and few studies that attempt to use these concepts in a more integrated way, as outlined in the previous section. The use of these concepts is very rare in research into the use of health practices. As far as I am aware no research has used these concepts – either singly or together - to explore the role of online information and support in the everyday caring practices of people with rare syndromes or disabilities. This research employed a mixed method approach to explore the role of online support and information in the wider caring practices of parents of adults and children with Rett syndrome. The research questions were as follows.
1. Are younger, wealthier and more educated parents of people with Rett syndrome more likely to use online support and information than others? 2. Are different platforms for online peer support socially differentiated so that like parents of people with Rett syndrome are brought together ‘in a seemingly fortuitous way’?7 3. How does an individual’s habitus and possession of different forms of relevant cultural and social capital affect their use of caring-related online support and information? 4. How does the use of online peer support sites influence wider caring practices? Is there any evidence of differentiation of benefits by age, income or education?
The next chapter outlines how these research questions were approached, describing research design and analysis procedures.
7 After Bourdieu (1986, p.22).
76 Chapter 4. Methodology
As I argued in the previous two chapters, research into the role of online support and information in the everyday caring practices of people with a rare syndrome is methodologically and theoretically fragmented. This fragmentation broadly reflects wider theoretical and epistemological orientations that tend either to prioritise the importance of macro, structural differences and downgrade micro explorations of everyday interactions or vice versa. This can only provide a partial picture, which is limited in exploring how online information and support are used in everyday caring practices while acknowledging the likely social differentiation of online and wider practices. In Chapter 3, I proposed a new way of researching this problem, which has three key components, described in detail in this chapter. Firstly, I focused on a case study group of parents of people with a particular rare syndrome (Rett syndrome, described in Chapter 1). Secondly, I used Bourdieu’s concepts of social, cultural and economic capital, habitus and fields and subfields to explore how structural differentiation interacts with micro processes. Thirdly, as described in this chapter, I used both qualitative and quantitative methods in a mixed methods approach. Section 4.1 of this chapter describes and justifies the overall research design and use of a mixed methodology to explore the research questions presented at the end of Chapter 3. Section 4.2 describes the survey element of this research, beginning with the hypotheses to be tested, describing the development of the survey and choice of measures, piloting, recruitment and nature of the sample drawn. Section 4.3 describes the qualitative element, which included both interviews and use of records detailing visits to online peer support sites and groups. This section includes description of the research tools used, and recruitment and key characteristics of the interviewee sample. Section 4.4 describes how quantitative and qualitative data was analysed and combined. The chapter ends with a summary of how this approach was able to yield new insights into the role of online support and information among carers of people diagnosed with a rare syndrome. These insights are presented in the remainder of chapters in this thesis.
77 4.1 Research design
As stated above, my aim was to explore whether there was social differentiation in the use of online support and information and how this related to wider caring practices. I was particularly interested in how the use of online support and information might be differentiated in terms of income, education and age. In other words, I was interested in the links between agency and structure, as outlined in Bourdieu’s concepts of social, cultural and economic capital, habitus and fields. In deciding how to approach this research, I was informed by Bourdieu’s own attitude towards methodology, in that he argued for using the methods best suited to addressing the research questions at hand (Bourdieu & Wacquant, 1992). Bourdieu has used a range of different approaches, which broadly divide into quantitative and ethnographic approaches (Fries, 2009). These reflect his own position of “constructivist structuralism”, which relates to his arguments about the “dialogic interplay of objective and subjective social factors” (Fries, 2009, p. 330), a stance I summarised in Chapter 3. Harrits (2011) argued that Bourdieu’s ‘praxeological knowledge’ approach deals with the double hermeneutics problem of the social sciences (after Giddens, 1993) where two perspectives coexist: that of the observer and that of the social actor (Harrits, 2011). This means that “social analysis must be done both from outside and from within, or as Bourdieu argued, that explaining and understanding are one” (Harrits, 2011, pp. 160-1). Harrits (2011) recommended the use of statistical analyses to explore structure alongside interpretive interviews to explore meaning and experience. She argued that findings from these two perspectives do not need to mirror one another as in more traditional triangulation methods used within mixed methodology (Harrits, 2011). This is because Bourdieu’s view, summarised in Chapter 3, is that social agents may not perceive these structural constraints. Nonetheless Bourdieu argued that socialisation informs actors’ practice and leads to a certain amount of reproduction of these structural differences.
78 As argued above, it is not possible to explore the interplay between the social differentiation of the use of online support and information in everyday caring practices without using both quantitative and qualitative data within the same case study group of parents. In taking this approach I am also following Fries (2009), who used social, cultural and economic capital, habitus and fields to frame his own research. His aim was to answer an analogous question to my own, which was, “How do objective social structural conditions such as social class, gender, ethnicity, and education provide the objective context for the subjective decision to use complementary/alternative medical practices” (Fries, 2009, p. 338). He argued for the use of a sequential mixed method design (after Tashakkori & Teddlie, 1998), which began by mapping out structural differences with a survey and ended with an exploration of habitus through individual accounts. This approach is clearly relevant to the research presented in this thesis, where my aim is to explore how the objective social structural conditions of age, income and education provide the objective context for the subjective decision to use online support and information in one’s wider caring practices. As will be recalled in Chapter 3, I outlined four research questions, which are summarised in Table 4.1. These involved the exploration of macro structure, micro interactions and the possible habitus and capital related processes that link them together. In Table 4.1 I have included details of the method used to explore each question, which involves mixing methods across and within questions.
79 Table 4.1 Research questions, relationship to Bourdieu’s concepts and methods used
Research question Bourdieu’s concepts Method 1. Are younger, wealthier and Cultural capital (as measured by qualification Survey more educated parents of held) people with Rett syndrome Economic capital (as measured by household more likely to use online income) support and information than Differentiated generational practices (as others? measured by age) 2. Are different platforms for Cultural capital (as measured by qualification Survey online peer support socially held) and differentiated so that parents Economic capital (as measured by household interview of people with Rett syndrome income) are brought together ‘in a Differentiated generational practices (as seemingly fortuitous way’? measured by age)
Sense of affinity of people sharing similar practices and background (in interview accounts) 3. How does an individual’s Relevant capitals and ‘goods’ available in Interview habitus and possession of different subfields online (e.g. knowledge, different forms of relevant advice). cultural and social capital Habitus (own relevant practices and tastes) affect their use of caring- Habitus (as above, perceived in online subfield) related online support and Use of other sources of social capital. information? 4. How does the use of online Cultural capital (as measured by qualification Survey peer support sites influence held) and wider caring practices? Is Economic capital (as measured by household interview there any evidence of income) differentiation of benefits by Differentiated generational practices (as age, income or education? measured by age)
Relevant capitals and ‘goods’ gained in different subfields online (e.g. knowledge, advice, increasing economic capital).
Habitus (relevant practices and tastes in the use of online information and support and in
80 wider caring work). There were two stages of research. Stage 1 aimed to test the social patterning of online peer support use and comprised a survey of parents of people with a diagnosis of Rett syndrome living in the UK. Stage 2 explored in depth how online peer support meshed with wider information seeking strategies and social capital resources and what constrained and limited participation in specific online subfields. As can be seen in Table 4.1, the Stage 1 survey explored aspects cutting across three of the research questions. These were the social differentiation of online support and information, particular platforms for peer support and resulting benefits. The Stage 2 interview explored how an individual’s habitus and possession of relevant forms of cultural and social capital affected their use of online information and peer support and their use of this information and advice in their wider caring practices. This stage also involved filling out a record of recent visits to online peer support sites and, if available, use of a computer, smartphone or tablet to check details, which were used as aide memoires during the interview. The following sections give further details about how these stages were implemented, the research tools used, process of research, samples drawn and analysis methods used. A third stage, exploring online interactions, was originally proposed and approved by the University of Surrey Ethics Committee (see Appendix 2 for approval letter). This aimed to triangulate findings from the other two stages through exploring the use of language, dominant discourses and social sanctioning in two public peer support sites and groups used by interviewees. Anonymised covert observations were to be made as requests to observe may have prevented or deterred parents from posting on these sites and groups during fieldwork. However, the only public sites ever used by interviewees were charities’ Facebook pages on which little, if any, peer support was given. This was an interesting and unexpected finding, which is discussed in more detail in Chapter 7 in relation to the greater symbolic capital held by organisations as compared to parents within these online subfields. In addition my developing research relationships with parents and gatekeepers and increasing transparency in sharing my results introduced a risk of deterring parents from using such sites in the future if covert observations were
81 carried out alongside this more open method of engagement. As a result, I decided that carrying out observations on public sites would yield no useful additional data and raise ethical difficulties. Instead I retained my focus on parents’ accounts of relevant practices in relation to the use of online support and information. I was able to verify descriptions of online practices in an informal way while looking up links provided in online support use records (see the beginning of section 4.3 for details) or during interviews, when sites were often browsed to aid discussion.
4.2 Stage 1: Quantitative survey of parents of people with Rett syndrome
Following the rationale described above, Stage 1 aimed to map out the structural differences in parents’ use of the Internet and online support and information related to caring for someone with Rett syndrome. In particular, this involved exploring differentiation by age, income and education, as outlined in the first research question. Respondents to the survey also provided a sampling frame for recruitment into Stage 2, as described in the next section. A survey was chosen as an appropriate method for making planned comparisons between groups (Sapsford, 2007, p. 10), in this case age, income and education groups. As the survey used mostly quantitative questions this allowed the construction and comparison of statistical descriptors of this population (Groves et al., 2004), facilitating comparisons between these groups of interest.
4.2.1 Hypotheses and exploratory analyses As described in Table 4.1 above, the survey addressed research questions one and two and part of question four. A set of hypotheses was created, which are listed in Table 4.2 alongside the relevant research question. These hypotheses were based on the literature reviewed in Chapter 2. However, it is important to note some of the ambiguities and gaps within the literature and the reasoning behind how these hypotheses were created and why some could not be created. Hypotheses relating
82 to the social differentiation of the use of the Internet overall, its use for caring information and the use of online peer support are based on the strongest evidence described in Chapter 2, although it is somewhat limited in places. Preliminary findings suggest that there is social differentiation of the use of the Internet for health information, with younger, wealthier and more educated people more likely to use it in this way. However, with regard to the use of online peer support, the evidence is less clear and what is known is based on a single study of a single forum (Leonard et al., 2004). This study found that although there was greater use among more educated and professional parents, the utility and benefits of the group were rated lower by parents working in clerical, professional and management posts and older parents. Posting behaviour is another grey area. Oxford Internet Survey (OxIS) data shows a greater level of posting across different online platforms by younger people and people with higher incomes. However, given the lower amount of time spent on RettNet by professional, clerical and managerial groups and older parents (Leonard et al., 2004), it is possible that this does not hold true for posting on online peer support sites.
83 Table 4.2 Hypotheses to be tested in Stage 1
Research question Hypotheses 1. Are younger, wealthier and a. Internet use will be significantly positively related to income and more educated parents of education and significantly negatively related to age. people with Rett syndrome more likely to use online b. Among Internet users, use of the Internet for information and support and information than advice related to Rett syndrome will be significantly positively others? related to income and education and significantly negatively related to age.
c. Among Internet users, younger, wealthier and more educated parents will be significantly more likely to have ever visited an online peer support site.
An exploratory analysis will be undertaken to explore whether age, income or education are related to ever having posted on an online peer support site.
2. Are different platforms for An exploratory analysis will be undertaken to explore the role of online peer support socially education, income and age in use of different peer support differentiated so that parents platforms. of people with Rett syndrome are brought together ‘in a seemingly fortuitous way’? 4. How does the use of online a. Among users of online support, younger parents and those peer support sites influence who do not work in a professional, clerical or management wider caring practices? Is there role will be more likely to report benefits of use. any evidence of differentiation of benefits by age, income or An exploratory analysis will be undertaken to explore whether education? income or education are related to the benefits of using online peer support.
84 4.2.2 Design of the survey The full survey questionnaire is available in Appendix 3. An introductory page included key information about participation including an outline of the research, estimated time required to complete the survey and how data and anonymity would be protected. Parents were asked to choose one person to fill out the survey per household. This was to ensure that each respondent provided information about the caring practices of a single household8. The questions were divided into five sections: the first asked about sources of support and use of the Internet; the second and third were for current Internet users and ex-users respectively, and covered use of online support groups, social capital benefits and (for ex-users) reasons for stopping use; the fourth section was for people who had never used the Internet and covered intention to use, reasons for not using and views on potential benefits of use, including caring advice and support; the final section covered key demographic details and included an interview request for current online support site users. As outlined in the first section of this chapter, I aimed to establish whether there were structural differences in the use of the Internet, online support and information and online peer support groups. My choice of measures was based on the evidence of social differentiation of online support and information use presented in Chapter 2 and the arguments about the role of economic and cultural capital in understanding differentiation of the Internet in Chapter 3. I was also informed by Bourdieu’s use of structural measures in Distinction (Bourdieu, 1984), where he combined household income, education and occupation to explore socio- occupational class differences and as part of his operationalisation of cultural and economic capital. As discussed in the final section, the numbers of respondents to my survey were too low to carry out complex comparisons across combined categories; so single categorical variables were used instead. Therefore household
8 Although this may have led to completion by the parent who was more active online (see later data about Internet use), this would still have provided more information about the impact of online support and information within wider caring practices as they related to someone with Rett syndrome within one household. 85 income was used as a proxy for economic capital and education as a proxy for cultural capital. Occupation was used as a reflection of socio-occupational class only where there was an indication that occupation rather than education or income was likely to differentiate use. This also reflects a pragmatic decision based upon the high number of parents in this sample who were full-time or part-time carers, some of whom had given up high-status occupations in order to care full-time. In addition, some parents’ part-time roles were likely to reflect fit with caring duties, rather than reflecting class background. Therefore education was seen as a more fitting way of exploring class affiliation in a way that was more analogous to Bourdieu’s (1984) conception. I operationalised social capital sources by asking parents about their views and use of specific forms of alternative sources of caring-related information and support: local health professionals, telephone support from an organisation, local group support and online support. Appendix 4 summarises details of the measures used in each section. In order to make meaningful comparisons with Oxford Internet Survey (OxIS) data collected during my survey fieldwork period I sought and secured permission to use Internet use and demographic questions from the latest OxIS questionnaire (G. Blank, personal communication, May 17, 2012). However it should be noted that the OxIS is interviewer-led, while my survey required self-completion. Where possible, I have followed the wording of the 2013 OxIS questionnaire. However I sometimes made minor changes to make questions more appropriate for self-completion9. Where new questions were created they used the same anchoring terms, categories and terminology used in the OxIS questions where possible and relevant. This included use of demographic measures of age, income, occupation and education used by OxIS in order to facilitate comparisons with wider Internet use findings. In order to measure the benefits of online sources of support I was guided by
9 The biggest wording change was from the OxIS interviewer asking ‘Do you yourself personally use the Internet at home, work, school, college or elsewhere or have you used the Internet anywhere in the past’, followed by a prompt about ever having used the Internet, I split this into two questions and reduced the words to support recall and understanding of the question. The question used in my survey was, ‘Do you currently use the Internet on any device (at home, work, school, college or elsewhere)?’
86 Ferlander’s (2007) descriptions of four kinds of social support that can be accessed through social capital resources described in Chapter 3. I adapted relevant items from Williams' (2006) Internet Social Capital Scale (ISCS) that related to Ferlander’s (2007) definitions of informational, emotional and instrumental support (see Appendix 4).
4.2.3 Pilot phase I attended a Rett UK Regional Day and talked to interested parents about my research and planned survey. Five parents agreed to pilot my survey. Three parents and my external supervisor gave feedback on the full draft of the survey, providing some minor wording improvements, which were incorporated into the final survey. Additional online support sites were added to the survey as a result of suggestions. Parents suggested that the ideal time for a survey was 10 minutes, with a maximum of 15 minutes. I asked five friends to time themselves completing the longest path through the survey. This took them up to 10 minutes to complete. The expected time to complete the survey was listed as between 10 and 15 minutes on the survey to take account of the additional time needed for parents to remember details required to answer certain questions.
4.2.4 Structure of final survey All respondents were routed through the survey depending on their answers to filter questions. This was through written directions in the paper version or automatically in the online version. The survey was created using Survey Monkey’s online software ( www.surveymonkey.com ) Select package, which allows rerouting from irrelevant questions. The online survey was adapted to create a paper version based on a PDF (Appendix 3), in order to “keep the essential survey conditions as similar as possible across modes [of data collection]” (Groves et al., 2004, p.164). Paper questionnaires were printed as A5 booklets. The question about recruitment channel was excluded from the paper survey as all paper surveys were sent out with letters to Rett UK
87 members (see below)10. The question about current Internet access was excluded from the online survey as online completion demonstrated current access.
4.2.5 Reaching parents of people with Rett syndrome My focus was on UK-resident parents11 of living people with Rett syndrome. I aimed to recruit 250 parents. As with many groups of carers or people with a specific condition or syndrome, there was no central database listing people with a diagnosis of Rett syndrome. At grant proposal stage I had negotiated permission to recruit a random sample of parents from the British Isles Rett Syndrome Survey (BIRSS), a research database that contained 930 family contacts. However, when I met with the Cardiff University staff managing this database to finalise arrangements, they informed me that only 300 contact records were known to be current and that the majority of referrals came from Rett UK’s membership database. We therefore agreed that a different sampling frame would be more appropriate for this research. As described in Chapter 1, Rett UK (established in 1985) was the only UK charity completely focused on providing support for parents. Rett UK have a large database of members (1200 households at the time of my fieldwork), including parents of people with Rett syndrome. As noted in Chapter 1, the only other Rett- specific UK charities (Rett Syndrome Research Trust and Cure Rett) were relatively new, having been established in 2009 and 2012 respectively (Rett Syndrome Research Trust, n.d., Cure Rett, n.d.) and neither offered membership at the time of the survey. Rett UK’s database of members is updated every two or three years. However membership required a subscription fee until 2011, meaning there was a risk it would slightly underrepresent less wealthy parents. Rett UK gave permission for me to send a letter to their ‘family’ members and details of the two mailings I sent to Rett UK members are described in Appendix 5. This includes a description of the letter sent to members (Appendix 6). As will be seen below, I added additional
10 Had any further surveys been requested through the other channels, a note would have been written on the survey to allow coding of this channel. However, none were. 11 This included foster parents
88 channels of recruitment in order to reduce any biases of completely relying on this database as a sampling frame. However, the nature of the available sampling frames meant it was not possible to carry out a randomised sampling approach. Given my intention to compare groups across multi-level variables (e.g. household income by use of specific support spaces) any attempt to draw a simple random or stratified random sample from the Rett UK membership risked drawing too few responses for the kinds of analyses planned12. This would potentially be worsened given the likely low response rates among carers (for instance, 40% among carers in Blackburn and Read, 2005). There was no way of creating a larger sampling frame of eligible parents as not every source contained sufficient demographic detail. Finally, as some channels were public (e.g. public online groups) it was not possible to estimate their reach to eligible parents. I instead decided to recruit as many people as possible and then try to establish how much my sample was representative of eligible members of Rett UK, who provided the largest potential pool (and number of respondents) in this sample. As outlined above, Rett UK’s membership database is the most complete sampling frame and therefore the closest there is to a UK-wide estimate of demographic makeup of this group and certainly of the main sample population from which I was recruiting. In order to assess any sample biases I compared the demographic profile of survey results with an anonymised version of Rett UK’s database (see Appendix 5 for details of how I created this database). As I needed to reach as diverse a group as possible to aid diverse recruitment into Stage 2, I carried out additional recruitment through online support sites. It was likely that there was a group of parents who were not accessible through these channels, which all required some form of engagement with charities, email newsletters or online support groups. This potentially introduced a bias towards parents who may be (or have been) more actively seeking information. Therefore articles about my research were also included in Rett UK’s newsletter, which is posted out to all members and then posted online at a later date. This increased the potential pool of parents via contacts with professional carers, friends and relatives of parents who were not
12 Sapsford (2007) suggests that there should be at least 20 people per cell in each comparison 89 affiliated with any charitable body or reading online support groups. A copy of my initial recruitment article can be found in Appendix 7, which included key study information provided through other channels. I added reminders about the research within subsequent articles in the newsletter. Despite these efforts, I acknowledge the possible impact of a likely bias toward parents actively (or previously actively) involved in information-seeking in my interpretation of findings in Chapters 5-8. To maximise recruitment through all channels I provided surveys in online and paper formats and gave interviewees a choice of a range of modes of interviews. The use of three different mediums (letters, newsletter article and online postings) necessitated different approaches to recruitment, which are described in more detail in Appendix 5. I initially collected survey data between the middle of November 2012 and 21st December 2012. However, as I had only received 140 responses by this date, I reopened data collection after I had received ethical approval for my second mailing (see Appendix 8). This second period ran from 22nd March 2013 until July 2013. The second mailing went out to 577 people on 22nd March 2013. Details are given in Appendix 5 and the follow-up letter (Appendix 9) and a form aiming to assess reasons for non-response and eligibility in the sample (Appendix 10) are also described there. Reminders were also sent out in Rett UK’s newsletter and in the online sites and groups as before. Non-parental family members or bereaved parents completed some surveys sent out in the first mailing. In discussions with Debbie Main, my external supervisor at Rett UK, it transpired that this database included the full range of familial relations, not just parents. Appendix 5 gives full details of how I managed the second mailing to avoid these difficulties. During data entry of paper surveys, I noticed a number of misprints. These had occurred during conversion from my PDF questionnaire into the printing software used by the printers. Misprints were mostly minor, preserving the legibility of the questions (boxes replaced the hash tags in questions about Twitter, the ampersand in ‘Yorkshire & the Humber’, the ‘2’ in ‘NVQ 1 or 2’ and the é of ‘Internet Café). Unfortunately two misprints compromised the legibility of two questions. In the question on part-time working hours a box replaced the ‘2’ in ‘Working part-time
90 8-29 hours per week’, but the full-time hours being listed as 30 hours a week or more provided helpful context. The most unfortunate printing error was in the household income question, which made the first three income categories (up to £30,000 per year) illegible in paper surveys. This meant that only online surveys and paper surveys that had been sent out and returned during the second mailing collected details of household income under £30,000 (74 online surveys, 15 paper surveys with accurate data in the under £30,000 per year groupings, n = 89, 46.8% of all surveys). In some of the paper questionnaires containing the misprint one of the lower categories had been ticked and sometimes cases respondents had written in a salary band range that could be related to existing boundaries. Paper surveys were therefore coded using any of the categories over £30,000 that had been ticked, as “under £30,000” or into one of the lower categories if enough additional information had been given. Respondents earning over £30,000 were able to indicate their earning band across both survey formats, meaning that accurate household income data was available for all respondents earning over £30,000 (n=92). In total, accurate, full data was available about household income for 78.6% of the sample. The number of people who indicated that they earned £12,500 or less was very low (n=7) and all had completed the online survey. If, as found in the OxIS, far fewer people in this category used the Internet than in other groups (58% as compared to 88% and over in other groups: Dutton and Blank, 2013), one would expect a disproportionate number of respondents earning under £12,500 per year to fill out the paper survey, the majority of which were misprinted. Therefore, the ‘Under £30,000’ group may include – and disguise - a large group of people earning under £12,500 per year. Thirty two parents requested a new survey. New surveys sent out corrected printing errors found in the original survey. Fifty new eligible responses were received in the second survey data collection period: two new paper surveys, 20 old paper versions of surveys and 28 further online surveys.
91 After ineligible and incomplete online responses13 had been excluded, there were 190 complete, eligible survey responses. Checks for duplicate responses were run in SPSS and none were identified. It was difficult to calculate a definitive response rate, so a maximum sampling frame number of 607 was calculated by subtracting 12 ineligible parents identified from the second mailing from the final sampling frame size of 619. The minimum response rate based on letter returns from this maximum sampling frame was 26%, but given the possibility of over-inclusion - for example of unidentified family members plus parents of children who do not have a formal diagnosis or who have not informed Rett UK that they have been bereaved - it may well be much higher. There were 71 responses to the second mailing questions about non- response, including 58 from eligible parents. This represented only a small fraction (14%) of returns from non-responding parents who were sent a letter through Rett UK, so is not representative of the whole set of non-respondents. Nonetheless, it provided illuminating data, especially from a group that were unwilling to engage in the research and might otherwise have been unrepresented. The next section outlines the characteristics of the survey sample.
4.2.6 Characteristics of survey sample Table 4.3 shows proportion of recruitment by channel. A large majority (83%) were recruited through letters sent to named Rett UK members. Those recruited online were from a range of online channels: Rett UK’s Facebook Page (13), other Rett- specific Facebook pages and groups (six), Twitter (three) and a PMLD Network email (one). Although respondents were given a choice of survey mode at recruitment, they most often responded in the mode in which they were approached. Sixty-four per cent of parents who were sent a letter with a paper survey responded in that mode, while all parents recruited through all other channels completed an online survey, none requesting a paper survey. Overall, 61% of respondents returned a
13 It was stipulated in the online survey information that if parents wished to withdraw from the survey they could stop at any point, so incomplete surveys were withdrawn.
92 paper rather than an online survey, reflecting the greater number recruited through letter.
Table 4.3 Recruitment channels for survey respondents
Method of recruitment n % of sample Letter to named Rett UK member(s) 158 83.2% Rett UK newsletter only 4 2.1% Online 23 12.1% Through a friend or relative 1 0.5% Not given 4 2.1%
This section highlights salient characteristics of the survey sample and describes what can be gleaned about non-response biases. Rett UK data was summarised for households asked to complete the survey in the second mailing (see Appendix 5 for details). This included data about 619 households. The available data depended on the membership form used. Less data was collected from more recent records. Table 4.4 presents demographic data available on Rett UK’s database, which is compared with the sample data. This represents data available on individuals listed either as a couple or as a single member (n= 977). Some comparisons were difficult to make due to missing data – most notably age data, which was only available for just under half of relevant members and gender information, which was not always available. Nearly a quarter of data on ethnicity was missing, making this comparison less meaningful.
93 Rett UK sample Survey respondents n % n % Member or respondent age 23-34 15 1.5% 15 7.9% 35-44 95 9.7% 47 24.7% 45-54 148 15.1% 50 26.3% 55-64 95 9.7% 49 25.8% 65+ 70 7.2% 24 12.6% Not known 554 56.7% 5 2.6%
Ethnicity White 724 74.1% 179 94.2% Ethnic minority 27 2.8% 7 3.7% Not known 226 23.1% 4 2.1%
Gender Female 224 36.2% 163 86.0% Male 37 6.0% 21 11.0% Couple (not specified) 357 57.7% n/a n/a Missing 1 0.2% 6 3.0%
Occupational group Managers, Directors & Senior Officials 29 3.0% 7 3.7% Professional Occupations 119 12.2% 30 15.8% Associated Professional & Technical Occupations 50 5.1% 11 5.8% Administrative & Secretarial Occupations 46 4.7% 11 5.8% Skilled Trades Occupations 55 5.6% 1 0.5% Caring, Leisure & Other Service Occupations 44 4.5% 14 7.4% Sales & Customer Service Occupations 10 1.0% 2 1.1% Process, Plant & Machine Operatives 16 1.6% 0 0.00% Elementary Occupations 13 1.3% 2 1.1% Carer 177 18.1% 70 36.8% Retired 46 4.7% 33 17.4% Missing (not taken, given or not enough information) 371 32.8% 9 4.7% Table 4.4 Comparison of individual data from Rett UK database with sample demographic data
The sample drawn appears to have under-represented men and ethnic minorities but represented a range of occupations, although over a third of survey respondents were full-time carers, a higher proportion than in the Rett UK database. Some of these differences may have been due to the instruction to choose one person to complete the survey, where female respondents may be more active in seeking out health information. Nonetheless, as stated earlier, this may have meant
94 data was collected about the person more likely to be using online support to inform household caring practices, potentially giving a more accurate reflection of its influence within a household. Survey respondents were aged between 23 and 89, with the majority of respondents aged between their 30s and 70s. There was a low proportion of parents aged over 65, but this was a greater proportion than those found in the Rett UK database. Due to missing data on age in the Rett UK database, it is hard to assess whether there are fewer older carers on the database overall, but a smaller number in this age group may partly reflect the higher rate of sudden mortality among people with Rett syndrome than in the general population (see Chapter 1). Table 4.5 compares household-level data available on the Rett UK database and in the survey sample group. There was more information available on the age of children of members with Rett syndrome (calculated from year of birth) than on the parents’ ages, although there was missing data for 104 children. There appears to be a slightly higher representation of parents of younger children in the sample, although of course missing data might mask higher levels of membership among parents of younger children.
95 Table 4.5 Household information comparison between Rett UK members and survey respondents
Rett UK sample Survey respondents
n % n % Age of child with Rett syndrome Pre-school age (0-4 years old) 6 1.0% 13 6.8% Primary school age (5-10 years old) 63 10.2% 34 17.9% Secondary school age (11- 16 years old) 116 18.7% 44 23.2% Post-school age (17-25 years old) 139 22.5% 37 19.5% Aged 26-38 years old 132 21.3% 42 22.1% Aged 39+ years old 59 9.5% 15 7.9%
Not known 104 16.8% 5 2.6%
Region of UK
Scotland 22 3.6% 8 4.2%
North West 66 10.7% 24 12.6%
South West 55 8.9% 24 12.6%
Wales 18 2.9% 7 3.7%
South East 95 15.3% 46 24.2%
Greater London 82 13.2% n/a n/a
London n/a n/a 17 8.9%
East of England 22 3.6% 8 4.2%
East Midlands 40 6.5% 20 10.5%
West Midlands 67 10.8% 13 6.8%
96 Yorkshire & the Humber 55 8.9% 11 5.8%
North East 19 3.1% 8 4.2% Northern Ireland 14 2.3% n/a n/a
Not known 64 10.3% 4 2.1%
97 In terms of regional representation, survey respondents represent most of the range of areas covered by members, excepting Northern Ireland, which was left off the list of areas in the survey in error (although nobody added this information to the additional information box at the end). Where region could not be ascertained from address information, this was noted as ‘not known’, but only 10% of records had this problem. Given the overlaps between categories of the South East and London in the survey and Greater London in the membership database, the percentages were not very different from one another overall, suggesting reasonable representation of members by area. Not shown in Table 4.5 is the proportion of households with two children with Rett syndrome, which was about equivalent, with nine among Rett UK members (1.5%) and two among survey respondents (1.1%). Similarly, seven children of members of Rett UK had male children with Rett syndrome (1%) compared with one in the survey sample (0.5%). Overall then, data in the sample was reasonably reflective of the diversity of members of Rett UK in terms of geographical area covered and occupational group, although there was a higher representation of retired people and carers in the survey sample. Women were probably over-represented in the survey sample. It was possible that younger parents of younger children and people identifying as having a ‘White’ ethnicity were more highly represented in the sample than among members although it was difficult to judge differences due to missing data. However, it appears that younger parents were reached through the addition of online recruitment, which added another 22 respondents (12% of the sample) not reached through other media. Parents recruited solely through an online source were significantly younger on average (41 years old, ranging from 23 to 60 years old) than those recruited through at least one non-online source (average 52 years old, ranging from 29 to 89 years old)14 and doubled the number of respondents in this age group from seven to 15.
14 A chi-square comparison of age groups was significant, 2 (4) = 28.30 p< .001, with a significant and moderate association between age and recruitment mode (Cramer’s V score of .393, p <.001). The significance derived mostly from the much higher percentage of the 23-34 year-old age group (p< .001) that were reached only online (34%) compared with the sample average of 8.2 per cent.
98 Appendix 11 includes further information about sample respondents that was not available from Rett UK membership records. It was most common for children to have received their diagnosis when aged under four (59.9%) or between five and 11 years old (21.4%). Seventy two per cent of respondents’ offspring with Rett syndrome lived in the respondent’s household all of the time. The majority of respondents had some form of higher education (43.2%), although just fewer than a third had reached basic or secondary education and 9% had no qualifications. It was difficult to assess the household income of respondents due to the printing error, but about one third earned under £30,000, with a spread of household earnings across the full range of categories from under £12,500 per year to £80,000 or more. Internet use among survey respondents was very high (91.6%) compared with the current UK rate of 78% (Dutton and Blank, 2013). As this is not a randomised sample, it is not possible to conclude whether or not use of the Internet overall is higher among this group of carers than in any other group or whether this reflected a self-selection bias. However, in data from the non-response form, a third of those choosing not to participate cited a lack of interest in the topic because they did not use the Internet, suggesting a slight self-selection bias. Nonetheless as the main focus of this thesis is on understanding the differential role of online support and information in everyday caring practices among current Internet users, this sample still allows for a thorough exploration of the research questions posed in the previous chapter.
4.3 Stage 2: Qualitative interviews
As outlined in Table 4.1, interviews were used to explore the micro processes involved in the use of online peer support and information, in particular in answering research questions two to four. Thus interviews were used as described by Fries (2009) as a way of exploring people’s accounts of their own practices in terms of online and offline support and information seeking, their dispositions toward the Internet and online information and platforms, and how they used information in
99 their wider caring practices. As such the aim was to uncover relevant forms of habitus through these dispositions and practices. These were used to try to explore individual agency and how this related to the constraints of structural differences. Semi-structured qualitative interviews were chosen because they allowed an in- depth exploration of the complexity of people’s experiences (Mason, 2002, p. 65) while retaining a topic-based but flexible structure (Bryman, 2008, p. 438). As part of the interview preparation, parents were asked to complete short records of their use of online peer support sites (see Appendix 12). These included details of the posts they had viewed, the responses to it and whether they commented or not. The record was available in three formats (paper questionnaire, Survey Monkey survey designed to be readable on all net devices, and editable Word document). These records were designed to be used as elicitation cues rather than sources of data (similar to the use of text messages in Rettie, 2008), so were destroyed after the interview. This approach was adopted to avoid the burden of a full diary for parents with high demands on their time, where the data collected may be of varying quality or may not be collected at all. Not all parents completed records. Their use was supplemented or replaced by parents looking up information on the Internet during the interview, an element introduced by a parent at the first interview and adopted in subsequent interviews where online access was available.
4.3.1 Recruitment UK-resident parents who had visited any online support site related to caring for their child15 with Rett syndrome in the last three years were eligible to participate. Recruitment began with the first surveys sent out on 21st November 2012. A total of 55 parents noted their interest in participating in an interview through the survey. Six parents were not eligible and I contacted them to thank them for completing the survey and explain why I was unable to interview them. Initially each eligible volunteer was emailed to request setting up a time for a phone call to discuss the next stage of the research or telephoned if they had only provided a telephone number. In these phone calls I described the interview process
15 This included adult children
100 and measures to protect data and anonymity, answered any questions and tried to build some initial rapport. I sent all parents who still expressed interest in the research a covering letter or email (Appendix 13), a paper or electronic copy of the Information Sheet (Appendix 14) and the consent form (Appendix 15). Whenever I received a completed consent form I contacted parents to make final interview arrangements. Some parents, although initially interested and in some cases returning consent forms, changed their minds about participating when we were trying to set an interview date and in one case a parent texted to cancel an interview the evening before it was due to happen. I faced ethical challenges at various points in the recruitment process. One parent had consented but had not come back to me to confirm a date for the interview. Another parent had agreed to participate in an email interview but did not respond to the opening email in the interview. On contacting both I discovered that their children with Rett syndrome were in intensive care. Another parent told me on a follow-up call that her mother had just died, but that I could ring her after the funeral. In all of these cases I decided the most ethical course of action was to remove any sense of obligation to participate by asking parents to contact me if they wished to continue with the research. None of these parents came back to me. After following up all parents who had indicated interest through the survey I made some direct appeals for interviewees in the Rett UK newsletter and the online forums where parents were recruited for the survey, linking to details posted on my research website, which was based on recruitment information sent in the letter to Rett UK members (Appendix 6). As a result of this I gained consent from two further parents to participate in the research (via Twitter and through a family member) and both also agreed to complete surveys. Twenty parents began interviews with me and nineteen completed them (see below for further detail). Thirteen were Rett UK members, four were recruited online, one heard about the research through a friend and one did not share how they had been recruited. I carried out one joint interview as the husband of the main interviewee stayed and participated, although he contributed less than the primary interviewee. Less is known about this interviewee, as he had not filled out a survey.
101 4.3.2 Mode of interview Prospective interviewees were advised that interviews were expected to take between one and a half and two hours. For those who agreed, a choice was initially given between three synchronous modes: face-to-face, Skype or telephone interviews. Where synchronous interviews were not viable, email interviews were offered. As email interviews are asynchronous they can be completed in short episodes when convenient (Opdenakker, 2006). By offering these to parents I hoped to avoid excluding parents with the most caring responsibilities or with competing demands from both work and home. However, I stressed that the material of a synchronous interview would still need to be covered. A preference-based selection of mode was used to avoid generating researcher-centric biases between modes, for example providing face-to-face interviews to those within a local travel radius. When an interview date or start date (for email interviews) was agreed interviewees were asked to fill out records with two or three examples of carers’ online support sites and groups they had visited in that time. Where interviews were carried out in private residences, I left a sealed envelope with the address with my husband. I arranged to call him by a certain time and he was to open the envelope only if he was unable to contact me by then or I did not return home. On returning home I destroyed these details. I made private reflexive audio notes as soon as possible after each interview, usually immediately afterwards in my car. Where records of online support site use had been completed, these were used as elicitation cues when talking about specific sites during the interview. Parents were also encouraged to look up details of posts they had read or sites and groups they used if a computer or smartphone were available for this purpose. Where records were used, in some cases parents kept possession of the records, describing their contents to me, which allowed them an additional level of confidentiality and control over the interview process. In practice, all parents used either records, notes or real-time checking of sites and groups as elicitation cues during the interview. The use of records or of real-time browsing produced different kinds of reflections.
102 Parents using their own notes would talk more about their own experiences of browsing and what they had found useful or interesting, while parents browsing online would discuss their impressions of the sites, which were sometimes sites they had not browsed for some time. In both cases, personal experiences and attitudes to regularly used sites were elicited and analysis focused on the key areas outlined above in terms of their own practices and dispositions. At the completion or termination of each interview parents were given a sheet including my contact details and a range of support services (Appendix 16).
4.3.3 Interview schedule The interview schedule (see Appendix 17) covered interviewees’ general use of the Internet and their experiences of having visited different support sites. Following Fries (2009), the questions were designed to find out about the detail of practices as part of a reflexive sociological approach, focusing on descriptions of practices and their taken-for-granted dispositions (i.e. habitus) towards the Internet, information and support seeking and wider caring practices. For each site they used regularly they were asked about the regularity and frequency of use, reasons for posting or not, perceived norms of the site (to explore perceived site habitus) their similarity to other users and users’ views (to assess ‘affinity’ and shared habitus), types of advice sought and found, reactions to conflicts, the use and utility of advice gained online, information-seeking strategies across sites and offline sources and the benefits and limitations of online support. This schedule was used flexibly, with topics covered in the order they arose in the interview.
4.3.4 Sample I had aimed to recruit a range of parents who used online support sites in different ways and who could shed light on the demographic trends found in Stage 1. Given the difficulties of securing participation outlined above, my sample was essentially a convenience sample, comprised of all parents who had agreed to and been able to complete my interview. However, possibly due to the survey sampling through a range of mediums, there was still a good variation in use of the Internet, age of
103 parent and child with Rett syndrome, time since diagnosis, household earnings and geographical location. This meant that, as originally planned, interviewees were able to give a broad picture of their use of the Internet, which could give some insight into the demographic patterns of use outlined in the results section, particularly as these related to age and time since diagnosis. Table 4.6 provides key demographic data about interviewees. All but four of the interviewees were female and all but two were White (of British origin). Although 13 interviewees had spent their whole lives living in the UK, six had spent some time living elsewhere, sometimes living abroad for a few years, while one person had moved to the UK from South Africa in adulthood and one did not share information about their background. It should be noted that one parent was from the United Arab Emirates (and had only spent one year in the UK completing a Masters qualification). This did not become clear until the interview had been arranged but the interview was completed because it shed light on an interesting and little-researched phenomenon – the use of UK support sites by parents living abroad. In terms of UK geographical regions, there was a reasonable spread across many parts of England, but no one from Scotland, Wales, the North East or the Midlands was interviewed. Interviewees lived across a range of urban and rural settings.
104 Table 4.6 Demographic details of interviewees by mode of interview chosen
Face- Vol to-face Telephone P16 Email (n=9) (n=5) (n=3) (n=3) Total Gender Female 8 5 2 1 16 Male 1 0 1 2 4
Age 0
23-34 0 1 0 0 1
35-44 4 1 1 3 9
45-54 1 3 2 0 6
55-64 3 0 0 0 3
Region resident
North West 0 3 0 1 4
South West 2 0 0 0 2
South East 3 1 1 2 7
London 2 0 0 0 2
East of England 0 1 0 0 1
Yorkshire & the Humber 2 0 1 0 3
(United Arab Emirates) 0 0 1 0 1
Occupational status
Working full-time 1 4 2 1 8
Working part-time 3 0 1 1 5
Unemployed 0 0 0 1 1 Doing housework, looking after children or other persons 4 1 0 0 5
Occupational groups
Managers, Directors & Senior Officials 0 2 2 1 5
Professional Occupations 3 1 0 1 5
Associate Professional & Technical Occupations 2 1 0 0 3
Caring, Leisure & Other Service Occupations 0 0 1 0 1
16 Voice over Internet Protocol (VoIP) interviews included Skype and Google Hangout interviews. 105 Interviewees tended to be from a narrower range of occupations than the survey respondents and to be more qualified and earn more. However, there was still some variation in the whole group. The majority of interviewees (15) had received some form of higher education qualification. Just over half of the interviewees worked either full- or part-time, while five were full-time carers. The majority of currently employed interviewees had occupations ranked in the three top hierarchies in the Office for National Statistic’s Standard Occupational Classification 2010 (Management, Professional and Associate Professional and Technical Occupations), with one interviewee working in a service occupation. The highest earning person in the household most often had a job from one of these top three hierarchies, although in three households nobody held a job. The household income of interviewees ranged between £12,500-20,000 per year to £80,000 or over, but nearly half of interviewees came from households bringing in over £70,000 per year. The first interview took place on 14th February 2013 and the final (email) interview was completed on 21st May 2014 (this overlapped with survey data analysis). The length of synchronous interviews ranged from 70 minutes to a four- and-a-half hour-long interview, which is discussed further below. The completed asynchronous email interviews took between a month and a half to eight months17 to complete, with between 47 and 71 emails exchanged (counting emails from both parties). Table 4.6 also summarises demographic differences among interviewees by mode chosen. Just under half of interviews (including the joint interview) were undertaken face-to-face, with the rest carried out over the phone (five), over Skype or Google Hangout online call (three) and email (three). All but one of the interviews (an email interview) were completed. After a long email silence and a few attempts to contact this interviewee via email, they informed me that they had had a nervous breakdown. Although this individual was initially keen to continue the interview in a different mode, we ultimately agreed it would be better to terminate the interview after a period of suspension and they gave permission for me to analyse the partial
17 At a rate of about two emails a week. Some of these were reminder emails from me.
106 interview. It is notable that all email interviews took place among people in the 35- 44 year old age bracket. Efforts to avoid a face-to-face interview bias in the South East were successful. However, none of the interviews in the North West were carried out in person. In part this was due to parents’ solicitousness in selecting what they thought would be ‘easier’ for me, despite my efforts to reassure them it was not problematic for me to travel, perhaps compounded by some parents’ concerns about ‘not being of much help’. The interview I carried out in Yorkshire and the Humber was carried out while I was up in Manchester for a conference and it is possible the parents may not have agreed to my travelling up for this interview if it had been solely for the interview. Appendix 18 provides details of interviewees’ children with Rett syndrome and relevant details of interviewees’ Internet use for caring-related purposes. All interviewees had one child with Rett syndrome. The majority of children were of school age (n=15). Ten children lived at home all of the time, one part of the time and eight lived elsewhere. The youngest child was three and the eldest was 28. All children had received their diagnosis of Rett syndrome before the age of 11, with nearly half receiving it at the age of two. Children had received their diagnoses between 17 years and under a year ago, with over half having received a diagnosis in the nine years prior to the interviews. Almost all of the interviewees had been using the Internet for at least six years and all rated their ability to use it as good or excellent, the highest categories. The majority of parents had read carers’ groups or sites within the last month. Most interviewees agreed or strongly agreed that reading such sites was beneficial in terms of reducing a sense of isolation or solving problems, although one parent was neutral about these benefits. Sixteen of the parents interviewed said they had posted at some point in a carers’ group or site and most had done so within the last month.
4.3.5 Reflection on the interview process In one sense, I occupied the position of an outsider in my interviews, as I am not a parent of someone with Rett syndrome and have no children of my own. Nearly all
107 parents asked me why I had chosen to focus on parents of people with Rett syndrome, perhaps seeking to ascertain whether I had a personal or family connection. Only one interviewee asked me whether I had any children and when I said I did not, she provided a detailed reflection on what it was like to receive criticism of her parenting approach, rather than assuming a shared understanding. On the other hand, my experience of having worked with carers and people with profound physical and learning disabilities gave me some insight into the caring dilemmas and shared experiences of carers of children with physical and learning disabilities. This meant that interviews could proceed smoothly with a shared knowledge of specialist therapies, medication and complex health problems. I also shared with all parents a familiarity with the Internet and experience of using social media (Facebook, including closed groups and Twitter) and some specific groups and forums (Carers UK online forum and the PMLD Network emails). I have also read and posted on some unrelated online peer support forums personally, which has given me a useful perspective on the experience of being a site or group ‘user’ seeking support, information and understanding from other people in a similar situation. These considerations aside, rapport could vary for a number of reasons. I noticed I generally had an easier rapport with parents closer to my own age (36 during fieldwork), noticing fewer pauses before they answered questions and a greater volunteering of information. The rapport was fastest and strongest with women who also had a similar level of education. I noticed that parents aged over 50 disclosed less information about their emotional experiences or difficulties faced, although they were initially more forthcoming in their accounts about the negative aspects of sites. My most challenging interview was one that lasted for four and a half hours. Given that the expected interview length given in the information was up to two hours, I regularly checked with the interviewee that they were happy to continue. This interviewee drew upon detailed anecdotes to illustrate key points, including the wider experiences of friends and family. This was the only interview where I found it hard to contain my own emotional reaction to the events described, which involved alleged medical neglect and the resuscitation and near loss of her then infant daughter with Rett syndrome. Although I ensured the key topics were covered and
108 tried to keep the role of online support as a key focus, it felt inappropriate to interrupt descriptions of difficult and traumatic experiences and I was mindful that interviews needed to offer something in return for the generous sharing of personal and difficult information. The mode of interview influenced the process of building rapport before the interview and reading of emotional responses during the interviews, but did not affect the ability to build rapport overall. Face-to-face interviews involved a greater lead-in and rapport-building phase. However I was most aware of time constraints during face-to-face interviews, possibly as a result of being more aware of non- verbal cues from interviewees that they were getting restless or tired, when I would end the interview as soon as possible. Skype and telephone interviews were started with very little lead-in time as they were often undertaken in the evening and once at the weekend and the sense of having a bounded slot of time was intensified. However, I did not notice any mode-specific differences in level of disclosure, with some (usually younger) parents sharing difficult and personal experiences with me in every mode. It was difficult to judge in telephone and impossible to judge in email interviews when parents were becoming upset. Across all interviews it was hard to anticipate which questions would raise difficult issues. I did not press interviewees to talk about very difficult issues (such as postings about bereavement) if they had not raised them. Two parents cried briefly during the interviews. In both cases I stopped the interview and allowed the interviewees to collect themselves before giving them a choice about whether or not to continue. Both recovered quickly and indicated they were happy to continue. Email interviews raised a series of specific ethical and procedural dilemmas. Although I set up an expectation of sending reminders ‘in case my email has got lost in a busy inbox’, it was difficult to anticipate how long to leave between reminders and how to pace the interview. When answers to questions determined the following sets of questions I tended to list ‘(if yes)’ or ‘(if no)’ follow-up questions, which made these sections more like a questionnaire. Interviewees tended to give brief answers at the beginning of the interview and it took time to encourage them to be more expansive. As noted above, one email interview took place over seven
109 months, sometimes with gaps of one or two weeks between replies and this was very time-intensive as it required regularly rereading what had already been discussed. Finally, some interviewees opted to use their work email accounts even after I raised the possibility that these may not be entirely private. Nonetheless, the provision of a range of interview modes enabled me to maximise the range and number of parents who were able to participate and gain some useful insight into the role of online support among parents of a children of a relatively diverse range of ages. This allowed me to explore how experiences had changed within a wider socio-historical context, as represented in Figure 1.1, as well as providing particularly useful data in exploring social differentiation in this sample.
4.4 Summary of the data analysis processes
This section describes how the data was analysed and interpreted, how limitations were overcome and how mixed method and mixed mode data was combined.
4.4.1 Analysis and interpretation of quantitative data As outlined in the first section, following Fries (2009) and Harrits (2011), quantitative data was analysed in order to explore differentiation in terms of the use of online support and information within the wider sample group of parents of people with Rett syndrome. Given the limitations of the sampling process and the slight biases described above, this could not be used to generalise to the whole population of people with Rett syndrome, although there were some similarities with the Rett UK database information in terms of range of occupations and region of UK. As noted above, there appeared to be a slight over-representation of carers and of women. Nonetheless, as interviewees were drawn from this sample, survey data was still suitable to provide a contextual backdrop against which to explore the role of interviewees’ practices, habitus and capitals in seeking information and support related to caring for a child with Rett syndrome and the relationship to wider caring practices. In this sense survey data acted like a set of contextual, detailed case
110 studies. As noted in Chapter 2, little is known about the online practices and social differentiation of the use of online peer support among a wider group of parents of people with a rare syndrome, with existing research either exploring users of a specific forum or being based on qualitative interviews with parents of children with a range of different syndromes. As argued in Chapters 1 and 2, comparisons across different rare syndromes would dilute the value of such insights, as they would include confounding extraneous factors, such as differences in caring responsibilities and the different socio-historical backgrounds of each syndrome. The data presented in this thesis is therefore valuable in understanding the social differentiation and role of online support and information in the everyday practices of a case study group of parents of people with a specific rare syndrome, sharing a particular socio-historical context that raises shared caring dilemmas (as discussed in Chapter 1). Statistical tests were used where possible to test the hypotheses and strength of relationships because this is preferable to relying on subjective, perceived magnitude in non-randomised samples (Sapsford, 2007). I used the program SPSS to carry out all statistical analyses and summaries of descriptive data reported in this thesis. In mixing online and offline survey data, it is important to avoid measurement error, where questions might be answered differently in different modes (Dillman et al., 2009). Appendix 19 outlines the checks I undertook to assess the comparability of survey data collected across modes, following best practice guidance in survey methodology. These checks established that there were no significant differences among modes that would affect data quality. The number of survey responses (n=190) limited the complexity of statistical tests that could be carried out. This had two impacts on the tests carried out below. Firstly, where variables had multiple categories, this often needed to be reduced to allow enough expected counts per cell in chi-square tests. This may have obscured wider patterns in the data and nuances that could be ascertained in a larger sample. Data relating to reasonable sample sizes per comparison is reported here; for each statistical result and presentation of descriptive data reported, a series of tests have been carried out to find the best fit for the data. Secondly, it was not possible to run logistic regressions or chi-square tests with multiple predictive variables. In practice
111 this meant that where more than one factor influenced how online support was used it was not possible to disentangle the independent contribution of these factors. In analysing my quantitative data I therefore followed Fries (2009) in arguing that although Bourdieu tended to use correspondence analysis (e.g. in Bourdieu, 1984), “other statistical techniques […] can be used to explore the objective relations within social space”. While Bourdieu (1984) was able to top up his initial sample for Distinction with a larger sample to allow for this kind of analysis, this was not possible in this population, with these sampling frames. However, as argued in Chapters 5, 6 and 8, these limitations did not adversely affect my ability to answer the research questions posed in this thesis.
4.4.2 Analysis and interpretation of qualitative data As with cross-modal quantitative data, there has been some argument about the comparability of qualitative data collected in different modes with regard to the research process, building rapport, technical problems and expressing emotion. I therefore reflected upon these aspects before combining data. VoIP interviews were very like face-to-face interviews, the only difference being the lack of lead-in time discussed above and occasional technical problems necessitating the move (in one case) to a telephone interview. Email interview data differed in that more people dropped out without informing me first and interviewees could edit their responses – although there was some evidence of spontaneity in some email interviews, with long sentences used when discussing emotive topics and typos left uncorrected. Finally, interviewees were able to use humour and express emotion across all modes (for instance, using punctuation and emoticons in email interviews). As noted above, rapport appeared to be affected more by age differences, although this did not appear to affect the level of disclosure related to Internet practices. A themed analysis was used to sort, code and analyse the data, informed by the procedure detailed in Lofland and colleagues (2006). This method was chosen because it allowed the combination of pre-existing theoretical coding with emerging themes. While transcribing interviews I created some initial codes and memos about the nature of the data. Once I had imported my transcripts into NVivo I created some
112 initial codes reflecting key categories noted in this emergent coding and some reflecting key thematic concerns. This initial coding included both broad higher-level codes to organise nodes (‘social patterning mechanisms’, ‘meshing with info-seeking and social capital resources’) and initial descriptions of ‘constraints and limitations of online forums’ that had emerged from transcript coding and memoing. I also included a ‘not sure yet’ category for any other intriguing and potentially useful findings. Where parents talked specifically about their dispositions toward the Internet, parenting and information practices and tastes, these were coded under a set of ‘habitus’ codes. After I had coded each transcript, I created a case study memo to capture each parent’s account of how their use of online support and information reflected relevant aspects of their practices and dispositions as well as existing sources of support, and the role such information and support played in their wider caring practices. This was done in order to avoid missing the richness of individual experiences within a themed coding approach, and in particular to understand the individual contexts within which the seeking of information and support occurred, which was used to inform findings reported in Chapters 6 and 7. As I coded my first few manuscripts I became aware of the importance of differentiating between different sites and sources of information (online and offline) and changes in the use of these sources over time. I therefore added codes for each source and when they were considered useful, as well as coding descriptions of how use had changed over time. My final set of codes were organised under the following headings, which reflected the interplay between the use of online and offline sources through habitus, across time and between social groups. These were: ‘personal habitus, capitals held’, ‘use of knowledge and connections in caring practices’, ‘fit between personal habitus and subfield and social capital habitus’ and ‘social capital and subfield resources used’. The final stage of my analysis involved creating a set of matrix codes to explore the patterning of different uses and dispositions among parents of different ages, education and income groups. Following the advice of Lofland and colleagues (2006) I developed and refined models to explore emerging theories based on the data.
113 4.4.3 Mixing data from different methods As noted in the first section of this chapter, the intention was to combine data to explore different aspects of the use of online support and information and how they may connect to wider structural differences, particularly whether they reflected the predictions made in the first part of this chapter. This involved establishing whether the social differentiation predicted in research questions existed in this dataset and how they impacted on the use of online support and information, the use of particular platforms for online peer support and the benefits accrued from such sites. Social differentiation results are presented within Chapter 5 to provide a context for exploring the micro aspects of use and how these interplay with these broader structural differences in Chapters 6 and 7. However, although quantitative results are mostly presented within a single chapter, they are drawn upon in the following chapters to draw together findings to answer the research questions posed at the end of Chapter 3. However, it is important to note that the mixing of data was not something that only happened in the presentation of and reflection on the findings. The processes of analysis described above overlapped and influenced each other. Therefore, as I was initially analysing my survey data, I had begun my interviews and the role of age and expertise in the use of online support sites was becoming clearer. As I wrote up my qualitative findings and presented my initial work to colleagues, I became aware of further statistical analyses I could carry out in order to explore intriguing aspects of my qualitative data. This iterative process was an important part of the shaping and refining of my thesis over time.
As argued above and in Chapter 2, the recruitment of carers is complicated given the lack of comprehensive sampling frames. Furthermore, data on the use of online support and information among carers has tended to be fragmented down methodological lines, limiting the ability to explore the interplay between social differentiation of use and everyday practices. As was to be expected, it was not possible to draw a randomised sample and the sample drawn may over-represent women and full-time carers. Nonetheless, my sample does represent a wide range of occupational groups and carers from across the UK, as well as a range of age groups. Moreover the survey data still enabled the
114 qualitative data to be explored within the frame of a wider group of contextual case studies. This allowed, as planned in the research questions, an exploration of the interplay between structure and individual practices of interviewees, who were drawn from the same survey sample. As such, the findings presented in the following chapters provide an original contribution to our understanding of the role of online support and information in the everyday caring practices of parents of people with a rare syndrome. Chapter 5 explores structural differences hypothesised to exist among parents of people with a rare syndrome with regard to their use of online support and information within wider caring practices. This is followed by Chapter 6, which builds on these insights to explore the micro processes involved in seeking information and advice over time and in response to other sources of support, as well as the differential use of online peer support subfields. Chapter 7 explores struggles for symbolic capital within online subfields and social differentiation of the use of information gained online in gaining symbolic capital within wider caring fields. Finally, Chapter 8 summarises how these findings have contributed to the wider literature as summarised in Chapters 2 and 3.
115 Chapter 5. Structural differences in the use of caring- related online support among survey respondents
As discussed in Chapter 4, given the rare incidence of Rett syndrome and the lack of a comprehensive sampling frame, it was not possible to draw a randomised sample. Therefore, as I discussed in the previous chapter, these results reflect survey respondents’ approaches to online support and information. However they are still able to provide a context for the use of the Internet in the everyday caring practices of interviewees that can be used to inform understanding of how these parents’ social differences may constrain and influence their micro practices as outlined in the research questions. Although a set of hypotheses was set out in Chapter 4, a formal testing of these is not really desirable, as this would suggest generalisability of findings. Instead the questions underlying these hypotheses as they relate to the wider research questions about this sample of parents will still be explored, with reference to the specific structural differences described. As noted in Chapter 4, I follow Sapsford’s (2007) suggestion to use statistical tests in order to move beyond subjective impressions of data in a non-randomised sample. Chi-square comparisons were chosen in preference to more complex statistical analyses, as discussed in the previous chapter, as they allowed for comparisons within a relatively small sample. The results presented in this chapter can add to the existing literature much like qualitative case study work, highlighting potential future avenues of research, as well as allowing for the exploration of how social differences might influence micro practices in a case study group, bounded by this sample. This chapter begins with three sections that explore three of the research questions posed at the end of Chapter 3. Section 5.1 investigates the social differentiation of the use of online support and information in this sample. Section 5.2 explores the social differentiation of the use of different platforms of support among respondents. Section 5.3 describes the social differentiation of benefits gained from online support sites. After that, section 5.4 uses available quantitative
116 data to explore some of the possible connections between the social differentiation and use of the Internet for caring that were made in Chapters 2 and 3. This includes the relevant social differentiation of digital competence, access and experience, the use of existing sources of support and other factors related to the age of respondent, a key differentiating factor found in this data. This chapter closes with a summary of how parents’ position in the wider socio-historical context of communication and medical changes may influence their use of online support and information, using relevant statistics to outline key differences among different age groups. This raises a series of questions that will be explored in the following chapters, exploring how this social differentiation is linked to the everyday practices of interviewees drawn from this sample group.
5.1 Social differentiation of the use of online support and information among survey respondents
In Chapter 3 I summarised arguments that inequality of access to and use of the Internet could be viewed through a Bourdieusian lens, as a reflection of unequal economic capital, or economic capital converted into other capitals (social and cultural). Following the findings in existing research, a set of different aspects was explored in relation to age, income and education. These were: overall use of the Internet; seeking online support related to caring for someone with Rett syndrome; ever having visited an online peer support site; and ever having posted on an online peer support site.
5.1.1 Social differentiation of the use of the Internet in this sample As noted in Chapter 4, use of the Internet was high in this sample (91.4%, n=169). As shown in Table 5.1, below, use reduced with age, a highly significant difference, 2 (2) = 47.78 p< .001 with a (p <.001) Cramer’s V score of .508, suggesting that around half of the variance in Internet use could be explained by age of respondent.
117 Table 5.1 Frequencies and percentages of use of the Internet among key groups.
Internet use
Current user Ex-user Never used Total
Age of respondent n % n % n % n
23-44 years old 62 100.0% 0 0.0% 0 0.0% 62
45-66 years old 97 92.4% 2 1.9% 6 5.7% 105
67-89 years old 10 55.6% 2 11.1% 6 33.3% 18
Annual household income
Under £30,000 58 86.6% 1 1.5% 8 11.9% 67
£30,000 to under £60,000 56 94.9% 2 3.4% 1 1.7% 59
£60,000 and over 33 100.0% 0 0.0% 0 0.0% 33
Education
No higher education qualification 85 85.9% 4 4.0% 10 10.1% 99 Holds higher education qualification 80 80.0% 0 0.0% 2 2.4% 82
Internet use also increased slightly with household income, which was significant, 2 (1) = 5.75 p< .05 but with a lower Cramer’s V score of .190 (p <.05), suggesting low explanatory value. Level of Internet use did not appear to differ much between people with and without a higher education qualification, but no chi-squares could be carried out on this data due to low expected cell counts. Therefore, aside from the much higher prevalence of Internet users in this sample, the social patterning found in this sample reflected differences by household income and age found in the Oxford Internet Survey (OxIS: Dutton and Blank, 2013). This suggests that within this sample, parents’ use of the Internet may not be very different from that of people in general, a finding that is in keeping with other surveys on carers’ use of the Internet in terms of age and suggested by employment status (Blackburn et al., 2005)18.
18 Blackburn and colleagues (2005) did not measure household income.
118 The rest of this chapter explores the social differentiation of the use of online social capital sources as sources of caring-related support.
5.1.2 Social differentiation of the use of generic online support related to caring in this sample There are many different sources of information and support related to Rett syndrome and caring for a child with health and communication difficulties. This section explores the use of generic online support, which was defined on the questionnaire as “Online support and advice (related to parenting someone with Rett syndrome)” that could be “seen on websites, blogs, discussion boards, Facebook groups, chat rooms or emails from email groups”. As such it was not exclusive to peer support messages exchanged between parents and could include support and advice gained from professionals and organisations. Overall, 83.7 per cent of the survey respondents had read this kind of online support (n=159). This represented 92.3 per cent of current Internet users (n=155) and 75 per cent of ex- users (n=3) but also one person who had never used the Internet (16.7% of this group). This final finding may either reflect proxy use through someone else – which was not what I intended to measure here - or may have been an error in completing the survey. The use of this kind of support was therefore tested among respondents who had ever used the Internet, to avoid confounding results with Internet use findings. Ninety two per cent of respondents who had used the Internet at some point had used generic online support. It is perhaps not surprising that nearly all respondents who had used the Internet had at some point looked for support or advice about Rett syndrome. Table 5.2 presents frequencies and percentages of use among key groups. There was little difference between use among income groups and chi-square cell counts were too low to carry out a comparison. Similarly, there appeared to be little difference between those who did or did not hold a higher education qualification and this difference was not significant.
119 Table 5.2 Frequencies and percentages of use of generic online support and advice among key respondent groups19
Ever read generic online support and advice
Age of respondent n %
23-44 years old 60 96.8%
45-66 years old 87 90.6%
67-89 years old 9 75%
Annual household income
Under £30,000 52 91.2%
£30,000 to under £60,000 56 98.2%
£60,000 and over 32 97.0%
Education
No higher education qualification 80 92.0%
Holds higher education qualification 73 92.4%
Age of respondent was the only variable significantly related to use of generic online support, 2 (2) = 6.69 p< .05 but with a low Cramer’s V score of .198 (p <.05). The significance in this chi-square test was derived from the higher (25%) than expected level of respondents who had never used generic online support (8.2% in the whole group) in the 67 to 89-year-old age group, with little difference between the two younger age groups. However, it should be noted that this was based on very low numbers not using generic online support in this group (n=3). Overall then, there was little to differentiate the use of generic online support within this group, where the vast majority had used it at least once, although there was a suggestion that this was less popular among older respondents who had used the Internet (a very small group overall, n=12).
19 Calculated among parents who were current Internet users or had ever used the Internet.
120 5.1.3 Social differentiation of the use of online peer support in this sample Online peer support was defined on the questionnaire as “‘shared online support messages’ posted by other carers. These are messages asking for or giving support and advice related to caring for someone else. These messages are posted on a website or in an email group so they can be seen by others using it”. Three aspects of use were explored: ever having visited an online peer support site; recency of visiting such a site; and ever having posted on such a site. Seventy-three per cent of respondents who were current users of the Internet had read an online peer support site at some point. Table 5.3 compares results in use, recency of use, and posting across the three social groupings of interest. As suggested by the figures, there were no significant differences in respondents ever having visited an online peer support site by household income and education, where percentage of use was similar across categories. However, age of respondent was significantly and relatively strongly related to online peer support use, 2 (4) = 32.59 p< .001 with a Cramer’s V score of .434 (p <.001). As can be seen in Table 5.3, this represented a use by the majority of current Internet users in the sample aged under 44, use by about two thirds of those aged between 45 and 66 and a third of those aged 67 and over.
121 Table 5.3 Frequencies and percentages of use of online peer support among key respondent groups.
Use of online peer
support20 Read within
Ever read last month21 Ever posted22
Age of respondent n % n % n %
23-44 years old 56 90.3% 49 87.5% 49 87.5%
45-66 years old 66 66.7% 39 60% 42 63.6%
67-89 years old 4 33.3% 2 50% 3 75%
Annual household income
Under £30,000 46 78% 35 77.8% 35 76.1%
£30,000 to under £60,000 42 72.4% 30 71.4% 32 76.2%
£60,000 and over 27 81.8% 19 70.4% 18 66.7%
Education
No higher education qualification 64 71.9% 45 71.4% 49 75.4% Holds higher education qualification 59 73.8% 43 72.9% 42 72.4%
Forty-seven per cent of respondents who had ever visited an online peer support site had done so within the last month, with the remaining responses being spread more or less evenly among other categories (three to under six months, six months to under a year, then yearly intervals up to three years and over three years). Chi-squares were therefore carried out to compare use within and over a month ago to avoid the problem of low expected cell count. Although the proportions presented in Table 5.3 suggest more recent use by younger parents, expected cell counts were too low to carry out a chi-square comparison. As suggested by the similar levels among all categories within household income and
20 Among current Internet users 21 Among those who have ever visited an online peer support site 22 Among those who have ever visited an online peer support site
122 education groups, these variables were not significantly associated with differences in the recency of use of online peer support in this sample. Finally, among respondents who had ever read an online peer support site, comparisons were made between those who had ever posted and those who had not. In total, 125 parents in this sample had ever visited an online peer support site. Among this group, 75.4 per cent had also ever posted on one (n=92). Although there was a slightly lower level of posting among the wealthiest group in Table 5.3, household income was not significantly related to ever having posted. Level of education also did not significantly differentiate respondents who posted from those who only read online content. Due to low expected cell counts, it was not possible to make comparisons across age groups of respondents or their children. Due to the low numbers in the oldest group, the percentage of those posting in this group in Table 5.3 may be misleading. However, as shown in Table 5.3, posting in an online support group appears to be noticeably differentiated by age, with higher proportions of younger parents ever having posted in one. Table 5.4 summarises statistically significant findings reported in this section, which are used, as argued above, to provide an indication of strength of relationship within this sample. Age of parent was the strongest differentiator of the use of the Internet, generic online support and online peer support. Although comparisons across recency of use and ever having posted could not be carried out, descriptive statistics suggest a greater recency of use and proportion of posting within the 23 to 44-year old age group compared with the 45 to 66-year old age group. Overall then, findings suggested that use of the Internet for information and support relating to caring for someone with Rett syndrome was related to age much more than to income and education in this sample.
123 Table 5.4 Relationships between key variables and use of online support and information among survey respondents.
Age of Form of social differentiation Income Education parent
Current Internet use .190* - .508***
Sources of online social capital ever used
Generic online support ns ns .198*
Online peer support ns ns .434***
Recency of use of online peer support ns ns -
Content creation on relevant sites & groups ns ns - ‘-‘ depicts comparisons that could not be carried out due to low expected cell counts ns = non-significant comparisons that could be carried out. All figures given are Cramer’s V calculations. The highest result for each variable is highlighted * p< .05, ** p < .01, *** p< .001
5.2 Brought together ‘in a seemingly fortuitous way’? Social differentiation in the use of online support platforms among respondents
The sections to date have brought together use of online peer support across a range of different online platforms. As implied by the title of this section, Bourdieu (1986) argued that people may ‘seemingly fortuitous[ly]’ find themselves among a homogenous group in certain social spaces and it was proposed here that certain online support spaces may be similarly differentiated. All current users of the Internet were asked to indicate where they had ever read shared online support messages posted by other carers. Table 5.5 shows the overall percentage of use of each platform as a place where respondents sought information or support related to caring for their child with Rett syndrome. It is clear that not all platforms were equally popular, with Facebook Pages or Groups used
124 more than any other platform. There were a number of popular charitable Pages and parent-led Groups on Facebook and they featured prominently in interview accounts. The importance of Facebook Groups as a source of support and information was such that one interviewee, who had previously chosen not to sign up to Facebook, was considering opening a caring-specific account as she felt she was missing out on valuable information and support. Website comments, email groups and blogs had been read for this purpose by nearly half of all these respondents at some point. Discussion or message boards had only ever been used by just over a third of these respondents, while use of chat rooms and Twitter was much lower (18% and 12% respectively). Table 5.6 presents the frequencies and percentages of use by age, income and education groups and Table 5.7 presents the results of chi-square analyses for each comparison. In terms of income and education, there were no significant differences in use of platform, except in the use of blogs, which was differentiated by income, 2 (3) = 8.68, p< .05, with a nearly moderate association shown by a Cramer’s V score of .248 (p< .05). None of the individual cells in the comparison reached significance, but as shown in Table 5.6, there is evidence of a linear relationship, with increased use related to increased household income. It is possible that this may reflect greater converted time available to spend time reading sites with less of an information-finding focus, as described in Robinson (2009). Overall, age of parent has the strongest explanatory power among all variables tested here. The greatest use of each platform occurred among the youngest age groups. This did not add anything to the findings reported above, which had established that there was greater use in (undifferentiated) online peer support by younger parents.
125 Table 5.5 Percentage of use of each platform for support and information related to caring for a child with Rett syndrome.
% use among Platform Internet users Facebook 59%
Website comments 47%
Email groups 46%
Blogs 43%
Discussion or message boards 36%
Chat rooms 18%
Twitter 12%
However the evidence of wealth-related differentiation is important because, as will be discussed in Chapter 7, blogs were described by interviewees as differing from other forms of online support in their ability to provide a counter-narrative to traditional narratives about mothering children with serious health problems and disabilities. This means that – as well as younger parents – wealthier parents may have access to a wider range of narratives than other groups who only access parental Facebook Groups or organisational Pages and other kinds of online support detailed below. A notable finding was the lack of impact of education on all, and household income on almost all, platforms. Overall then, except for the use of blogs, the use of different platforms is again most differentiated by age of parent. However, it should be noted that the numbers of parents aged over 66 included in these comparisons is very low, meaning that percentages in this group may be misleading. However, this partly reflects lower use of the Internet in this age group, supporting the key finding that online support and information are not used much in this group overall.
126 Table 5.6 Use of different platforms by age, income and education
Discussion or Facebook Website comments Email groups Blogs message boards Chat rooms Twitter n % n % n % n % n % n % n % Age of respondent 23-44 years old 54 87.1% 31 54.4% 34 58.6% 36 62.1% 32 53.3% 19 31.7% 15 25% 45-66 years old 45 46.4% 41 44.6% 38 41.3% 33 34.7% 27 28.4% 10 10.6% 4 4.3% 67-89 years old 2 20% 3 37.5% 3 30% 3 30.0% 1 10% 1 10% 1 10% Annual household income Under £30,000 36 62.1% 26 48.1% 24 44.4% 21 38.2% 19 33.9% 10 18.5% 5 9.4% £30,000 to under £60,000 34 60.7% 22 44.9% 24 46.2% 25 47.2% 22 40.7% 9 16.4% 7 13.0% £60,000 and over 24 72.7% 19 59.4% 19 57.6% 23 69.7% 13 39.4% 10 30.3% 7 21.2% Education No higher education qualification 50 58.8% 36 45% 38 47.5% 32 39.0% 29 34.9% 12 14.6% 7 8.8% Has higher education qualification 49 61.3% 37 50.7% 36 47.4% 39 50.6% 31 39.7% 17 21.8% 12 15.4%
127 Table 5.7 Social differentiation of the use of different online platforms by income, education and age
Age of Form of social differentiation Income Education parent Different online platforms
Facebook ns ns .536***
Website comments ns ns .162*
Email groups ns ns .250*
Blogs .248* ns .278*
Discussion or message boards ns ns .352***
Chat rooms ns ns .274*
Twitter ns ns .393***
‘-‘ depicts comparisons that could not be carried out due to low expected cell counts ns = non-significant comparisons that could be carried out. All figures given are Cramer’s V calculations. The highest result for each variable is highlighted * p< .05, ** p < .01, *** p< .001
A key limitation of the data collected is that it can only tell us whether someone has ever visited one of these kinds of sites, so we cannot tell whether this is something that has happened recently or in the past. This is something that will be
128 teased out in the following chapters, which focus on how use is embedded in everyday practices.
5.3 Unequal profits or unappealing goods? The social differentiation of the benefits gained from online peer support by survey respondents
This section explores whether benefits gained from online support sources were socially differentiated. This includes results of a general rating of the utility of generic online support as well as the social capital-style benefits of online peer support. The latter were based on questions reflecting Ferlander’s (2007) definitions of the kinds of support that online sources of support could feasibly provide (emotional support, informational support and instrumental support: see Chapters 3 and 4). As discussed in Chapter 3, according to Bourdieu’s theory of capitals, we would expect some groups to be able to leverage greater benefits from groups where they can both convince others that they ‘belong’ and where those others possess capitals or other resources they require. This requires having some knowledge about whether different sources of online support (and particularly online peer support) can offer benefits that are meaningful and beneficial for particular groups of parents. Existing research reviewed in Chapter 2 suggests that generic online support and peer online support may differ in terms of what they may offer to particular groups. Thus gaining benefits from health information more widely appears to be differentiated by education, while the use of online peer support is more differentiated by age and occupation. This may reflect the differing levels of useful ‘goods’ available through lay information to certain groups of parents, particularly those who can gain useful benefits from generic support that may not come from peers and older parents, who may not have much to gain from online peer support, particularly if, as in this sample of respondents, the majority of users are younger and likely to have less relevant information and advice relating to their older child’s
129 needs. This could explain why Leonard and colleagues' (2004) study of RettNet subscribers found that younger parents and non-professional and allied groups rated this group as more beneficial. Younger parents would be more likely to have younger children and a relatively low base of knowledge related to caring for a child with Rett syndrome. It is possible that professional and allied groups were able to make greater use of wider sources of information, as suggested by differences in income and education in the Oxford Internet Survey (OxIS). Therefore, in addition to income, education and age, occupational level was also explored among this sample in terms of benefits gained from online peer support.
5.3.1 Social differentiation of the perceived benefits of generic online support in this sample There were low numbers of respondents rating generic online support as ‘not at all important’, which caused problems with low expected cell counts in chi-square comparisons. Therefore simplified importance ratings were used to test these hypotheses. These compared ‘not important’ (combining ratings of ‘not at all important’ and ‘not so important’) with ‘important to some degree (combining ‘important’, ‘very important’ and ‘essential’ ratings) among respondents who had used each source. This does represent a skew toward positive ratings but, given the low numbers involved, was unavoidable. Among respondents who had ever used it, 63.2 per cent rated generic online as important to some degree. This makes this form of support of lower importance than offline sources of support within the sample as a whole, where local group support was rated as important by 73 per cent of respondents who had used it, telephone support as beneficial by 81 per cent of users and support from local health professionals as important to 90 per cent of respondents who had used it. Table 5.8 presents the rated importance of generic online support by income, education and age groups and Table 5.9 shows results of chi-square comparisons. There is a slight decrease in the proportion of parents rating generic online support as important to some degree as income increased, but this was not significant. Rating by education level was not significant and proportions were about equal across respondents with and without a higher education qualification. Age, however,
130 was significantly related to the rating of generic online support, with younger parents more likely to rate it as important and a reduced proportion of importance across each older age category.
131 Table 5.8 Rated generic online support as ‘important’, ‘very important’ or ‘essential’ by age, income and education groups
Rated as important to some degree
Age of respondent n %
23-44 years old 46 78.0%
45-66 years old 48 55.8%
67-89 years old 3 30%
Annual household income
Under £30,000 38 73.1%
£30,000 to under £60,000 36 64.3%
£60,000 and over 18 56.3%
Education
No higher education qualification 50 62.5%
Holds higher education qualification 46 63.9%
Table 5.9 Social differentiation of the use of different online platforms by income, education and age
Age of Income Education parent Rated importance of generic ns ns .317** online support
** p< .01
132 These results are interesting in that they do not support the idea that more educated and wealthier parents may benefit disproportionately from general online support. However, ‘generic online support’23 may differ from information gathered online, reflecting advice and support seeking rather than information seeking. However, the differences in age do support the idea that online support is a more valuable ‘good’ to younger parents, who may have younger children, diagnosed more recently, and therefore possess less knowledge about Rett syndrome than older parents. These relationships are explored in section 5.4.
5.3.2 Social differentiation of the perceived benefits of online peer support in this sample Given sample-size-related difficulties with carrying out chi-square tests, the original variables (five-point Likert scales) were reduced to fewer categories to aid analysis with a limited sample. The new categories were ‘agree’ ‘neither agree nor disagree’ and ‘disagree’, with the former and latter categories subsuming the ‘agree strongly’ and ‘disagree strongly’ categories. However, most of these comparisons could not be carried out, with a few (non-significant) exceptions. Therefore new categorisation was used, bringing together negative and neutral responses and comparing them with positive responses and each relationship was tested again. Table 5.10 presents the frequencies and percentages of agreement with the benefits of reading online peer support by age, income, education and occupation. Table 5.11 presents results depicting the strength of these relationships.
23 Defined on the survey as, “Online support and advice (related to parenting someone with Rett syndrome)” that could be “seen on websites, blogs, discussion boards, Facebook groups, chat rooms or emails from email groups”. 133 Table 5.10 Benefits experienced from online peer support by age, income, education and occupation
Agree or strongly Agree or strongly agree that agree that reading reading about other parents’ others’ experiences has experience has made me feel less helped me solve alone problems
n % n %
Age of respondent 23-44 years old 52 92.9% 42 75% 45-66 years old 51 77.3% 47 72.3% 67-89 years old 3 75% 1 25%
Annual household income Under £30,000 22 81.5% 15 55.6% £30,000 to under £60,000 36 85.7% 32 78.0% £60,000 and over 26 96.3% 19 70.4%
Education
Does not hold a higher education qualification 50 78.1% 49 76.6% Holds a higher education qualification 54 91.5% 39 67.2%
Occupational group24 Full-time carer 40 80% 36 73.5%
Managers, Directors & Senior Officials 7 100% 4 57.1% Professional Occupations 21 87.5% 19 79.2%
Associated Professional & Technical Occupations 9 100% 6 66.7%
Administrative & Secretarial Occupations 5 100% 5 100% Skilled Trades Occupations 1 100% 1 100%
Caring, Leisure & Other Service Occupations 12 92.3% 9 69.2%
Sales & Customer Service Occupations 1 100% 1 100% Elementary Occupations 1 100% 0 0%
24 Among parents who were not retired or unemployed 134 Table 5.11 Social differentiation of the benefits of reading online peer support sites and groups
Household income Education Age Occupation25 Emotional support: reading others' experiences makes me feel less alone Agreement, neutral or disagreement - - - - Agreement versus other categories (neutral or disagree) ns .185* - - Informational support: reading others' experiences helps me to solve problems Agreement, neutral or disagreement ns - - - Agreement versus other categories (neutral or disagree) ns ns - ns ‘-‘ depicts comparisons that could not be carried out due to low expected cell counts ns = non-significant comparisons that could be carried out. All figures given are Cramer’s V calculations, described in the text. * p< .05 ** p < .01
Survey respondents who used online peer support were asked how much they agreed with four statements. The first statement was, ‘Reading about other parents’ experiences has made me feel less alone’. As will be remembered from Chapter 3, this emotional support question (after Ferlander, 2007) was added to take account of other benefits of online peer support that were not adequately covered by Bourdieu’s concepts of capitals, but were thought to be relevant to this group. However, as argued in Chapter 3, this variable could also be considered as a marker of belonging, or being among ‘like others’. This difference – between people in a similar situation and similar people – is discussed in Chapter 6, where parents made a distinction over time between these two states, sometimes making explicit reference to class. In the sample as a whole there was a high level of agreement (84%) with this statement, while only 5% disagreed or strongly disagreed. As can be seen from Table
25 Professional, clerical and management roles versus other roles (after Leonard and colleagues’ [2004] findings). 135 5.10, there were high levels of agreement with this statement across all categories of variables, the lowest being among the small group of parents aged 67 and over (75%, n=3) who had ever read an online peer support site. There were slight variations within variables, most notably in age and education, where the youngest and most educated parents rated the emotional support variable higher than the other two groups. Table 5.11 shows that this difference was only significant in terms of education level, (1) = 4.22 p< .05 with a low Cramer’s V of .185 (p <.05), reflecting higher agreement among parents with a higher education qualification, although cells did not reach significance. The age and occupational comparisons could not be made, and difference by income level were not significant. All survey respondents who had ever read online peer support were asked how much they agreed with the statement: ‘Information and advice in shared online support messages has helped me to solve problems.’ Seventy-two per cent agreed or strongly agreed with this statement, with only 6.4 per cent disagreeing or strongly disagreeing. Tables 5.10 and 5.11 showed that a much lower percentage of the oldest group agreed with this statement, although this was based on a single response. As a result, a chi-square comparison was not possible. While a smaller proportion of parents with household income of under £30,000 per year agreed that online peer support had helped them solve problems, this difference was not significant. Occupation was not significantly related to a stronger level of rated utility, unlike in Leonard and colleagues’ (2004) findings, although the lowest proportion of agreement was among Managers, Directors and Senior Officials (57.1%).
136 Survey respondents who had communicated with at least one person exclusively through an online peer support group (65.3% of the sample, n=62) were asked to rate how much they agreed with a series of statements about the benefits they had gained from this communication. None of the parents in the oldest age group, and the sales and customer service occupational group had communicated solely with another parent exclusively online. Tables 5.12 and 5.13 summarise the responses to these questions by relevant social groupings. As before, these calculations were based on comparisons between those who strongly agreed and agreed versus those who were neutral, disagreed or strongly disagreed. Many of these comparisons could not be carried out due to low counts in cells, and where they could be carried out, none were significant. Numbers by occupation were particularly small, making interpretation difficult. Overall, 65 per cent of this group agreed or strongly agreed that ‘When I felt lonely, there was at least one person I could talk to’ (emotional support). There was higher agreement with this statement across the younger age group as compared to the middle age group, but these differences did not reach significance. This benefit did not appear to be differentiated by income or education and was not significant. It was not possible to carry out a chi-square comparison across occupational groups. Seventy five per cent of the wider group communicating with some carers exclusively online agreed that ‘There was at least one person I could turn to for advice about making very important decisions’ (informational support). The pattern of findings was similar, with a greater level of agreement among the youngest age group and little differentiation in income and education. All chi comparisons could be carried out, but none reached significance. The greatest level of agreement among this group was with ‘They have given me information and advice that has helped me to solve problems’ (informational support), where 80.6% of this group agreed or strongly agreed with this statement. There was less difference between the two age groups on this question while a greater proportion of the wealthier group agreed with this statement than other groups. It was only possible to carry out a chi-square comparison for education, but this found no significant differences between groups.
137 Agreement with Agreement with ‘There Agreement with ‘They ‘When I felt lonely, was at least one person I have given me there was at least could turn to for advice information and advice one person I could about making very that has helped me to talk to’ important decisions’ solve problems’
n % n n %
Age of respondent 23-44 years old 30 78.9% 28 32 84.2% 45-66 years old 13 56.5% 11 18 75.0% 67-89 years old n/a n/a n/a n/a n/a
Annual household income Under £30,000 15 65.2% 15 18 78.3% £30,000 to under £60,000 19 79.2% 16 19 76.0% £60,000 and over 6 60% 6 9 90%
Education Does not hold a higher education qualification 23 69.7% 22 28 82.4% Holds a higher education qualification 19 70.4% 17 21 77.8% Table 5.12 Benefits experienced from contact with another carer on an online support site by age, income and education
138 ‘n/a’ No carers had communicated with another carer solely online in this group
139 Agreement with ‘There was at least Agreement with ‘They one person I could have given me Agreement with ‘When I felt turn to for advice information and advice lonely, there was at least about making very that has helped me to one person I could talk to’ important decisions’ solve problems’ n % n n % Table 5.13 Benefits experienced from contact with another carer on an online support site by occupation26
88 .9 Full-time carer 18 69.2% 69.2% 24 % 15 10 0 Managers, Directors & Senior Officials 2 100% 50% 2 % 2 77 .8 Professional Occupations 5 55.6% 77.8% 7 % 5 83 Associated Professional & Technical .3 Occupations 6 100% 83.3% 5 % 4 60 Administrative & Secretarial Occupations 5 100% 40.0% 3 % 3 Skilled Trades Occupations ------62 .5 Caring, Leisure & Other Service Occupations 6 75% 50% 5 % 3 n/ Sales & Customer Service Occupations n/a n/a n/a n/a a n/a 0 Elementary Occupations 0 0% - 0 % 0
26 Among respondents who were not retired. 140 The final statement was, ‘They would help me fight an injustice’ (instrumental support). Fewer parents (56.7%) within this subgroup agreed or strongly agreed with this statement overall compared with other statements. A greater proportion of younger and wealthier parents agreed with this statement. All chi-square comparisons could be carried out, but none were significant. The low numbers in this subgroup hampered these final comparisons. However, in terms of age, this should be interpreted within the wider picture presented so far within this chapter. A lower proportion of older parents had ever used the Internet, leaving only small numbers of older parents who were online and who had ever read online peer support or posted in an online support group. Finally, of those who had posted, none had communicated with another carer solely online. This is suggestive of different online practices to younger parents, which will be explored in the next section.
5.4 Exploring the role of age: time, child’s needs, alternative sources of support and digital differentiation
Table 5.14 summarises the significant findings reported so far in this chapter. It is striking that use of online information and support in this sample is most strongly differentiated by parents’ age, with only minor contributions from income and education, although it is possible that income differences may have been obscured by a lack of detail about respondents earning under £30,000 per year. As will be recalled, this reflects the greater use of online support, across a range of platforms, and greater benefits reported by younger parents, although the latter could not be tested significantly. The other significant findings in income and education suggest relatively weak relationships, except for the greater use of blogs among wealthier parents, which is of a similar significance level to the age differentiation. The remainder of this chapter explores a number of potential explanations for these differences that are suggested by the literature reviewed in Chapters 2 and 3 and by Bourdieu’s concepts. These are: differences in digital literacy and Internet access;
141 access to alternative sources of support; age of child and associated information and support needs; and time since diagnosis. This section therefore begins by testing the relationships between these variables and parental age. It goes on to compare the relative strength of these competing explanations for the findings. This chapter ends with a summary of how age relates to these wider variables as well as socio- historical and technological changes over time, which will be explored through parents’ own accounts in the following two chapters.
Table 5.14 Social differentiation of online support use within income, education, age of parent and occupational groupings.
Age of Form of social differentiation Income Education parent Occupation
Current Internet use .190* - .508*** n/a
Sources of online social capital ever used
Generic online support ns ns .198* n/a
Online peer support ns ns .434*** n/a
Recency of use of online peer support ns ns - n/a
Content creation on relevant sites & groups ns ns - n/a
Different online platforms
Facebook ns ns .536*** n/a
Website comments ns ns .162* n/a
Email groups ns ns .250* n/a
Blogs .248* ns .278* n/a
Discussion or message boards ns ns .352*** n/a
Chat rooms ns ns .274* n/a
Twitter ns ns .393*** n/a
Online peer support benefits
Emotional support (from reading) ns .185* - - p < .05; ** p < .01; *** p < .001; ns = not significant; ‘-‘ = comparison could not be carried out.
142 5.4.1 Relationship between age of respondent and key variables of interest Respondent’s age is related to and may function as a proxy for, a number of other important variables that were explored in Chapters 2 and 3 in relation to the social differentiation of the use of the Internet. These include factors likely to affect possession of social capital, the likelihood of finding worthwhile ‘goods’ in online support settings and differences in Internet practices. Tables 5.15 and 5.16 summarise these differences by the three main age groups discussed above. As can be seen in Table 5.16, age of parent was highly positively correlated with the age of a child with Rett syndrome and time since diagnosis. Time since diagnosis was also highly positively correlated with child’s age. Both age of child and time since diagnosis are likely to be associated with differences in information needs. For instance, information about diagnosis and prognosis (among the benefits of online support groups identified in Chapter 2) may be most sought after when a child is suspected of having a developmental problem or has just received a diagnosis. Time since diagnosis may also be associated with a greater level of access to different sources of social capital and information (along with child’s age, when diagnosis is late). Having access to existing alternative sources of (offline) social capital was identified by Gundersen (2011) as one possible reason why some parents did not engage with online peer support. Although access to social capital was not quantified here, use of two offline sources of support was measured. Telephone support was significantly related to age, although the group making the most use of this support were aged between 46 and 66 years old, so this cannot provide a possible explanation of why use is much lower in the eldest group. Use of local group support was not significantly associated with age. However, sources of support and information can be numerous, and include family, online sources of information that are not provided by peers and support provided by peers offline. These are explored in detail in the following chapter through interviewees’ accounts.
143 23-44 years old 45-66 years old 67-89 years old Key differentiating variables (n=62) (n=105) (n=18) Details of only or elder child with Rett syndrome Mean age of child 9 years old 23 years old 40 years old Range of children's ages 2-18 years old 3-42 years old 16-50 years old Average age of child at diagnosis 3 years old 6 years old 19 years old Range of children's ages at diagnosis 1-10 years old 1-28 years old 2-39 years old Average years since child was diagnosed 5 years ago 16 years ago 21 years ago Range of years when child was diagnosed 1997-2013 1981-2012 1982-2004 Internet use % current Internet users 100.0% 92.4% 55.6% Mean years using Internet 11 years 10 years 12 years Range of years using Internet 3-20 years 1-25 years 2-30 years % with mobile access to the Internet 85.2% 51.1% 25.0% % rate self as 'good' or 'excellent' at using Internet 90.3% 65.6% 60.0% Use of sources of social capital % ever used telephone support 71.0% 89.3% 80.0% % ever used local group support 77.4% 83.0% 69.2% Table 5.15 Descriptive statistics on key variables by age group of respondent
144 Table 5.16 Strength of relationship between age of respondent and key variables of interest
Age of respondent
Age of child .88***
Years since diagnosis .78***
Years using the Internet .25*
Mobile access to the Internet .43***
Self-rated ability to use the Internet -.32a***
Use of telephone support .252**
Ever used local group support ns a. Depicts a correlation coefficient rather than a Cramer’s V calculation * p< .05, ** p< .01, *** p< .001
Finally, as shown in Chapter 2, Internet use is differentiated by differences in access, technical ability and time spent online. As demonstrated in Chapter 3, these relate to digital inequalities that - it has been argued, following Bourdieu - may contribute to the reproduction of existing social inequalities. As shown in Table 5.16, age of respondent was significantly related to years using the Internet, although mean number of years did not appear to vary greatly in Table 5.15. However, this may reflect a tendency, noted among interviewees, of respondents finding it difficult to recall years of use, often finding they had underestimated or overestimated once we started discussing Internet use in terms of their caring history. Age of respondent was strongly significantly related to having mobile access to the Internet, with mobile access reducing with respondent’s age group (see Table 5.15). Age of respondent was also negatively and significantly associated with self-rated ability to use the Internet, indicating that as parents’ age increased, self-rated ability to use the Internet decreased. However, Table 5.15 shows that the main difference in high self-rated ability was between the youngest group and both older groups. Overall then, age of respondent in this sample is related to factors that the literature reviewed in Chapters 2 and 3 suggested are related to differential use of
145 the Internet, but may also reflect differences in information needs. These factors are age of child, years since diagnosis, years using the Internet, mobile access and self- rated ability to use the Internet. While a potential difference in access to alternative sources of social capital or support was found (in this case, telephone support), it did not explain the lower uptake of online resources among the older group, so interview data will be used to explore this explanation in more detail. The impact of these factors on the use of the Internet and benefits gained from online support is briefly explored next in comparison to the impact of respondent’s age.
5.4.2 Exploring the impact of age-related differences in differential use of the Internet and differing information needs Tables 5.17 and 5.18 summarise a series of chi-squares undertaken to explore the relative influence of the factors identified above as they relate to the research questions. Due to problems with multicollinearity and the small sample, it was not advisable to carry out a comparative analysis including all variables (for instance, a logistic regression) to assess the relative strength of each variable (Field, 2009). Instead I discuss the relative strength of relationships in providing a possible explanation for the differentiation of the use of online support and information in this sample. For each aspect of online support and information use, the strongest relationship is highlighted in yellow in Table 5.17. This shows that in all cases, the time-related variables (age of parent, age of child and years since diagnosis) provide the greatest explanation for variation in use of the Internet and online support in this sample. Tables 5.19 and 5.20 provide frequencies of use where age of child or years since diagnosis provides the strongest differentiation of use and benefits of online support and information. These tables are referred to in the following subsections, which summarise the contribution of different factors to each aspect of use.
146 Table 5.17 Social differentiation of use of the Internet and online sources of information and support by key variables
Self- rated Years ability to Age of using Mobile use Form of social differentiation Income Education parent Years since diagnosis Internet access Internet
Current Internet use .190* - .508*** - n/a n/a n/a
Sources of online social capital ever used
Generic online support ns ns .198* - - - -
Online peer support ns ns .434*** .397*** ns .283*** .226**
Recency of use of online peer support ns ns - .375** ns .258** .218* Content creation on relevant sites & groups ns ns - .343** ns ns ns
147 ‘-‘ depicts comparisons that could not be carried out due to low expected cell counts ns = non-significant comparisons that could be carried out. All figures given are Cramer’s V calculations. The highest result for each variable is highlighted * p< .05, ** p < .01, *** p< .001
148 Use of the Internet and online sources of support Table 5.17 shows differences in use of the Internet to find information and support relating to Rett syndrome. It was not possible to carry out comparisons over categories of child’s age and years since diagnosis to explore their impact alongside the impact of respondents’ age on use of the Internet. However, the strong relationship of age of respondent with Internet use mirrors data cited in Chapter 2 where use of the Internet reduces with age. Similarly, it was also not possible to make comparisons over the other variables into the use of generic online support. However, in terms of the use of online peer support, these results show that age of child is most important in differentiating use among respondents. As shown in Table 5.19, this represented a greater use among parents of school-age children, which dropped in subsequent adult groupings. Similarly, increased years since diagnosis was associated with reduction in use, with 91 per cent use in the first nine years, dropping to 68 per cent and lower in subsequent categories. Years since diagnosis most strongly differentiated the recency of use of online peer support sites. This relationship was not linear, with recency of use increasing among parents of children diagnosed over 20-24 years ago. This could be explained by the dynamic use of online support in relation to the changing needs of parents, which is described in interview data analysis in the next chapter. However, as can be seen in Table 5.20, numbers in this category were relatively low, so percentage comparisons are somewhat misleading. Age of child was also significantly differentiating, with fewer parents of older children having visited an online peer support site within the last month. Other factors influencing recency of use that may overlap with one another, included having mobile access, where having access was related to having visited an online peer support site within the last month. Similarly, lower self-rated ability to use the Internet was associated with a lower level of recent use.
149 Table 5.18 Social differentiation of use of different online platforms and benefits gained from online support sites and groups O c c u p Form of a Years social ti using Self-rated differentiatio Age of o Years since Interne Mobile ability to use n Income Education parent n Age of child diagnosis t access Internet Different online platforms n / Facebook ns ns .536*** a .457*** .460*** ns .343*** .230** n Website / comments ns ns .162* a .291* ns .18* .182* ns n / Email groups ns ns .250* a .321** .250* ns .226** .245** n Blogs .248* ns .278* / .370*** .336** .28** .25** .178*
150 a Discussion or n message / boards ns ns .352*** a .310** .281** - .313*** .169* n / Chat rooms ns ns .274* a ns ns ns .234** ns n / Twitter ns ns .393*** a .246* .219* .27** .297*** - Benefits gained from online support Importance of generic n online / support ns ns .317** a .197* .280** .199* .251** ns Online peer support benefits Emotional support (reading) ns .185* - - - .252* ns - - Informational ns ns - n ns .352** ns ns ns
151 support (reading) s Someone could talk to if felt alone ns ns ns - .395** ns ns - ns ‘-‘ depicts comparisons that could not be carried out due to low expected cell counts; ns = non-significant comparisons that could be carried out. All figures given are Cramer’s V calculations. The highest result for each variable is highlighted * p< .05, ** p < .01, *** p< .001
152 Table 5.19 Frequencies of use by age of child, where age of child is most strongly associated with differentiation
Ever read Ever Online relevant read Ever peer website relevant read support commen email relevant use ts groups blogs Someone could talk to if felt alone (carers online only)
n % n % n % n % n % 2 5 . 0 Preschool age (0-4) 13 100.0% 7 58.3% 3 % 6 54.5% 6 100.0% 5 8 . 8 Primary school age (5-10) 32 94.1% 15 53.6% 17 % 20 60.6% 19 86.4% 6 5 . 1 Secondary school age (11-16) 44 100.0% 10 27.0% 28 % 27 62.8% 11 61.1% 4 7 . 2 Young adulthood (17-25) 32 88.9% 7 33.3% 17 % 10 27.8% 5 50.0% 2 26-38 years old 31 81.6% 4 23.5% 9 6 8 22.2% 2 40.0%
153 . 5 % 2 0 . 0 39-51 years old 7 63.6% 0 0.0% 1 % 1 20.0% n/a n/a ‘n/a’ no parents in this category had communicated with another carer solely online.
154 Table 5.20 Frequencies of use by years since diagnosis, where years since diagnosis are most strongly associated with differentiation
Content creation Emotional Informational Recency of use of on relevant sites support (from support (from online peer support and groups reading) reading)
n % n % n % n %
0-4 years 29 90.6% 26 81.3% 31 96.9% 23 71.9%
5-9 years 22 71.0% 28 90.3% 24 77.4% 23 76.7%
10-14 years 16 66.7% 18 72.0% 21 87.5% 18 75.0%
15-19 years 12 66.7% 9 52.9% 15 83.3% 17 94.4%
20-24 years 8 80.0% 6 54.5% 10 90.9% 5 45.5%
25-29 years 2 22.2% 6 66.7% 4 44.4% 3 33.3%
Years since diagnosis most strongly differentiated respondents ever having posted on an online peer support site. However, as shown in Table 5.20, this was not a linear relationship, with a slight rise in ever having posted among parents of children who received a diagnosis between 25 and 29 years ago. Again this represents a low number of respondents, so percentages are slightly misleading. However, it is possible this may reflect differences in posting for advice or offering advice, which is explored in the following chapters. Interestingly, years using the Internet, having mobile access and self-rated ability to use the Internet did not distinguish between parents who had or had not ever posted online. However, this comparison is between respondents who had ever used online peer support, where competence was generally higher than in the rest of the sample (see Table 5.17).
Differential use of online platforms for information and support As can be seen in the tables above, use of different platforms was associated with multiple variables related to both time and digital competence, suggesting that both were important in influencing access (although, of course, with possible overlaps where these variables are related to one another). However, use of these different
155 platforms was still most strongly differentiated by age of child or of respondent. The relationship with age of child was interesting in that there was the highest proportion of readers of email groups and blogs among parents of secondary school age children, with higher reading of website comments among parents of pre-school age. This could reflect a number of changing aspects of information seeking and available resources over different carers’ lives. This could include differences in different media available at different times, the greater accumulation of useful sources of information and the interplay of changing needs with all of the above. The interview data explored over the next two chapters explores these interleaving aspects in greater depth. Those without mobile access to the Internet were significantly less likely to have ever used each of these platforms. Having a lower ability to use the Internet was also associated with lower use of Facebook, email groups, blogs and discussion or message boards. However, it did not differentiate use of chat rooms nor of website comments. Greater years using the Internet were significantly associated with greater use of website comments, blogs and Twitter. It was not possible to carry out comparisons on the impact of mobile use on Twitter or of years of use on reading discussion or message boards. However, descriptive results suggested that use of most platforms was differentiated by skill in using the Internet and ease of access through mobile devices.
Differential benefits gained from online support sources The rating of the importance of generic online support was most strongly differentiated by the age of the respondent. However, years since diagnosis - and to a lesser extent age of child - were also associated with differences in rated importance. A higher proportion of younger parents, with younger children, particularly those who had been diagnosed within the last seven years, rated generic online support as important than other groups did, with rated importance lowering over time and age of child. It was also interesting to note that the rated importance of the use of generic online support varies by years using the Internet and mobile access, which may reflect experience in seeking information and ease of access,
156 although self-rated ability to use the Internet was not related to this variable, suggesting that finding generic online support is not something requiring strong technical skills. By comparison, the benefits experienced from online peer support sources were not differentiated (or could not be tested) by years using the Internet, having mobile access or ability to use the Internet. Instead, emotional support and informational support were most strongly associated with years since diagnosis. However, as shown in Table 5.20, these were not linear relationships. Although the lowest proportion reporting experiencing these benefits were the group with children diagnosed more than 25 years ago, high proportions of parents of people diagnosed 15 to 19 years ago reported gaining informational support from online peer support sites, or emotional support among parents of people diagnosed between 20 to 24 years ago. This may reflect changes in child’s needs or existing knowledge about Rett syndrome over time (for instance, the development of greater genetic understanding of the syndrome in the last 15 years). A sense of not feeling alone when reading online peer support could cross age groups of interviewees, for reasons explored in more detail in Chapter 7. In terms of feeling there was someone one could talk to if one felt alone (emotional support measure for parents interacting with some carers exclusively online), this was only differentiated by age of child, with a higher proportion of parents of younger children more likely to agree. All other relationships were not significant, and a comparison by occupational groups could not be carried out.
5.5 Interpreting the structural constraints on the use of online support and information among survey respondents
This chapter set out to provide a context for understanding the use of the Internet in the everyday caring practices of interviewees. As such, it outlined how social differences among survey respondents were associated with differential use of the Internet and online support, and differences in benefits gleaned from these sources.
157 As noted in this chapter and the end of Chapter 4, the relatively small sample, due to the rare nature of Rett syndrome and lack of a comprehensive sampling frame, limited the kinds of analyses that could be carried out. Nonetheless, the data presented here provides an original contribution to existing data on the use of the Internet for support and information among parents of people with a rare syndrome. As noted in Chapter 2, existing quantitative data has either tended to explore use of the Internet among groups of carers of people with very different needs and length of time spent caring, or to focus on users of a specific forum. This research instead provides a snapshot of the use of the Internet among a large case study group of parents of people with Rett syndrome. As noted in Chapter 4, this sample is likely to under-represent men and over-represent Internet users and full-time carers. However, as also argued in that chapter, this may more accurately reflect how online support is used to inform the caring practices within a household. However, it does for the first time allow for the exploration of how structural differences in use among a wider pool of parents of people with a rare syndrome may constrain or influence the everyday uses of the Internet at a micro level. As such, this research can address the key criticisms of the literature outlined in Chapters 2 and 3, by presenting a coherent exploration of how structural differences interact with everyday caring and information-seeking practices among a case study group of parents of people with a rare syndrome. By exploring both aspects in a single piece of research, with parents drawn from the same sample group, it is possible to build a picture of how practices are related to structural differences without being deterministic or ignoring the impact of wider differences in how the Internet is used. The picture presented by the data here shows that among survey respondents, use of the Internet was similarly socially patterned as in the general population, with greater use among wealthier and younger groups27. The use of generic sources of online support and advice was high within the sample, with 83.7 per cent having ever used it. However, a striking difference emerged between these findings and digital inequalities data in the wider population and among carers, as summarised in Chapter 2. This was the low impact of income and education on the use of online information and support. It is possible, in terms of impact, that this
27 The impact of education could not be explored due to low cell counts.
158 may reflect the high proportion of carers within this sample but this still serves to demonstrate that among this group of respondents, different contextual forces are at play. As noted in Chapter 2, data on the use of online peer support is limited and, like the data here, cannot be used to generalise to a wider population of carers or of people with a rare syndrome. The data collected on carers (summarised in Chapter 2) has suggested that higher education and occupational status group is associated with greater use among these parents. However, this was not the case among this group of respondents, where use was highest among younger parents and parents of school age children, variables that were highly correlated. Years since diagnosis were also related to use, but not in a clearly linear way, with high use among parents of children diagnosed 20 to 24 years ago. As explored in Chapter 6, some parents of children diagnosed a number of years ago were using online peer support sites as a way of keeping informed about recent research advances and it is argued in that chapter, as within this whole thesis, that differential use of the Internet needs to be considered within the wider social, technical and research changes within which they occur. Similarly, while the recency of use of online peer support sites did not reflect a linear relationship with years since diagnosis, it was associated with lower use among older parents. This may reflect differences in Internet practices among older parents and the use of different sources of support, while also reflecting the existence of a group of parents of children diagnosed many years ago who are seeking up-to-date information on advances in research and potential treatment. These apparently conflicting influences on use are interesting because they reflect the situation of individual parents seeking information and providing care within the influence of a wider set of intersecting and constraining structural forces. This supports current findings that use of the Internet within wider caring practices cannot be deterministically predicted by a single demographic element, reflecting current approaches to ‘cultures’ of the Internet (Dutton and Blank, 2013) rather than structurally deterministic categories. It also appears to offer some initial support for Bourdieu’s (1998) argument for the potential for agency and choice within wider constraints, which can be challenged through engagement with fields (Bourdieu and
159 Wacquant, 1992), although the analysis of interview data will explore this in further detail in the following chapters. Use of all kinds of online platforms was differentiated by age, with greater use of all kinds by younger parents. This was mirrored in findings related to the age of the child with Rett syndrome and, to a lesser extent, to years since diagnosis. Differentiated aspects of Internet use (years used, mobile access and technical competence) also influenced use of these platforms, with greater competence and easier access particularly associated with greater use. As noted above, time variables (age of parent, age of child and time since diagnosis) were highly correlated and were associated with differential use of the Internet but their relative impact could not be differentiated through statistical analysis due to the small sample. Nonetheless - as argued in more detail in Chapter 6 - there is a value to exploring how these factors concurrently shape everyday practices and reflect a wider socio-historical context in the micro actions of individuals. An interesting finding was that blog use was greater among wealthier parents. As will be argued in Chapter 7, this is significant as blogs were considered as qualitatively different in terms of narratives, and conflict related to parenting practices. Finally, benefits gained from online support were mostly not differentiated by income or education, which runs counter to OxIS findings in information seeking in health more generally (Dutton and Blank, 2013). However, as noted above, this may partly reflect differences between information seeking and the seeking of advice or support, where more educated parents may value independent information seeking over advice and support seeking. This was an aspect of use that emerged in interviews and is discussed in Chapter 6, with parents drawing a distinction between primary and secondary information seeking. The exception to this finding was that gaining emotional support online was associated with holding a higher education qualification. This was a puzzling finding that is explored in more detail in Chapter 7. The impact of years since diagnosis on benefits - where a greater proportion of parents of children more recently diagnosed report informational and emotional support benefits - does reflect to a certain degree the findings of Leonard
160 and colleagues (2004), who found that younger parents reported greater benefits. Similarly, significantly more parents of younger children reported finding online support sites useful as places to speak to somebody if they felt alone. This could reflect both the relative lack of existing sources of support and the propensity for parents of younger children to avoid meeting older children with rare syndromes suggested in Gundersen’s (2011) research, an aspect also explored in Chapter 6. It was not possible to explore the impact of age of respondent on all benefits, but descriptive findings suggest (after Bourdieu, 1986) the greater value of the ‘goods’ available online to parents of children with a recent diagnosis, whose level of expertise is likely to be low. This is explored in the context of individual experiences of caring for a child with Rett syndrome in the following chapter, which emphasises the importance of taking into account the knowledge and expertise built up over time by parents, which is not adequately captured by the research reviewed in Chapter 2. Data on ever having posted on an online peer support site bears further exploration in the following chapters as this does not distinguish between posting for advice and offering advice, nor does it differentiate between having posted many years ago and more recently. The finding that differences in access to the Internet, self-rated ability and years of use were not related to ever having posted may be related to the higher level of competence, years of use and mobile access among those who do access all and particular forms of online peer support. In summary, despite the limitations of this dataset, it is valuable in providing a backdrop for interpreting the use of online support and information in wider caring practices. The practices of parents explored in Chapters 6 and 7 are interpreted using the knowledge that age of parent, age of child, years since diagnosis, use of mobile access, experience and online skill are likely to structure use in ways that may not always be apparent to interviewees. By combining these two forms of data within a single case study group I am able to explore the complex and dynamic interplay between these structuring contexts and individual practices. Chapter 6 explores the use of online support and information in the context of capitals, habitus and the socio-historical context within which they occur. Chapter 7 explores how the use of online support may both reproduce and challenge wider structural relationships.
161 162 Chapter 6. The contingent use of online support and information: the role of habitus, social and cultural capital, expertise and needs
The interview data presented in this chapter and Chapter 7 explore how the structural differences identified in Chapter 5 relate to differences in the use of online support and information in the wider caring practices of interviewees. This chapter explores the qualitative aspects of research questions two and three. This involved exploring the interplay between one’s own needs, practices, possession of cultural and social capital and habitus and the ‘goods’, practices and habitus perceived to exist in specific online subfields. The range of ages of interviewees and their children allowed an interesting cross-comparison of support and information needs at different life stages in a caring ‘career’ against a background of wider social, research and technological changes. As argued throughout this and the next chapter, parents’ use of online peer support sources was not static and fixed, but dynamic and responsive, influenced by their changing needs, the resources available to them and their accrual of relevant expertise and support sources. The first section of this chapter describes the interaction between the changing information and support needs of parents, the accrual of relevant ‘goods’ and sources of support and the contextual nature of the kinds of information and support available across online and offline sources. The second section narrows the focus to the differential use of online subfields of support and information. This involves an exploration of the role of habitus in differentiating between online subfields and alternative sources of support and teases out suggestions of the role of cultural capital in the choice between the use of peer and alternative sources of online information. This chapter closes with a summary of how this data has added to our understanding of the interplay between structural and micro aspects of online peer support use in wider caring practices.
163 6.1 Online information and support seeking in context: the dynamic nature of needs, expertise, support and biographical disruption over time
I have argued so far that a full understanding of the use of online support and information needs to take account of both structural differences in use and the interplay between individual habitus, capitals and everyday practices. As noted in the previous chapter, parents drew upon a range of online and offline sources to gain relevant information and support and use was largely differentiated by a combination of time-related variables (age of parent, age of child and time since diagnosis). However data from a survey carried out at a single point in time is unable to tease out how parents’ age, the age of their child and the time since diagnosis might structure their experiences over time, their need for information and their engagement with online sources of support and information. The interview data was instructive in this respect because it combined data from parents aged from 32 to 58, with children aged from 3 to 28, who had received their child’s diagnosis from within that year to 17 years ago. In the retrospective accounts of older parents and the contemporary accounts of younger parents, some key themes emerged in terms of similar kinds of information and support ‘goods’ sought at different stages in a child’s life and a carer’s ‘career’. These similar needs were embedded within dynamic and differing contexts, with changes in both the nature of knowledge and of mediums of support that reflected developments in the wider fields of medicine, research and technology, as described in Chapter 1. Finally, these accounts allowed for an assessment of how parents’ expertise grew over time with each new set of needs, making the ‘goods’ available on some online sources of support largely redundant, particularly when they appeared to be dominated by younger parents with less relevant expertise or ‘goods’ to offer. This section presents these findings in terms of how caring-related expertise and access to relevant social capital changes and accrues over time. Figure 6.1 outlines - in an illustrative and simplified form - the processes of accruing relevant
164 ‘goods’ and identifying useful social capital networks drawn from interviewees’ account. Each of the four parallel processes (care needs of child, biographical/illness narrative, possession of relevant expertise/ ‘goods’ sought, and social capital resources) represents a continuum, with illustrative examples given based on interview analysis. The changes in these parallel processes will be described below, but it is important to note three key points now. Firstly, that there is a change in terms of the information and support needed over time. Secondly, that these dynamic processes also happen within a dynamic context, with changing content of the available expertise within wider fields and changing modes of communication and social capital resources. This model is also therefore suggestive of the experiences of parents who did not have the Internet to draw upon at the time of their child’s diagnosis, or who had limited access. Finally, the model is, to a certain extent, an idealised version of interviewees’ accounts, which involved times of withdrawing from contact with peers, and renewed senses of biographical disruption with new health problems. The variation within the experiences of interviewees is described below. However it should be noted that the interviewees who participated were those who felt able to participate and are unlikely to reflect the full range of experiences of all parents of people with Rett syndrome, for instance among parents whose caring and work demands made participation impossible. However, the model has strengths in that it illustrates the dynamic aspects of carers’ experiences, the agency behind interviewees’ attempts to make sense of and address a series of unpredictable health crises, and allows for the accrual of expertise and networks over time and within the context of wider changes in society relating to technology, research and communication. The findings depicted in Figure 6.1 are discussed below in relation to the age of the person with Rett syndrome, rather than in terms of the processes. This is to demonstrate the interrelated nature of the parallel changes in all four processes over time.
165 Figure 6.1 Amassing expertise and social capital and repairing biographical disruption – parents’ changing needs over time
166 6.1.1 Early childhood Although some interviewees had had some contact with people with disabilities, either within their own families or as part of their work, none had any knowledge of Rett syndrome when suspicions developed about their child’s health and development or when a diagnosis was given (sometimes many years later). Mirroring Schaffer and colleagues’ (2007) findings, for some interviewees, this period of uncertainty before the diagnosis was spent researching the possible explanations for their child’s puzzling loss of skills, with the identification of Rett syndrome as a possible cause. However for other parents, the diagnosis or period of waiting for test results was the first time Rett syndrome was raised as a possible clinical diagnosis. This meant that for the majority of interviewees at or prior to diagnosis there was a lack of understanding of Rett syndrome and often, broader disability and related health problems, twinned with a lack of pre-existing connections to relevant social capital resources. Additionally, as with the ‘classical’ progression of Rett syndrome, most interviewees’ children had also been born without any obvious health problems, although this experience varied from family to family. For parents of older children, when diagnosis sometimes occurred later, this could involve two points of diagnosis, with Rett syndrome diagnosed later in their caring career. Interviewees’ accounts of the information and advice provided at diagnosis varied, and accounts tended to support suggestions by some commentators that local health professionals may lack up to date information relating to rare syndromes (Gundersen, 2011; Zaidman-Zait and Jamieson, 2007). For some parents the initial health input could be limited or could involve the communication of distressing, out-dated information.
our paediatrican had very helpfully told us she would be dead before she was eighteen
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago] Some interviewees described how the information and support offered by health practitioners felt inadequate, for example simply naming the diagnosis over the phone or suggesting parents look it up on the Internet.
[My daughter’s] community paed refused for a long time to actually voice her opinion on what she thought was wrong with [my daughter], kept saying delayed development!!!28 When me and her Dad refused to leave her office until she told us what she “thought” it was, she then said that she thought it was Rett Syndrome which of course meant nothing to us. She then said she had sent a blood sample from [my daughter] to GOSH for testing (no permission from us to do this!) and that in the meantime we should go home and look up RS on the internet!!! […] We had no support at all and no further contact with the CP. A few days later we took [my daughter] to her GP for a chesty cough and asked did she have the test results. The GP, shocked that no one has called us, said yes and promptly burst into tears after telling us yes [my daughter] had RS. Still no further support […]
[Interviewee #194, mother in her 40s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
All interviewees described a period of time when they felt a need to seek additional information about Rett syndrome. For some interviewees the distressing nature of the initial information they had gleaned from health professionals or initial online searches meant they delayed this process. However, when information seeking began, interviewees’ accounts showed a link between this need for information and attempts to comprehend what the diagnosis meant for them, their child and their family. This could be an uncertain and potentially overwhelming process, given the variability of health problems and severity of disability within the diagnosis of Rett syndrome. For a number of interviewees there followed a very intensive period of information searching online or from other known sources and a seeking out of any sources that might
28 This excerpt was from an email interview, punctuation left as in original email transcript. provide any broad advice and information, which again echoes Schaffer and colleagues (2007) descriptions of an intensive period of use of the Internet to understand the meaning of the prognosis for one’s child. In this research older parents described a similar reaction and how this was achieved before they had access to the Internet. This also suggests that the greater availability of information online is not necessarily the cause of this kind of information seeking among parents of people with rare syndromes.
but I, you know, I I wanted to read about everything […] and at that point, you had to kind of get copies of things that had been […] o- produced, so I had to, I got lots of copies of the papers from the Rett Syndrome Association and that kind of thing […] the Rett Syndrome Association at that time, which was the key place for information, really, there were, sort of contact families and things, so I remember ringing […] and having conversations on the phone, you know, that was really how people did it […] so you’d have a conversation on the phone and you’d ring another parent and you’d talk for three hours about, you know, whatever it was […] and certainly I spent a s’, you know, a certain amount of time talking to people on the phone at that time […] and would have, you know, online, if it had been there
[Interviewee #77, mother in her 50s of a 19-year-old woman with Rett syndrome, diagnosed 17 years ago]
Due to the array of information available, much of this information searching involved scanning through sources for anything that might be relevant in the future as well as what was relevant now. This was suggestive of the ‘expert’ or ‘informed’ patient role described in health research more widely (Bury, 1997; Nettleton, 2004b; Ziebland, 2004) and reflecting Giddens’ (1991) work on patients as ‘reflexive consumers’ and is termed ‘expert carer’ work in the context of this thesis. my husband saw an article, which he then reposted, which is this one, um, about some research that the Rett Syndrome Research Trust are funding […] and then I […] had a look, and listened to the interview. So I'll use it for that, for staying on top of what's happening with research or that sort of thing.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
During early childhood this could also include unearthing and seeking practical advice about adapted parenting strategies, for example, toilet training and communication or finding out about specialist equipment (for example to support drinking and communication, appropriate travel cots and prams).
As noted in Figure 6.1, interviewees tended to have few existing sources of relevant social capital, particularly with regard to Rett syndrome. Some interviewees were given information, the details of Rett UK, put in touch with other ‘Rett parents’ or were referred to (or insisted on being referred to) Rett specialists for further information. However, for other parents, no pointers to social capital resources were given and they had to find their own sources of potential support and information.
Um, when [my daughter] was first diagnosed, um, we weren’t given any details as such, we were just sort of told just to go and find our way [JH: Mm-hm] so um, I first contacted um, the American Rett people […] I didn’t even realise there was one in the UK [JH: Ok, yeah s’] So it was them that really I was in touch with first
[Interviewee #30, mother in her 30s of a 12-year-old girl with Rett syndrome, diagnosed 9 years ago]
It is difficult to find parents with Retts nearby. The parents we were informed about live about 45 miles away. [Interviewee #84, father in his 30s of a 3-year-old girl with Rett syndrome, diagnosed during the past year]
The sources of support used varied, reflecting the sources of known information available to the interviewee at the time of diagnosis, as represented in Figure 6.1. Significantly, this did not reflect a complete move from offline to online sources among younger parents, but more of a choosing among available, known sources. For instance, in all completed interviews where children had been diagnosed during the current ‘Participatory age’ of the Internet, interviewees spontaneously named at least one attempt to gain information or support from an offline source. Where parents of younger children had chosen to and been able to access a local group for parents of people with Rett syndrome, they found contact with parents of older children reassuring.
the first time we went to [a local Rett UK group] it was an evening one and […] it was just the parents and [my daughter] wasn’t that long.. diagnosed and um… what we got from that was [..] it was just a really nice, social, relaxed evening and we were just like, ‘these people have gone through this and they’ve come out and they’re ok,’ and they still go on holiday and they still have a life, they go to work, they have fun, they take their kids out on days out.. life goes on, and for us as an, when she was so newly diagnosed, that was, cos we uu- you can’t envisage what how much our life was gonna change and n what it was gonna be like and so, and we still can’t, but, to have met these families with a- all the older children to have come through what we’ve come through and life goes on and you can see that you know they’re like, ‘oh yeah, we went sk- skiing and – we actually didn’t ski because she can’t walk, but we put her in a sledge and she went down it, you know and and it was just like oh ok, actually life can be manageable, it’s ok, you know and that was amazing
[Interviewee #193, mother in her 30s of a 4-year-old girl with Rett syndrome, diagnosed 2 years ago] However, some available forms of support involved face-to-face contact with other parents and their children with Rett syndrome, for instance Rett UK’s family events. For some interviewees with young children it could be challenging to meet older children with Rett syndrome at this early stage of biographical disruption.
Um and I remember back in those days meeting a family with an older child and in hindsight it was a mistake. [JH: Right.] I needed to meet some people with children my own age. [JH: Mm. And why why was why did you feel it was a mistake?] Because you just focus on what that child can’t do. [JH: OK.] And you know you think that that’s your child’s future. [JH: OK.] You don’t focus on what the child or the parents or the person can do. [JH: Yeah] Your instinct is to focus on what they’re not doing at that age. [JH: Yeah.] And when your child’s 18 months old, you don’t really need to know that.
[Interviewee #25, mother in her 40s of an 8-year-old-girl with Rett syndrome, diagnosed six years ago]
This meant that for some parents, such potential sources of peer support offline were avoided at this stage.
Um, we've, because we're members of Rett UK, we've been invited to the family days, which we haven't gone to. And part of the reason we haven't gone, is because... I feel like... such a tangible reminder of our future is quite hard for us to deal with? [JH: Ok, yeah.] Um, like we took [my daughter] to the Rett clinic in Guys and St Thomas in London and weeee.... er, we really wanted her to go, we wanted the specialists to see her […] but obviously in the waiting room there's a lot of little girls in wheelchairs with feeding tubes. And my little girl is walking around, perhaps not very well and she can't talk and she can't use her hands. But she's not in a wheelchair with a feeding tube and that was really hard. [Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
This was a similar finding to Gundersen (2011), whose interviewees found it too difficult to face other children with the same rare syndrome, but they also found meeting other parents of children with the same diagnosis in the early stages difficult, which not all parents in my sample reported. However, even at this early stage, some of the same parents were already building networks of parents they felt they could call upon for advice.
Um... a-a- I have - in the last sort of six months or so, built up more of a... a -a - not a support group, because I don't know anybody very well but - set of contacts of people that I could probably contact [JH: Yeah] Um, I've got telephone numbers for people living in the area whose daughters have Rett syndrome and that kind of thing, so I feel more like I could call somebody if I had a specific question.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
About half of interviewees’ first contact with online peer support sources came through recommendations from offline, existing sources of social capital, such as work (within disability services), a health professional, parents of people with Rett syndrome or a Rett syndrome charity. The remainder accessed these sources through online searches. Interviewees and survey respondents were often unaware of the full range of online sites and groups offering peer support. One parent, whose child had recently been diagnosed, had only just discovered the Facebook Pages of two charities, which tended to have an organisational focus rather than offer peer support29.
To be honest, I've never used a parents’ forum. Not because I have anything against them particularly, but I've just never come across one.
29 This aspect of Facebook Pages is discussed in greater detail in Chapter 7. [Interviewee #84, father in his 30s of a 3-year-old girl with Rett syndrome, diagnosed during the past year]
In summary then, for interviewees the period of time around receiving a diagnosis of a disability or of Rett syndrome was marked by a lack of relevant expertise and the initial experience of meaning making from an often striking biographical disruption. As argued above, at this stage interviewees sought new sources of available social capital and often embarked upon an intensive search for information as part of trying to make sense of the diagnosis and what it meant for them and their child, echoing existing qualitative findings (Schaffer et al., 2007). However, as noted in Chapter 2, the majority of findings relating to the use of the Internet and peer support among parents of people with rare syndromes excludes parents of adults. As my sample included parents of older children and adults, it was able to shed new light on how information seeking practices changed over time and in response to changing needs.
6.1.2 School-age to early adulthood Interviewees discussed how the age of their child was often associated with facing particular health needs, although individual health experiences could vary widely overall. This meant that some parents of children of similar ages could be looking for information about particular types of health problems.
like I say, they’re they’re all similar ages to [my daughter] so we’re all kind of going through the same, the girls are going through the same stages so like onset of seizures, gastrostomies, scoliosis, starting schools, communication strategies, they’re all kind of like going through the same stages
[Interviewee #193, mother in her 30s of a 4-year-old girl with Rett syndrome, diagnosed 2 years ago]
As children got older, the number of new health problems tended to reduce slightly, although again there was a great deal of variation. For some parents, this meant that online information seeking narrowed to focus on information about any new health problems as and when they arose.
I think what’s happened for us, things have changed with [my daughter] and so I’ve trawled some of the sites perhaps I haven’t been on for a while to get more updated information, cos we’ve never had to worry about epilepsy, so I’ve never particularly looked at that for her condition but she might now have it, so that’s why I’ve been trawling things I’ve looked at before specifically for that
[Interviewee #28, mother in her 50s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
The work of understanding the meaning of the diagnosis and trying to gain information about likely prognosis continued for some parents in information seeking about similarities among girls with the same genetic mutation.
but also there’s other people on there, um on [a particular site] that have been able to understand some of the mutations that the girls have got, so that was quite nice, um, a couple of months ago, people were posting on their girls’ different mutations so it’s nice to see who’s got what mutation and how the girls, are similar [JH: Oh ok. That’s that’s interesting, so did did you find something relevant to to you and [your daughter] on there?] Yeah I mean I found a couple of girls that um had the same mutation and at the same time found that they looked very similar [JH: Oh really?] Kind of like people with Down’s Syndrome look similar [JH: Yeah] it’s really peculiar to see some of the girls with Rett’s that have various similarities and you know have gone down the same path as, you know, developed epilepsy, scoliosis, you know [but] none of them develop, developed sleep apnoea…
[Interviewee #30, mother in her 30s of a 12-year-old girl with Rett syndrome, diagnosed 9 years ago] Parents’ use of online forums and other sources at this age-stage tended to focus upon interpreting new symptoms and behaviour, discussing and weighing up of different treatment options and on the daily management of health conditions. Examples included: the benefits and disadvantages of different drug combinations for treating epilepsy; the management of scoliosis and reality of spinal surgery; and the benefits of dietary changes. As such, they reflected the kinds of discussions described in research based on the analysis of posts on online forums for disabled children discussed in Chapter 2 (Huws et al., 2001; Jones & Lewis, 2001). However, the use of interviews here allowed an exploration of how these uses fitted into the wider context of parents’ lives and their children’s needs. Parents also continued to seek and use advice about relevant daily caring strategies and equipment for older children (for example communication aids, wheelchairs, splints, bibs and sleep systems30).
the daily struggles are sometimes harder than the larger medical ones, daily challenges of eating, sleeping, crying, screeching, so its the daily challenges and ideas/solutions to this is what is covered.
[Interviewee #194, mother in her 40s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
Parents at this stage still used a ‘horizon scanning’ approach as ‘expert carers’ keeping abreast of recent developments and therapies that might benefit their child, thus maintaining a certain broad focus in their information searching by scanning through preferred sources of information.
[JH: What is it that you go to these groups for, or look out for, or find most interesting on these pages? (Lists popular sites used)] Same answer for all 3, info on events, developments in the RS world, reading about family experiences, photos. When you have a child with RS, you want to know you have a lot of areas covered!
30 Sleep systems are supportive structures that aim to improve or maintain reasonable posture for children with spinal problems. [Interviewee #194, mother in her 40s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
This description is particularly evocative of the felt imperative to remain informed that was described by Ziebland (2004) and quoted in Chapter 2.
For interviewees with slightly older children with Rett syndrome, particularly those who had experienced greater health problems earlier in their childhood, the likelihood of facing novel health problems had decreased markedly.
but I also think that my child is old enough and established enough that there isn’t actually anything else Rett-wise that’s gonna kick that we haven’t already got, you know, she’s not gonna start breathing dysfunctions or having seizures or spinal curvatures or you know, swallowing issues, or or hyperventilation or or we we’ve already got all those things, there isn’t anything else coming, it, there there isn’t any more regressions to come
[Interviewee #174, mother in her 40s of a 14-year-old young woman with Rett syndrome, formally diagnosed eight years ago although mother realised 12 years ago]
This narrowing of information searching could also be related to a change in approach, a move from understanding Rett syndrome as a whole and its meaning for the family to a more practical, targeted approach.
the symptoms are the same all over the world, but I prefer the support and, what I can get to help us […] which obviously is, is a localised thing so it didn’t, you know the worldwide things just really didn’t um, interest me, as much. In the beginning they did because you’re after every bit of information you can get, but now I don’t need that […] I think you get to the point where you could read every medical symptom in the world but it’s not actually gonna change anything. [My daughter’s] still [my daughter] and I can read every email under the sun, it won’t actually make her any better, um, what will make her, have an easier life is if I can find out, is there anywhere local that does riding for the disabled, or or that side of things I found, more helpful
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
A number of parents of schoolchildren talked about moving away from the initial ‘shock’ period, where emotions were higher, but of still experiencing some feelings of grief that were less foregrounded.
And I think erm particularly, when recently we’ve had a few families who’ve just got a new diagnosis and they’ve got particularly young children, sometimes it does bring back the emotions. Cos our daughter was quite young when she was diagnosed and it’s the emotions are still there in the background and it can bring it back to the surface which is not really probably always a bad thing either. [JH: OK. What what’s positive about that then?] Um well to be honest sometimes I think if you try and hide grief, that’s all you’re doing. Um it’ll it’ll never go away and sometimes it will come to the surface and I think it’s how you deal with it. And accept that it probably always will be there as long as it’s not always at the forefront and it’s not constantly there. Short episodes, to me, are normal […] and if you’re empathising with somebody else.
[Interviewee #25, mother in her 40s of an 8-year-old-girl with Rett syndrome, diagnosed six years ago]
For one interviewee it was a case of ‘keeping going’ – against a fear of not coping with everything the diagnosis entailed.
I’m very much generalising here, um there’s two distinct groups. Those who are driven to making their lives the best they possibly can for the disabled children and those who’ve just - and I totally understand this - have just had enough and have given up. [JH: Yeah] and can’t cope and are just ground down by the system, by the child, by everything, by the lack of support, and my heart goes out to them but I can’t be one of them. I can’t, I can't ever let myself go there. I can see how you can get there, my dread is to get there, er and sometimes I keep going too much because my fear is that if I stop I’ll just collapse and will be one of them [laughs]
[Interviewee #86, mother in her 40s of a 13-year-old girl with Rett syndrome, diagnosed 11 years ago]
Interviewees with school-age children continued to build wider relevant social capital networks (including online and offline contacts) and to establish a set of trusted, reliable contacts. This could involve a period of active social capital building, making connections with as many other ‘Rett parents’ or useful organisations or people as possible, then a narrowing down to parents or organisations that could offer more in terms of relevant information, online and offline.
I think over the years – I guess things have changed for us […] I used a lot of things when she was smaller [JH: Yeah]. I think trying to glean information or – different things, but once she started at school and we had our diagnosis, things changed greatly u-u-and then I then homed in more on, say Rett UK because my specifics I could get from them and I’ve only perhaps used Carers or Contact a Family for more work-related things than anything else I think really.
[Interviewee #28, mother in her 50s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
Through, just through Facebook, um, you get sent Friend requests from people who know other Rett people and [JH: Oh ok] and that’s how it, how it went on and in the beginning of Facebook I accepted requests from everybody um because it was always, hey you’ve got to have as many friends as you can [laughs] [JH: (laughs) yeah] and [laughs] um I have got rid of lots, I had lots and lots of American, mums um, which I’ve got rid of a majority now, only the ones I’ve only kept, are the ones who I have some form of contact with and their systems and the way their benefits run and their their medical aid are completely different to us, so we really don’t have anything to discuss that’s in common with with us at all, other than the symptoms [JH: Yeah] Um, but yeah sometime, you know, the same, you might see the same names keep cropping up on other people’s posts and you you’ll send Friend requests and, yeah I’m a lot more picky [laughing] these days
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
Among this group were parents who had not received a diagnosis during the ‘Participatory age’. For some of these parents, the reliance on certain media tended to ‘stick’ along with the use of particular sources. This was also related to a certain form of ‘digital taste’, which is explored in section 6.2.5.
I sometimes just feel I need to speak to someone actually, you know, a conversation rather than… I know it is a conversation by the group, but I, I don’t know, perhaps it’s old habits die you - uh – whatever that saying is um just because in the early days when we were first using Rett UK, they didn’t have a Facebook page and there was no Twitter and all of that and so you just had to pick up the phone and I guess that’s, so for me I’m a bit of a creature of habit I suppose
[Interviewee #28, mother in her 50s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
For some parents of slightly younger children, this could involve taking offline some relationships formed online or into a private online correspondence31. This
31 Such as private messaging on Facebook, which cannot be seen by other users outside the conversation. could involve some element of establishing similar taste or parenting practices – a theme that is picked up in greater detail in section 6.2.5 on the role of habitus in choice of online subfield.
one of the things I, you know, yeah wanted to get across in this was that.. online support, has been great but actually it then morphs into friendships with a few people, which is sort of where I am now […] I now have identified, the people that, you know, I, that I get on very well with and now, we don’t do it on forums, you know, we text, or we email or we meet up[…] so yes, it very much hasn’t stayed online
[Interviewee #76, mother in her 40s of a 5-year-old girl with Rett syndrome, diagnosed 3 years ago].
The impact of changes in the Internet was obvious in this group, who had used some of the earlier forms of support, such as email groups. Some of these parents found existing support sources were ‘migrating’ to Facebook and other kinds of groups were closing due to lack of use or concerns about security and they followed these sources to their new platforms.
6.1.3 Adulthood The health needs of interviewees’ children plateaued in adulthood. However this may reflect the parents who were available to participate, who may have had healthier children. Nonetheless, among interviewees, there were few novel health issues to navigate.
the other thing, is that that we don’t need as much of of what that was now anymore because we’re kind of in a place where, [my daughter’s] older and it’s easier to to know what you need, there’s just not so many needs really […] they’re more social needs more than medical needs now
[Interviewee #132, mother in her 50s of a 28-year old woman with Rett syndrome, diagnosed 17 years ago] Interviewees with adult children had far fewer information needs than parents of pre-school and school-age children. This was partly due to a much higher stockpile of relevant knowledge. Parents of adult children talked in interviews about providing information to parents of younger children through various mediums and having less need for information and support themselves.
I tend to have been there, done that a bit, you know so so therefore I’m the font of knowledge rather than looking for the knowledge now you know? So um you know it’s it’s so there’s uh less need to find out about things actually
[Interviewee #132, mother in her 50s of a 28-year old woman with Rett syndrome, diagnosed 17 years ago]
Most older parents noted that those posting on online support forums tended have younger children, who were experiencing different issues.
Well, it’s like in Mother and Baby groups, isn’t it? [JH: Yeah, yeah] You wouldn’t have like the babies, and then you’d have a 10 year old there. (Laughter) [JH: Yeah.] It’s just a completely different thing, isn’t it? You know? [JH: Yeah. Yeah] It’s the ages, and everything in common I think.
[Interviewee #133, mother in her 50s of an 18-year-old woman with Rett syndrome, diagnosed 16 years ago]
This meant that the ‘goods’ that parents of older children could access in online support sites were limited in terms of information about caring and health strategies. However, parents of adult children still sought advice about new equipment (examples included use of iPads and communication equipment) and kept abreast of new therapies, which was achieved by parents both online and offline, for instance through Rett UK’s newsletter. Yet for some parents, adopting newer developments in communication, such as eye-gaze, was not straightforward with adult children.
I’m really kind of interested in things like eye-pointing and things like this, but again you have to see it in context, you know, it’s great, e- eye-pointing would be great, and if it’s beneficial for [my daughter], that’s great, but we have spent an awful long time finding communication systems that work for [my daughter], um, of which, I wouldn’t throw out the window, now, just for another system, you know so um [rubs hands together] we’ll wait and see
[Interviewee #132, mother in her 50s of a 28-year old woman with Rett syndrome, diagnosed 17 years ago]
Nonetheless, this group of interviewees were still engaged in expert carer work. This also reflected Schaffer and colleagues’ (2007) finding that parents of children with the rarest conditions in her sample continued to stay abreast of research while other parents tended to reduce this activity over time. However, it should be remembered that interviewees were recruited due to their active of use online peer support, so these information-seeking activities may not reflect all parents of people with Rett syndrome. Expert carer work involved both scanning for anything that might be useful for their child and staying appraised of developments in research. Research breakthroughs were monitored by interviewees with adult children through online sources, which were perceived to be the best and most up-to-date sources of such information.
I’m only really keeping an eye on it so that I don’t miss, major developments. So what would I click into, I’d click into something where they were talking about a new drug treatment, or they were talking about some kind of breakthrough, then I would probably go in and read it. Most of the time I’d just delete it
[Interviewee #77, mother in her 50s of a 19-year-old woman with Rett syndrome, diagnosed 17 years ago] Interviewees with older children tended not to be actively building their social support. For instance, when I asked one parent of an adult child about seeking advice and support, she made it clear that she had existing, trusted networks she could now rely upon.
you see, I’ve got a really good support network for my daughter now. Cos she’s um, she’s partly residential in a residential school with great nursing and really good teaching and excellent care. I’ve got a whole network of people to share my concerns with there.
[Interviewee #77, mother in her 50s of a 19-year-old woman with Rett syndrome, diagnosed 17 years ago]
When seeking new connections was mentioned by one interviewee with an adult child, it was about engaging with others either to offer help or to participate in fundraising activities, rather than seeking support.
I quite like to do these um fund-raising events and I always find out what other people are doing. Like last year I discovered quite a few people are taking part in the 10k run in London. So I decided to join them (laughs). So that’s quite good to find out what other people are doing and then do it with them.
[Interviewee #116, mother in her 50s of a 20-year-old woman with Rett syndrome, diagnosed 17 years ago]
The need for support with coping with the biographical disruption of having a child with Rett syndrome seemed to be lower among parents of adult children than among other interviewees. Three interviewees described having reached a level of ‘acceptance’, but of this also being related to their current situation with their daughter. I know people go through different stages at the different stages of caring. I’ve sort of um come to the third stage of acceptance. I think my emotional needs and things like that have um sort of quite settled. I think in the first phase, like it’s you’re in shock and […] I think that’s the time when you really need to talk to other people to share your emotions. I think that time has passed for me anyway because my daughter is now 21. I’ve been her carer for 21 years, so I feel quite settled. Occasionally I do want to share my feelings, especially as my daughter is getting older. I think I find it easier, well I think I need to talk to parents of my age really, because they are in a similar situation. [my daughter] will be leaving college in 2014 and then what do I do then?
[Interviewee #116, mother in her 50s of a 20-year-old woman with Rett syndrome, diagnosed 17 years ago]
us, s, who have got older children now don’t have, you know, we’ve we’ve got the grief, yes but we’ve got the acceptance and the getting on with it, really and actually it does, Jo, get easier, um you know, once you’ve accepted that, y-you’ve got this severely disabled, child, um actually, because they’re not, you know, they’re not regressing like they are in childhood, it does get easier.
Interviewee #132, mother in her 50s of a 28-year old woman with Rett syndrome, diagnosed 17 years ago]
This decreased need for support from other parents was something that carried over into the use of online peer sites for support.
I did feel the need for that, earlier on I felt the need for that when those things [online peer support groups] weren’t there and I found other ways to get that so I joined, I joined um contact groups, I was part of the Rett Syndrome Association, I deliberately went to meet with other parents, I went every year to a family weekend because I, once a year I wanted to spend time with, so I did those things, because that was what, so I obviously, I obviously, you know, would have benefited from this, you know at that time, it’s just that by the time this has come, I am less needy in that respect, I suppose.
[Interviewee #77, mother in her 50s of a 19-year-old woman with Rett syndrome, diagnosed 17 years ago]
However, having gone through a stage of seeking support was not universal in this group. A couple, who were interviewed together told me that they had never really felt the need to join any kind of support group.
And as [my husband] said, I don’t know whether we’d want to be just a group of Rett parents with Rett children. [JH: No. Yeah] Um I mean, you may be able to give each other a bit of support and there may be times where they say, “Well actually, we went to see this doctor”, or, “We went to this clinic”, or “We found out that you can like benefits and things”, but apart from that, I think it might be a bit…of a moan and an, oh dear. [JH: Yeah, yeah] You know so. [Husband of 133: I guess one thing is, we don’t feel sorry for ourselves.] No [laughs] [JH: Mm. Mm.] [Husband of 133: We never have.] No. We’re very positive, and – [Husband of 133: Don’t want to.] No. […] And I know it must be hard for some parents, because it does affect people in different ways, doesn’t it? [Husband of 133: Mm] But, erm, I think because we’ve always worked as well, so you have to get on with it, don’t you?
[Interviewees #133 and #133-H, parents of an 18-year-old woman with Rett syndrome, diagnosed 16 years ago].
On the edges of these parents’ accounts were references to other parents who had not managed to overcome the biographical disruption involved in having a daughter with Rett syndrome, so the accounts related here may only reflect the experiences of interviewees who felt able to participate in my research. and you’re gonna get some strong mums who... buckle […] the mother [of a girl with Rett syndrome I know] had got so distressed, she’d run away, they didn’t see her for five days, they didn’t know where she was, she couldn’t cope, that’s not a bad mum, that’s not a bad person, that was someone who cou- - and she still to this day can’t cope, the father can and the rest of the family all mucks in, that mother has never ever accepted um that child.
[Interviewee #174, mother in her 40s of a 14-year-old young woman with Rett syndrome, formally diagnosed eight years ago although mother realised 12 years ago]
Despite some variability in experiences, and the difficulties with recall associated with retrospective accounts, there were enough common crosscutting themes across parents’ accounts to be suggestive of a far more dynamic process than is normally depicted in research about carers’ use of online support and information. These processes were outlined in Figure 6.1 and show the role of parents’ agency in seeking support and information at different times, while also accounting for the relevant sources of social support and expertise accrued over time. This process is suggestive of Bourdieu’s description of the contingent nature of seeking ‘goods’ of value in different social capital sources (Bourdieu and Wacquant, 1992). The next section focuses on how the use of online support subfields relate to these accrued levels of expertise and social capital and also draws out aspects of individual habitus that appeared to influence the use of specific online support subfields.
6.2 The influence of habitus, cultural and social capital on interviewees’ ‘fit’ with specific online support subfields
This section explores the impact of differing levels of relevant caring expertise and social capital with regard to their impact on an individual’s use of specific online peer support subfields. As described in Chapter 2, this is a much neglected area within current research, which tends to talk about all online peer support as a single entity or focus on use of a single forum. As suggested in the previous section, parents’ stockpiles of relevant expertise and connections to trusted social capital resources appeared to develop over a caring career. Yet interviewees also possessed pertinent cultural capital that had the potential to differentiate their use of different sources, specifically having accessed research training in higher education courses that helped them to interpret primary research papers. In addition, interviewees also had access to other forms of social capital, which varied in terms of its appropriateness for certain forms of advice, support and information. It is therefore argued below that a clear understanding of differences in engagement with online peer support sources needs to consider the wider context of existing cultural and social capital rather than describing the use of online support and information in isolation.
6.2.1 Relationship to existing social capital resources Clearly all interviewees had had some contact with online peer support forums, so their accounts did not reflect the views of parents who did not seek out such sources of support. The existence of an alternative approach was suggested by the comments of one respondent to the survey, who rejected the need for any kind of peer support where good family support was available.
I have a great family network around us and we are not a family in crisis or need. We are a normal family doing things our way. We all muck in together and our daughter […] is the most delightful young lady you could wish to meet.
[Anonymous survey respondent]
For some parents information would be sought online, but support during difficult times was only sought from friends and family. [JH: Yeah. Um and so when you need help where what are the sources of help that you you would tap into?] Um, probably my my family. [JH: Yeah.] And close friends.
[Interviewee #25, mother in her 40s of an 8-year-old-girl with Rett syndrome, diagnosed six years ago]
However, some parents described how their own family’s reaction to their daughter’s diagnosis made it difficult for them to provide the support they wanted, or their understanding was limited.
With family it's more difficult. (Sighs). […] on the one side, on my mother-in- law's side, they're so caring and they're so lovely toward her, but they want to pretend it's not happening. [JH: Yeah] So, if we send them stuff, they don't read it […] On my parent's side [JH: Mm-hm] They're not nearly as loving or caring [JH: Mm-hm] but they sort of... feel like it's happening to them [Me: Ok. Yeah.] And then that's not helpful to me because it's not happening to them, it's happening to us.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
Although most interviewees had at least some good support from their family network, there could be limitations – for these interviewees – to what that support could offer.
Cos it’s, you know, having a child with Rett syndrome is a really lonely thing, can be a really lonely thing because there’s nobody much around that you can share that thing with, so you know, you’re often thinking, well you know, what what what do I do with this, what do I do with that and where whereas with a normal child, you know, you’d ring your sister and say, you know d’ was so-and-so like that when they were teething, you know, you’d have that kind of conversation, you haven’t got a frame of reference to do that with, so it can be a really lonely thing.
[Interviewee #77, mother in her 50s of a 19-year-old woman with Rett syndrome, diagnosed 17 years ago]
Interviewees also spoke about how, although friends could be very supportive, it could be difficult for them to understand what it was like to look after a child with Rett syndrome, or they worried about alienating them.
Yeah, cos yeah, although yeah, some of my friends are lovely and would do anything for us you can’t actually really talk to them about how you feel because… they don’t und, they would never understand, I wouldn’t have ever understood until you’re actually in that situation.
[Interviewee #83, mother in her 30s of a seven-year-old girl with Rett syndrome, diagnosed 5 years ago].
I think if you... spend a lot of time complaining to your friends then quite soon you don't have any.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
However, the progression of her child’s health problems meant that one interviewee identified more with parents of children with severe health problems or disabilities than with other parents of people with Rett syndrome. In this case, the young woman with Rett syndrome also had an unrelated heart condition.
our respite has been hospice, um, right from little, because of her ill health, um, my my friend down in [another area]’s just lost his boy with muscular dystrophy at the age of 23. We had more in common because our children both had health issues than me and say another Rett girl in this area that’s this big and walking and has just their hands, see, ‘just’, see again, [JH: yeah] ‘just’ lost the use of her hands and speech because, oh to be back to that!
[Interviewee #174, mother in her 40s of a 14-year-old young woman with Rett syndrome, formally diagnosed eight years ago although mother realised 12 years ago]
Some parents with established networks of Rett parent peers preferred to communicate with those parents privately, rather than through groups. This could reflect having pre-existing links with those parents or establishing friendships online that were later taken offline.
but the people in the Rett community that I really want to be in touch with I’m in touch with them anyway either by email or phone or – I mean – yes, there are a couple of families it is only via Facebook, but not necessarily via that [online peer support] group […] I guess unlike some I’m in an enviable position, I like to think, [JH: Mm-hm] in that, um, for [my daughter], there was – there were two older girls with Rett syndrome at her school [JH: Oh, really?] So I’ve always been able to ask those mums anything although they’ll get – all the girls are different, you, you know [JH: yeah] and because, um, I suppose also because of [being involved with the local] support group, and knowing other families actually I haven’t felt the need to ask the questions and I know other families around the country that I would probably ring rather than post something.
[Interviewee #28, mother in her 50s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago] So yeah, so I think that um, there’ve been times where, where that forum has been very supportive and maybe there are people who still find it so, um but I I’ve felt like I’d just sort of got to the end of that particular road, as I say, I had, partly through it, um, had, you know, made e- found my own network my own group, you know I have some, fantastic Rett friends and, that’s it, you know, they’re my friends, I’ve, you know, we’ve we we have had lots of online interactions but we’re now friends offline.
[Interviewee #76, mother in her 40s of a 5-year-old girl with Rett syndrome, diagnosed 3 years ago].
Even among younger parents, certain trusted sources of both online and offline information were seen as preferable to online peer support.
I had a friend who said, 'oh you should go and look at Mumsnet' (typing sound) they've got a Special Needs area... um.. let's see if we can find it... […] but you see what I mean? […] see I probably wouldn't look at any of these things because I would think that... what's Mumsnet going to know about the DLA that I can't get from Cerebra [local organisation] who are specialists in it?
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
Finally, a number of interviewees talked about overlaps between the kinds of information within different online peer support groups. This meant that if parents were already using one particular group, they might not feel the need to join another one.
I’ve been added to one recently but I’ve I’ve looked at it but it’s not different to the one that I’m already in so I I don’t really see the point in [inhales] in being on all of them. [Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
This comparative use of multiple sources of online support is neglected in the current research, which, as argued in Chapter 2, tends to reflect the use of online support overall or the use of a single group, rather than the choices made between alternative online groups. Together these findings suggest that the use of online peer support should be considered as part of a wider and shifting constellation of possible sources of support, which are weighed up for the ‘goods’ they can provide at a particular time in a parent’s caring career.
6.2.2 Cultural capital and differences in propensity to seek help in peer support forums As will be remembered from Chapter 5, education level – a proxy for cultural capital - was not significantly related to ever having used online peer support. However, within interviewees’ accounts, the role of online peer support as a primary source of information appeared to hold a different status depending on level of qualification held. This emerged from fourteen interviews, where interviewees described having preferred sources of information when they needed to research something new related to caring for their daughter with Rett syndrome. All four interviewees with a basic or secondary level of education described posting on a forum as a primary source of advice.
I tend to go there first. Um I posted I posted a a post recently [about puberty] […] and uh, I just wanted some advice and because I have quite a good rapport with a lot of the parents on in the group, kind of you know you’re gonna get sensible advice and it’s not all doom and gloom and people inject some humour into it and it you just feel a little bit better about it.
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago]. However, while interviewees from all educational groups had posted in forums asking for advice of various kinds, none of these interviewees described an online peer support site as their primary method of finding out new information, if they described having a preferred method at all. Five interviewees with a higher education qualification described how they would try to research something themselves first before asking a question on a forum, using a range of strategies including Internet searching, ‘expert carer’ scanning of blogs, contacting known Rett parents offline and, for one parent, reading journal articles.
Um... I mean I’m quite good at researching anyway, so I probably would go off and research it myself […] [JH: yeah yeah and so whe- when you, when’s the point that you would go online into a group and ask (…) people about something?] Um [JH: or would you tend just to look at it rather than post?] Some, I mean very occasionally I do [JH: Mm] I d’ e’ I don’t tend to ask questions.
[Interviewee #83, mother in her 30s of a seven-year-old girl with Rett syndrome, diagnosed 5 years ago].
For some parents with a higher education qualification, online peer support sites could be used to narrow down the focus of a search.
I mean you could Google but you’d end up sort of all day with the amount of stuff that is out there, but whether it’s actually, of any use or or or whether it’s NHS-funded, things like that obviously so it just seems to be, it seems to be a helpful way of finding out what is available [JH: yeah, qua’, more quickly and] yes [JH: access other parents who know] Yeah. […] I mean sort of can you advise on a mattress so you know unless, u’ unless you know what you’re looking for it’s sort of needle in a haystack so it’s all very, help, everyone’s helpful. [Interviewee #83, mother in her 30s of a seven-year-old girl with Rett syndrome, diagnosed 5 years ago].
For another interviewee with a higher education qualification this was combined with scanning sites or groups for information, where the use of online peer support was seen as a last resort only.
Um, if I’m posting it means that I’ve already read a load of stuff and I can’t find it anywhere. [JH: OK. Yeah.] It’s my last resort. [JH: OK. Yeah.] Er it wouldn’t be my first option. [JH: OK] Um, whereas some people probably can’t be bothered. Um I I just like to know I think, have some knowledge to base it on before I go in and ask the question. But yes, it would be, it would be, the bottom of the list to then do a posting. So that’s the difference for me, the other bit is is scanning for information and at first um and seeing if I can get that from people who’ve already posted.
[Interviewee #86, mother in her 40s of a 13-year-old girl with Rett syndrome, diagnosed 11 years ago]
However, even among parents with a higher education qualification, a lack of specific medical knowledge meant that reading other parents’ explanations of current research on peer support forums was a helpful way of interpreting it. This suggests a form of bridging social capital at odds with Bourdieu’s conception of social capital, which provided democratic access to ‘goods’ by any parents using a forum.
I want support and I want knowledge um you know and some people do an awful lot of research and obviously h-have a brain that can understand a lot more biology than I can and I appreciate that time and effort that they take. So that’s what I want out of it […] [JH: Yeah, OK. So that’s that’s really interesting so you that that there are some people in the community who will kind of gather up and kind of digest and present the research.] They haven’t got a medical background, but they seem to be able to search out the information and digest it and bring it to the community.
[Interviewee #25, mother in her 40s of an 8-year-old-girl with Rett syndrome, diagnosed six years ago]
However, as described next, very knowledgeable parents were sometimes circumspect about what they would share online, suggesting that access to this kind of bridging capital was limited by parents’ willingness to share ‘goods’ in online support spaces that did not offer them commensurate rewards, an approach more reflective of Bourdieu’s conceptualisation of the goods of social capital resources being available only to those with commensurate cultural capital.
6.2.3 Willingness to share cultural capital in peer support forums Most interviewees described a willingness to respond to other parents’ posts asking for support and information, but only if they felt they could add something new or had relevant experiences to draw upon.
I will just, add some information if somebody’s looking for something, um, so maybe say, ‘oh, yes my daughter had that problem at that age, but she hasn’t got it now,’ or, ‘this is what we’ve done for that’, that sort of thing.
[Interviewee #28, mother of a 12 year old girl with Rett syndrome]
However, for parents who had preferred alternative sources of support, the investment of time in online forums was seen as having less benefit than using it as part of an exchange to build social capital in spaces where they had existing online relationships. For example, one parent who blogged also only tended to respond to other bloggers’ posts [JH: Um, have you ever posted on a forum other than the blogs?] No. [JH: Mm. What what puts you off from posting is it, you] Time? [JH: Yeah. Mm-hm. Yeah] I think yeah, I I… I f-fully appreciate it might well be useful to other families, we say[?], we used this bit of equipment and it worked really well however this, blah blah blah and the kind, to have the conversation I’m reading, but, it sounds really selfish now, there’s nothing in it… for me to do that, then you’re not gonna a get a response, you’re not forming a relationship with anyone you’re not.. really getting anything off your chest, it’s not talk- – and I just don’t have time, I w- to do to be that… unfocused on what I’m on the Internet for really.
[Interviewee #193, mother in her 30s of a 4-year-old girl with Rett syndrome, diagnosed 2 years ago]
Given the finding that parents blogging and reading blogs were found to be more wealthy and educated than those who used Facebook groups (as was the case with this interviewee), this is a particularly interesting finding. However, as she wrote a publically accessible blog, including searchable terms, it is arguable that this information is available to others. Yet, as found in the survey, there was evidence of a greater proportion of blog reading among wealthier respondents. This meant that this interviewee might only be sharing her expertise within a group of like peers32. Although this was not through a deliberate intention to exclude, it did appear to reflect Bourdieu’s (1986) argument that people tend to find themselves among homogenous others in certain social spaces, which is explored in more detail in the next subsection. The final two sections of this chapter explore how the fit or disparity between personal taste, practices, and habitus interact with the habitus of individual online support subfields over time.
32 This could only be definitively confirmed through a randomised survey, but the social differentiation of blogs was suggested by the findings reported in Chapter 5. Parents’ accounts of similar parenting practices in section 6.2.5 below adds further weight to the interpretation made here that blogs were socially differentiated spaces used by a homogenous group of parents. 6.2.4 Fortuitously brought together? Bourdieu argues that members of an elite group will tend to find themselves in social contact through participation in social settings that “[bring] together, in a seemingly fortuitous way, individuals as homogenous as possible” (Bourdieu, 1986, p.250). This section begins with a discussion of what was meant by ‘like’ and ‘unlike’ others from the perspective of interviewees and how and whether parents were able to identify those who were ‘like’ them in practices, tastes and therefore social position in online settings. This was explored in terms of the use of different mediums of online peer support, where no differences were found, except in the use of blogs, discussed above. When asked about whether other parents in an online peer support forum were ‘like’ them or not, eight interviewees, with children of all ages, described how other parents of children with Rett syndrome or serious health problems were similar to them in that they experienced the same lifeworld. This was seen as distinct from the lifeworld of parents of children without serious health problems or disabilities. All of the interviewees who cited this ‘likeness’ had school-age or pre-school age children.
So I’m feeling less isolated knowing that there’s other people who deal with the same complicated, crazy things that you do
[Interviewee #76, mother in her 40s of a 5-year-old girl with Rett syndrome, diagnosed 3 years ago].
For one interviewee, this was closely connected to the sense of biographical disruption and grief discussed earlier, and provided a kind of social benchmarking for acceptable emotional responses to the diagnosis.
[JH: And do you find that the this site is a sort of good place to kind of spend time with other parents um sort of if you’re feeling a bit isolated or or wanting to kind of socialise with other parents who who are more understanding of of your situation?] Definitely because I think only other parents can understand what you’re going through. Your own family can’t and I think that’s um a common factor. […] Even the specialists can’t understand it unless they’ve got something similar going on […] and if you put you know if you if you’re feeling down I personally can’t post something about when I’m feeling down erm but sometimes it helps to know that somebody else is going through that and what you’re going through. [JH: Mm hm] You know, uh u’ a form of grief. [JH: Yeah.] Is normal.
[Interviewee #25, mother in her 40s of an 8-year-old-girl with Rett syndrome, diagnosed six years ago]
However it should be noted that this was by no means a unanimously held view among interviewees with children of this age. It is also notable that none of the parents of adult children expressed this attitude about other parents using online peer support sites, a finding that is explored in more detail in the final section of this chapter.
Answers to more direct questioning about whether other parents had a similar ‘social background’ were illuminating. Interestingly, in a finding that recalls some of the early research into the potential of the Internet as socially levelling, many parents reported finding it difficult – to a certain extent - to assess the social backgrounds of other parents, even within Facebook groups where online profiles were visible. This sense of social background could be missing across a number of different, relevant aspects and the lack of information could work both ways.
They wouldn’t know that I I was a single parent by that posting, you know, so, u’ how would I know other people? Some people have got their own pictures, some have got pictures of a whole group of Rett people on a fundraising thing or I’ve got no idea when somebody says, ‘oh, I’ve got an older girl […] ‘but you’ve got no idea when someone says, ‘my daughter this’’, I said [?] it could be a five year old dealing with seizures, it could be a fifteen year old, or a twenty year old, I don’t know whether they’re in the middle of nowhere, stuck, you know, isolated in family situations with support, cos you know what? Those forums don’t give you that information, that’s when you realise, although you think you’re on an open forum where people are prepared to discuss, no they’re not, they’re doing what I’m doing, they’re posting when they want to post, when it’s appropriate to post. Nobody’s got any clue that I’m a single parent
[Interviewee #174, mother in her 40s of a 14-year-old young woman with Rett syndrome, formally diagnosed eight years ago although mother realised 12 years ago]
Interviewees found it difficult – perhaps socially inappropriate - to discuss the impact of social background on their propensity to ‘gel’ with other people. However, in the following account some interesting points were made about the difficulty of differentiating between people of different social backgrounds in an online group setting. However this was ultimately reframed by the interviewee in terms of ‘having an affinity’, which she argued was not necessarily related to class, but was strongly suggestive having a shared habitus, which may not map directly onto socioeconomic background, but may reflect it to a certain extent (see discussions in Chapter 3).
I don’t, uh- although I would say that perhaps on a face-to-face you might gel more to a similar – I don’t want to sound snobbish if I say a similar class or a – [pause] it’s not quite that, I guess you just gel with certain people don’t you? [JH: Yeah, yeah, yeah.] Um that online you might not ch – because you’re not meeting them face to face [JH: Ok, yeah] you might gel differently [JH: Ok] I suppose is a way of saying it. [JH: Why, why do you think that is?] I don’t know, is it just we have a ne- I don’t know, for me I just know I like someone or I don’t like someone so I would just gravitate to someone who I seem to quite like if that makes sense. Whereas when you’re perhaps gelling on a, on an online community it’s slightly different isn’t it [JH: Mm] because you’re not meeting – you’ve not got the eye contact and the body language, you’re missing all of that so you might just gel with that person because you like what they say or um, you, you’re going through a similar thing but you could meet them face-to-face and think, ‘oh my God, I don’t like you’ [JH: yeah, yeah] I don’t know [laughs] it’s [JH: and you won’t – you wouldn’t be able to tell necessarily you think from, from the online contact things that you might] No, [JH: pick up] no I don’t think so because I think – when somebody’s talking you pick up different things – in their voice that you can’t pick up when somebody’s typing […] [JH: yeah. And in terms of – if people are similar to you in terms of background, social background and so on, do you think that’s something you might pick up more face-to-face than on, than on groups, or do you think it’s something that comes across on] I don’t know [JH: groups anyway] I don’t think it particularly – unless they’re baring their souls which we know lots of them do [laughs] it might not come across on a social networking site, I think it’s more likely to come across if you’re face-to-face perhaps just. Um, but – yes, I know a couple of Rett families who I gel with who perhaps aren’t the same social background or whatever. Uh, I don’t know [laughs] [JH: But there’s something you feel they’re kind of a kindred spirit in another way, or] Well, probably, I don’t know, probably uh, I don’t know really – yes, difficult [JH: it’s difficult to say, some people you like, some people you] yes, yes, I think it does just come down to that really and you just gravitate to people that you’ve got an affinity with in some way.
[Interviewee #28, mother in her 50s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
Fifteen interviewees described other users of an online peer support source differing from them in some way (this was usually in relation to Facebook Groups, the most used source of online support). This could include aspects already touched upon, such as age and severity of health problems of a child. For some parents, access to ‘unlike’ others was a positive advantage, for example as a source of bridging social capital between less experienced parents of younger children and parents with older children and more experience. However there were also aspects of preferences and choices, which are argued below to be expressions of habitus. These are explored in the final section of this chapter in terms of how they ‘fitted’ or jarred with different specific online peer support subfields. As argued above, over time parents would narrow their social networks to trusted allies, sometimes including other parents with whom they felt they had ‘something in common’ or an ‘affinity’. As reported in Chapter 5, the use of blogs was differentiated by income as well as age. These findings were reflected in interview results, where wealthier and more educated parents who wrote or read blogs either did not engage with other forums or described feeling a particular affinity with bloggers rather than people posting on other online platforms.
Um, and I quite like her... she's got some lovely pictures and she's got some favourite quotes and um (long pause, sound of keyboard) I like that sh- sh- that this is about... (drinking tea) her thoughts and feeling and experiences and they're, they're very well written. […] [Crying] So I sort of feel like you can find these kindred spirits. That you don't know each other (sound of reaching for tissues) but you're kindred anyway.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
However, these interviewees could also find themselves moving through a range of online support spaces as they discovered different sources of support, which may more or less reflect their habitus. There were also differences in how parents of older children engaged with many online platforms that – at least among survey respondents – tended to be used significantly more by younger than by older parents. This relationship was particularly strong in terms of the differentiation of peer support Facebook groups. These were popular sources of information and support and to a certain extent, difficult to avoid entirely if one wished to keep abreast of current developments and research, which was important to all interviewees. 6.2.5 Fits and misfits between interviewees’ habitus and forms of habitus expressed on online peer support subfields This final section explores aspects of habitus fit and misfit between interviewees and different online peer support sites they had visited. This was expressed in terms of how or even whether such spaces continued to be used over the longer term, following initial contact and use. Four areas emerged from interview data as pertinent when interviewees considered their fit with an online peer support subfield. These were parenting practices, digital taste, emotional expression and illness narratives.
Parenting practices Despite the difficulty of explicitly identifying people’s social backgrounds, there were aspects of taste and parenting practices that were analogous to Bourdieu’s conceptualisation of social position within social space in Distinction (Bourdieu, 1984). One key differentiating factor was disagreements about parenting practices, which were raised by thirteen interviewees and mostly related to some Facebook groups, or unspecified peer support sites. For example, these related to differences in terms of decisions about a range of topics, including medication, respite, when to take your child to hospital, whether or not to go ahead with a second pregnancy with a foetus diagnosed with Rett syndrome, diet, and the use of dietary supplements.
there are some families that are on multiple treatments but other families that’s decided not to give um medication to their children. Um, and on the [Facebook Group] families have vigorously disagreed about both both sides of the opinion. Um, you know particularly if their child is struggling severely with epilepsy. Um and I remember somebody posting about how they wanted just to enjoy, enjoy what their child could do and the life that they could have and I really understood that post. But somebody else, whose child was going through a a erm a lot of hospital treatment, found it offensive because their child was really struggling and was really ill. [Interviewee #25, mother in her 40s of an 8-year-old-girl with Rett syndrome, diagnosed six years ago]
Only one interviewee described encountering these differences when reading a blog, which was one of her reasons for providing a counter-narrative in her own blog. The blog was American and her observations reflect wider differences between discourses around religion, and children as ‘gifts’ that were also raised by two other interviewees in relation to their contacts with American Facebook ‘Friends’ with children with Rett syndrome.
I think, you know, the other reason, of course, that I started the blog, that I should have said when I did my search for blogs about Rett syndrome or blogs about children with special needs, I found a heck of a lot of stuff that was all very sweet and lovely and two-dimensional and… you know, some of it, there was, you know, it was completely unobjectionable but I just didn’t find it quite enough and I thought I wish I knew a bit more about, you know, some of the stuff that’s difficult, you know, I find life difficult, does anybody else find life difficult? [JH: Yeah yeah yeah] Is it just me or does everybody just look at their child and feel completely blessed to have, you know, such a, such a gift, you know? [laughs] Um and I, yeah I found it quite isolating that I, you know, that I felt, to begin with I was struggling, I think, I hope it comes across on my blog how much I love my daughter but also that I really struggle with all sort of things um and I just wanted to kind of give voice to that and also counter – yes, I suppose I was, in my own little way, even though I didn’t what, you know, whether anyone would much read it you know I was sort of expressing my own frustration, I think, really than… there was a lot of stuff out there as well, particularly emanating from America you know, along the lines of, you know, God gives special children to special parents, kind of thing you know and I just wanted to, to bust the myth of parents of children with special needs being special, I suppose that […] you know, there’s nothing special about it, you just deal with what you’ve gotta deal with. [Interviewee #76, mother in her 40s of a 5-year-old girl with Rett syndrome, diagnosed 3 years ago].
Of the two interviewees who wrote blogs, only one had experienced a criticism from another parent about her parenting practices.
Um, I did have a message once from somebody, who’d left, you know, left a comment left on a blog post, saying, that she thought it was very sad that I was so negative but there’s been very little of that kind of thing. I’m amazed really, gi- u- knowing what the online world is like […] it wouldn’t have surprised me if I’d had you know people, telling that you know, I just needed to pull myself together or stop whinging or you know realise that, you things could be much worse or whatever, but everyone’s been really polite [laughs]
[Interviewee #76, mother in her 40s of a 5-year-old girl with Rett syndrome, diagnosed 3 years ago].
These differences are important because they demonstrate the different kinds of experiences of online support by wealthier and younger parents who were significantly more likely to read blogs in the wider sample of survey respondents. In fact two interviewees in this group had decided either to withdraw from reading Facebook groups altogether or had never used them, so were – at least for a while – solely reading blogs, and therefore experiencing far less exposure to conflicting parenting practices and tastes, at least within the UK blogosphere.
Digital taste As noted in Chapter 2, there has been a shift in recent literature from demographically-deterministic descriptions of use of the Internet to exploring clusters of attitudes, for instance in the ‘cultures of the Internet’ described by Dutton and Blank (2013). A key differentiating factor among interviewees seemed to reflect a form of digital taste, expressed through a preference for either information-based interactions or more emotionally- based, sociable interactions. The first form of interaction was more likely on older peer support platforms, such as email groups, which reflected the styles of interaction used in the pre-participatory web. The second form was more closely tied to the forms of peer support provided on social media platforms, such as Facebook. This could therefore lead to habitus mismatches between platform and digital taste, as these excerpts show.
I get a bit fed up with it if I’m honest [JH: Ok] I get fed up with the things people post [JH: Do you?] […] You know I don’t need to know your child’s just – uh – had a spoonful of medicine – I, I, I get – yeah – I get a bit [Laughs] [JH: Do you find it goes into quite a lot of mundane?] Well I think some people are just on there constantly [JH: Ok] posting everything about their life [JH: Yeah] and that isn’t for me [JH: No, no] If they just used it to ask questions and people answer rather than keep posting, oh, you know, ‘my girl’s in hospital again’ [JH: Yeah] I don’t know really [JH: Yeah] [Sighs] [JH: Yeah, so you’d sort of prefer] But that’s me [JH:Yeah] D- do you see what I mean [JH: Yeah, of course] and somebody else might like the fact that they know what every Rett girl is up to constantly but for me I don’t need that.
[Interviewee #28, mother in her 50s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
[JH: let’s look then at the, the one the other one that you stopped using, the [email group], what what happened with those? What’s what’s your experience been with those?] Um, [sighs] it was a quite serious and of course you know it is for fact-finding and and I don’t I just found it quite, automated
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
Although older interviewees tended to prefer information-based communications, some younger parents also expressed a preference for this kind of interaction too, suggesting a difference in habitus that was not socially determined, but may partly relate to the wider structural differences between generations. A related aspect was interviewees’ willingness to share their feelings, and the links between illness narratives and biographical disruption, which are discussed in the following subsections.
Emotional expression Parents differed in terms of what they were prepared to share online, particularly when they were struggling to cope. This varied along a continuum from parents for whom this was unthinkable to those who had no concerns at all about sharing their feelings online. This was interesting because for both sets of interviewees there was no distinction drawn between privately accessible and public sites. This may however reflect the lack of anonymity available on most of the online sources of peer support used by this group of parents, particularly Facebook. For some parents, this involved differences in terms of using online peer support sites as a place to ‘vent’ or ‘let off steam’ when experiencing something frustrating, like a problem with a local service.
[JH: Ok. So at the moment, as as it stands and the groups and the sites that you know, you don’t think there’s anywhere you could kind of go to let off steam that would be in a kind of private…] Yeah. I would do that privately. Um, also because I kind of feel weird about doing that pu- publically. [JH: Yeah] um, [JH: Ok, so it’s something you might not do even if there were spaces to, to] That’s it. That’s it exactly.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
We did, I think it was on the Rett Shared page actually, we did, we did have a um, a rant thread [JH: Oh ok, yeah] and it was just one thread that you could just add your ‘AAAAARGGGH!’ to, if people wanted to [JH: (laughs)] to just have a moan and no one would comment on it, it was just you could ‘rrrrrgggh!’ Let off steam on the keypad and that was your rant thread [laughs], which was quite good
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
Differences in propensity to share emotional experiences online could be related to the strength of ties with people in an online environment versus those in personal relationships offline.
I mean it’s like anything, you know, you’ve you’ve got friends that you will, you’ve got work colleagues and you’ll sit and chat about what happened on the telly last night and where you done, where where did you go at the weekend, but you wouldn’t necessarily tell them that, I don’t know, that you’ve having a nervous breakdown or [laughs] you know, but your very close friends, you might well tell them that so I suppose it’s the same as in real life, isn’t it? [JH: Yeah, so they’re, they’re almost more like colleagues in a way, in terms of the kind of, u’ u’ sort of, [inhales] um, conversations that people expect to have with each other in those kinds of] Yes. Some of them can be personal about your child but not so much personal about yourself.
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
However for other parents a reluctance to share emotional experiences online appeared to reflect an overarching emotional habitus that applied equally online and offline, learned through family socialisation.
I wouldn’t ever particularly say we’re having a rough phase. I, uh, I don’t know because that’s just me because I feel I have to cope with my lot in life and not keep telling everybody because again, I suppose it’s the way I was brought up – not to wear your heart on your sleeve. If somebody says to you, ‘how are you today?’ you say, ‘oh I’m ok thank you.’ Because people don’t want to hear you say, ‘oh well actually, I’ve got this pain here and I’ve got a headache and my thumb hurts,’ You know, people get fed up with you. So I think I tend to – uh – always come across as quite cheerful and coping even if I’m not.
[Interviewee #28, mother in her 50s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
Propensity to express one’s emotions was not related to educational level among interviewees. However, it bore some relation to age. Although some parents in each age group described themselves as guarded online, no parent interviewees in their 50s described themselves as ‘very open’ online or willing to expose themselves at all. By contrast, parents in their 30s and 40s occupied a range of positions, from not sharing any emotion at all through some willingness to risk some exposure online to those who had no qualms about being very open online. Emotional expression was also closely related to concerns about ‘scaring’ parents of recently-diagnosed children and the kind of illness narrative adopted, explored at the end of this section, where some parents reported not sharing how they felt because they wanted to avoid adding ‘negative’, chaotic posts to online peer support forums.
Illness narratives As discussed in section 6.1, older interviewees talked about having reached a point of repair in terms of the biographical disruption experienced with receiving their daughter’s diagnosis. A key point of fit between individual and online subfield habitus related to the perceived illness narratives on an online subfield. Some illness narratives that parents described encountering on forums were similar to the ‘chaos’ narrative described by Arthur W. Frank in The Wounded Storyteller.
Chaos is the opposite of restitution: its plot imagines life never getting better. Stories are chaotic in their absence of narrative order […] are told as the storyteller experiences life […] The lack of any coherent sequence is an initial reason why […they] are so hard to hear (Frank, 1995, p. 97)
In its most extreme form, this involved a series of posts criticising an organisation’s research into a cure and the length of time it would take, which were effectively silenced with sanctions applied to the poster, who was perceived to have broken an unspoken rule meaning sanctions had to be applied.
he was able to splurge everything. People don’t do that and actually look at look at everybody’s reaction when he did [JB: Yeah, and what were they?] Block him, I blocked, don’t do this I’ve heard that he’s spouted off, I’ve blocked him, please ignore his, please du-de-du-deor is it like my reaction of look, you r’ you know, I empathise with you but you really shouldn’t be doing it so is that an element of why some people hold back? [JB: Mm. So you think people are kind of i-in a way they’re kind of sent to, sent to Coventry and ignored and blocked and, that kind of thing (?) happens?] They don’t want to hear his point of view
[Interviewee #174, mother in her 40s of a 14-year-old young woman with Rett syndrome, formally diagnosed eight years ago although mother realised 12 years ago]
The above account was a strong illustration how a series of sanctions were applied to somebody who had posted something considered too chaotic and too negative by other members. One interviewee reported that other members of a group had told her they had blocked33 this individual. Although Facebook argue that someone is not notified that they are blocked, it will become evident if they ever try to engage with somebody who has blocked them.
33 Blocking someone on Facebook involves ‘unfriending’ someone and means they can’t start conversations or see things that you post on your own profile. In addition, people who are blocked cannot tag someone in a picture, invite them to events or groups or add someone as a friend. However, interactions in groups can still be seen. (https://en-gb.facebook.com/help/290450221052800) However, a subtler form of chaos narrative could be in the form of what was described above as helpful to some parents: ‘letting off steam’, ‘ranting’ or ‘venting’, which was like an unresolved story. However, for one interviewee, reading these kinds of posts led to them reducing or stopping their visits to the site in question.
I think there’s too much um slanging [laugh] criticism about this and that. It sounds like people just seem to be moaning a lot. [JH: OK. What what sorts of of things of that sort of people complaining to to each other or about situations that they’re in. What sort of thing?] Er, mainly about health professionals being unsympathetic or the system is very slow and they have to spend a lot of time waiting in the hospital. Things like that. [JH: OK. Um so does that does that sort of affect how you use the group, do you think?] Yes, I think I tend not to go on it because it’s just people moaning about things rather than actually asking for advice or being supportive to each other.
[Interviewee #116, mother in her 50s of a 20-year-old woman with Rett syndrome, diagnosed 17 years ago]
However, for other parents negative comments could include other parents sharing their feelings with one another, which appears to relate back to the propensity toward emotional expression online discussed above.
but I think because often people are too bogged down into telling everyone about their daily life and then people say, ‘oh, poor you, oh, I’m really sorry, you know, oh, we’ve had that trouble too,’ and then I think, ‘oh, for goodness sake,’ I think sometimes - that’s what I – that’s the point I’d like to make, I think sometimes it’s all too negative, there’s not enough positives on there and I suppose I’m a positive person so I would rather post something that’s positive than to say, ‘oh, I’m having trouble with [my daughter], she’s having episodes and I don’t know what they are, can anybody help me?’ [JH: So does that, is that sort of how you’ll decide to post, part of the decision you make in terms of what you] I think so [JH: posting (inaudible)] Yes [JH: Yeah. Post so, it’s sort of, some progress really with this] Yes. Yes [JH: yeah. Ok.] Because I think ultimately that’s what most people look for - people want hope
[Interviewee #28, mother in her 50s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
This put some parents’ preferences in direct opposition to other parents’ needs. However one parent noted how initially ‘negative’ posts about facing a problem could be turned into co-created positive narratives with input from others. This was like the collaborative problem solving posts described by Huws and colleagues (2001) in Chapter 2.
I have to say that it’s somewhere you turn to when things, as you say, are, are going wrong or something new’s cropped up and it’s not working out, it’s [laughing] rarely somewhere you go when you’re saying, ‘this has gone really well’ [laughs] [JH: yeah, yeah, ok] That’s a shame really, cos we we do tend to use it more as a, ‘oh God, I can’t cope with this anymore,’ but, saying that when, someone may put a post that’s quite a negative – something that they’re going through that’s quite negative, if you’ve had that positive experience you can then reply to them and say, ‘have you tried this, this is brilliant’ um, you know and impart some more positive advice
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
Some interviewees described deliberately posting more positive, counter- narratives in response to more chaotic or ‘negative’ narratives or a perception of there being too many ‘negative’ posts overall on a forum. This involved some creation and co-creation of positive presentation of their children, which some parents noted were also missing from other sources, such as charities’ literature. This was like Jones and Lewis’ (2001) findings, where parents of people with Down’s syndrome posted to celebrate achievements and to present their children as children first.
another time when there was something really negative […] I left a a few posts cos I don’t wanna be seen to be ca’ but I put up […] [a picture] of my girl having fun and they’d they’d put all the negatives about their child and I said, um, this is a child that has […] [serious health problems] now look at the child. That that’s that’s the definition of her condition [JH: yeah, yeah and this is her] and this is her and you you know what it was the same positive mums, yeah, aren’t our girls beautiful when they smile.
[Interviewee #174, mother in her 40s of a 14-year-old young woman with Rett syndrome, formally diagnosed eight years ago although mother realised 12 years ago]
As discussed in the next chapter, the positions taken by rival charities were also reflected in the kinds of illness narratives shared online, and could become a focus for struggles for symbolic capital expressed through conflict within some online subfields.
6.3 Interpreting the interplay between micro practices and structural differences in online information and support seeking
This chapter has explored the differentiated use of online support sites that was suggested by the survey findings reported in Chapter 5. By exploring parents’ use of online support and information in context, it has provided a richer picture of how age of respondent, age of child and time since diagnosis relate to wider differences in expertise, access to social capital resources, stages of biographical disruption and the changing care needs of children and adults with Rett syndrome. This was a crucial finding as it recontextualises existing literature that discusses digital inequalities in seeking online information by providing a coherent account of how these multiple aspects of parents’ lives structure the kinds of support they need. By including parents who did not have access to the Internet at the time of their diagnosis, it also shows how similar kinds of information seeking occurred across a wider and changing social and technological background, as well as in a changing research environment. The inclusion of parents’ accounts alongside a survey has therefore provided a more three-dimensional picture of how support and information needs are dynamic and changing over time, while also occurring within a wider and changing social and technological context. In particular, this suggests that although parents of different ages use online support in different ways, this reflects accumulation of expertise and social capital resources, with online resources used in a more targeted way over time, rather than an impoverished level of use of the Internet, at least among the parents interviewed here, who were aged up to 58 years old. The second section explored how the ‘fit’ between online peer support subfields varied for interviewees who held wider forms of cultural and social capital and differing habitus. Although the survey found no differences in ever having used generic online sources of support and advice, there was some indication of a differentiated use of and prioritisation of different sources of support. Thus, where preferred sources of information were discussed, interviewees with the least education were more likely to seek help in solving a new issue primarily through posting on a peer support forum, while parents with a higher education qualification were more likely to seek primary sources of information first. This finding was speculative, but merits further exploration in future research. Having existing preferred social capital sources also influenced the use of online peer support subfields. In deciding between using different online subfields, parents’ tastes and preferences appeared to guide them. These were indicative of wider habitus and included differences in parenting practices, digital taste, emotional expression and the use of different illness narratives, the latter appearing to reflect the level of biographical disruption experienced by that parent at that time. Together these findings suggest that carers’ full quotient of cultural capital, social capital, and habitus influenced their use of online sources of support and information. Although there was some evidence that the use of online support could provide some bridging capital to parents who did not possess the same levels of cultural capital, the differentiated use of blogs described in Chapter 5 and the exclusive use of blogs by some parents to share expertise suggested there was evidence of the existence of some elite social spaces online. Taken together with the suggestive findings about information- seeking strategies, it is possible that parents with greater education may be able to access more sources of primary information, such as research, and to access information about caring strategies in an environment with less conflict, where shared habitus may be reflected in similar parenting practices and tastes. The impact of such differences will be explored further in the next chapter in terms of how online peer support subfields can be sites of struggle for symbolic power in wider fields and how parents’ possession of valuable ‘goods’ and cultural and social capital influences the symbolic power they can gain in wider caring fields. Chapter 7. ‘Playing the game’ – symbolic capital online and within wider caring fields
This chapter widens the lens of this research to explore the position of online support and information seeking as they relate to wider symbolic and structural power contexts. In section 7.1 I question the depiction of online peer support sites as inherently democratic by some commentators (see Chapter 2), using as an example how certain online subfields where peers can exchange information appear to reflect existing institutional power structures and broader digital inequalities. The bulk of this chapter explores the micro aspects of research question 4, specifically whether wealthier, younger or more educated parents accrued benefits from online support that were not sufficiently explored by survey results reported in Chapter 5. Section 7.2 picks up questions raised in Chapters 5 and 6 about whether parents holding more cultural or economic capital were able to access a wider range of sources of information online. This section also problematises the notion of the existence of distinct ‘lay’ and institutional information in silos online, arguing instead for a greater networked connectivity between different online spaces. Finally, section 7.3 explores whether benefits gained online are converted into symbolic power in wider caring fields, and whether these benefits accrued inequitably. The chapter closes with a summary of the role of online peer support sites within wider power structures. In Chapter 8 I bring these findings together with the findings described in Chapters 6 and 7 and reflect on what this research can contribute to the wider field described in Chapters 2 and 3.
7.1 Symbolic power online: why some online support spaces are more equal than others
As discussed in Chapter 2, research into the use of online support by parents of people with rare syndromes has either tended to treat all online peer support sites as interchangeable or to explore one site to the exclusion of all others, with only a few exceptions. As part of the exploration of how individual habitus fits – or does not fit – with online subfield habitus, some differences in symbolic power on two kinds of site were noted. In the previous chapter I discussed misfits between online subfields with personal habitus in terms of parenting practices, digital taste, emotional expression and illness narratives. This section explores how the unequal distribution of symbolic capital influenced parents’ use of two online support mediums: the Facebook ‘Pages’ of organisations and parental blogs. These operated in subtly different ways, but had similar impacts on the posting decisions described by interviewees. When parents discussed attempts to use organisational Facebook Pages for peer support it was clear that the structure and use of these groups influenced the ‘goods’ they could access there.
Yeah, yeah I tend to see what comes up in the Timeline. That’s what I mean, I tend to avoid, like, not not avoid but not see the other messages that are in there, like other section, whatever it’s called [laughs slightly] [JH: Yeah, yeah I know what you mean cos there’s some that are sort of, have got a higher profile haven’t they in there] Yeah [JH: cos I posted on it myself and you go, ‘ooh, where’s my message gone?’ (laughs)] Yeah, I’ve just I’ve just got it up, it’s called, ‘Recent posts by others on [Institutional Facebook Page]’ and you don’t tend to go into that bit
[Interviewee #30, mother in her 30s of a 12-year-old girl with Rett syndrome, diagnosed 9 years ago]
One parent discussed how when he had posted on one of these pages, the reaction from peers was disappointing
I posted about vaccinations. If they were safe for children with Rett's Syndrome. There was only one response from another subscriber. She was asking the same question as me […]The main limitation […] I have found is the lack of feedback from the group on questions and queries submitted through [the] Facebook [Page].
[Interviewee #84, father in his 30s of a 3-year-old girl with Rett syndrome, diagnosed during the past year]
This led to this interviewee deciding not to post unless they were engaging directly with the organisation rather than other parents. Another interviewee described how she felt constrained in how she posted on a charity’s Facebook Page. The distinction made between Facebook Groups and Pages34 below is important because it demonstrates how the structuring of pages within Facebook is recognised by some users and can encourage or discourage different kinds of posting behaviours. This relates back to arguments in Chapter 2 about the importance of considering how the technology of the Internet may influence interactions online (Halford & Carrigan, 2014; Kivits, 2013; Seale, 2005).
Um I probably wouldn’t let off steam as much on the [Charity Facebook Page], sort of if, if I was that down I’d probably ring them rather than being on their, you know, Facebook page ranting and raving [JH: Yeah. What what do you think would happen if you did post that kind of thing on that Page?] Um, probably not a lot but it’s probably not the place to do it [laughs] [JH: Yeah, sure sure, is is so that’s something you kind of, picked up from what people post and] Yeah just things that [the charity] hasn’t necessarily, cos i-it’s not on their their, it just seems because it’s run by professional – not professionals but do you know what I mean, it’s not, t’ cos they’re not run by parents it’s more of a place where it’s a bit more formal [JH: Ok sure] than it being a place where you can rant and rave [JH: Ok, so it’s kind of more, more about the kind of practical support
34 Facebook Pages are intended as ‘official profiles’ for businesses and brands, while Facebook groups “are the place for small group communication and for people to share their common interests and express their opinion” (https://www.facebook.com/notes/facebook/facebook-tips-whats-the- difference-between-a-facebook-page-and-group/324706977130) They are structured accordingly to foster these different forms of communication. than maybe emotional support in terms.] Yeah, i-it’s um it’s a Page rather than a group, isn’t it, uh whichever way around it is
[Interviewee #30, mother in her 30s of a 12-year-old girl with Rett syndrome, diagnosed 9 years ago]
For organisations’ Facebook Pages, responses were effectively limited to reactions to the posts made by the organisational representative. In the case of blogs, there were no places to post new topics so parents could only respond to the blog topic. One interviewee described how this set up a power imbalance, suggestive of symbolic power, which led to the organisation or blogger effectively setting the agenda for what would be discussed. As she describes, these were not places where parents were on an ‘equal footing’, but places where they were expected to react to, rather than initiate, conversations.
And I do, I do go and look at them a lot, but I don’t post. But to be fair, I don’t think that many people are posting [JH: No, I think you’re probably right] I think that people are commenting, but they’re not… starting the conversation, um, and I, I was aware that I wasn’t starting any conversations, it’s now reflecting on it I realise nobody else is either. Um, that’s quite interesting to me, why nobody’s starting the conversations, unless it’s the charities making a comment or the bloggers making a comment they then react to […] But maybe [people are more likely to post on] a forum more like Mumsnet, where everybody’s on equal footing because there is a bit of a power dynamic here, that this is owned by the charity, run by the charity, so it’s up to them to post. Owned by the blogger, their blog, so it’s up to them to blog um and everyone else reacts. If there was something that had less of that power dynamic, where everybody felt like peers, um, I would be more inclined to post [JH: Ok. Yeah, that’s a really interesting point, yeah]. Yeah. Because I do feel like I have things to say, Um, and I’m intrigued by the fact that I’ve never said them [JH: Yeah] [both laugh] Yeah. But it occurs to me nobody else is either. [Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
This is interesting because recent OxIS data suggests that a higher proportion of wealthier groups write blogs (Dutton & Blank, 2013). Therefore this greater power for bloggers to set the agenda in discussions on their sites suggests an undemocratic process at work, and the privileging of certain voices over others. A second important factor was the use of broader, non-institutional online peer support forums (e.g. Facebook Groups) as channels for promoting specific ideological agendas. It will be recalled from Chapter 1 that there were two charities that fundraised for a cure for Rett syndrome (one of these also aimed to provide support) and another charity that focused on providing support to parents. Parents involved with all three charities, either as supporters or in more formal roles, were active on different online peer support groups and contributed to discussions about fundraising. There was an urgency expressed in some forums about fundraising for a cure and an anxiety expressed by some parents that funds from cure research might be diverted to funding for support for parents35. This context is important to acknowledge as it serves to demonstrate how online peer support forums acted to a certain extent as subfields to “experienc[e] and negotiate[e] fields” (Sterne, 2005, p. 385), in this case, wider research and voluntary sector fields. The disagreements between charities were sometimes expressed in online support forums in ways that some interviewees described as quite polarising. The parents I interviewed sometimes had a specific allegiance to a particular charity, but four interviewees discussed supporting more than one charity. This could be reflected in a certain amount of disconnection between the more polarised narratives expressed online and the more nuanced views held by some interviewees privately.
there was a big um, there was a big hoo-ha last year about [two of the charities], almost like, people were, making out that they were having a
35 These observations came from interviewees’ accounts, but also from my own informal observations when using groups to post recruitment notices. war with each other and it’s just ridiculous, you know, and it was like, ‘oh, you’re either [one charity] or you’re [the other]’ and I just do not get involved in any of that, I completely refuse to be drawn either way
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
One interviewee was criticised for sharing a picture of a symbol of support to one particular charity on an online peer support forum. It is interesting to observe her account of how after she felt she had been misrepresented she used distancing tactics, but ultimately decided to withdraw her post, effectively meaning she had been silenced.
I posted [that] I had um bought [some merchandise from one of the charities], um, I’d got that bought as a […] present, so I […] put it on there, you know, showing it off basically and that was, that got lots of mixed reactions to be honest [laughs] [JH: Really?] I had some people saying it was um, it was really lovely and then had other people telling me that they didn’t need [merchandise] to show that they had a child with Rett syndrome […] they got quite aggressive and abusive actually [JH: Really?] It really shocked me because we’re all parents dealing with the same thing but they did get quite sort of, nasty [laughs] […] it got out of control to be honest because it went back to how the group was formed [and allegations about how they operate] and it got, like I say, from this one tiny little post of me showing off [the merchandise] it got quite out of control […] and it, yeah, it did get quite, I was like, ‘hang on, I was only showing that, I have nothing to with [organisation] I’m just posting [a picture of the merchandise I was given] and that’s it’ […] and then they started getting quite sort of, about money and stuff and I was like I’ve got nothing to do with [that organisation] you know, I don’t I don’t know any of that side, […] and then some of the [people from that organisation] stepped in and and I think it ended up with about sort of 60 or 70 messages and I just left it in the end cos I just thought, ‘well, it’s nothing to do with me now’ I think I removed the picture by the end cos I just thought if, it’s not worth it over a picture, you know.
[Interviewee not named here to avoid identification]
Overall then, there was a tendency for the habitus of certain online spaces to reflect the habitus of those with the highest symbolic capital – which could be held by those who ran the group, or had influence in wider fields outside the group. This strongly suggests that some sources of online support are actually inherently undemocratic. Production of content, although feasible on such sites is actually constrained by existing structural sources of power and features of the site that privilege certain accounts over those of other parents. This supports my arguments in Chapter 2 that the Internet is not an inherently democratic place to share and find information, and that Bourdieu’s concepts of fields and symbolic capital can explain how certain groups may gain advantages in this social sphere, as offline.
The next section of this chapter explores whether cultural and social capital gained online is used to leverage unequal gains within online settings and within wider caring fields for more privileged groups. 7.2 Unequal gains? The role of online sources in accruing valuable ‘goods’
This section expands the findings reported in Chapter 5 about accessing ‘goods’ available on online peer support sites. As will be remembered, these were largely differentiated by time-related variables (age of respondent, age of child and years since diagnosis), except for emotional support, which was more often reported by parents holding a higher education qualification. However, survey responses were limited to questions asking about the use of online support, and particularly online peer support. This reflected how my own thinking had been influenced by the wider literature, which often distinguished between ‘lay’ sources of health information and institutional sources of health information. However, by listening to interviewees’ accounts it became clear that this distinction was problematic for a number of reasons, some of which have emerged in discussions so far in this and the previous chapter. Firstly, this did not take into account the interrelation between multiple sources of information and the use of social networking applications as ways of linking to external sites. In interviews and records of online support interviewees demonstrated how they used Facebook Groups – and particularly charities’ Pages – to find links out to scientific sites and research papers. Secondly, as described in Chapter 6, parents would seek information across a range of more traditional, information-providing online media (static websites) and ‘Participatory age’ social networking sites. Finally, some parents reported having read parents’ summaries of scientific information posted on peer sites. Therefore, for many parents, online peer support sites were not necessarily distinct from other kinds of sites and their use fitted into wider information-seeking strategies. This meant that in order to understand the role of online peer support sites, I needed to widen my understanding within interviews to how these fitted within the wider use of the Internet as a source of information across both peer support sites and other online contexts. This may explain the lack of convergence between survey findings and interview data, where survey data suggests little existence of benefits accruing unequally to those with higher cultural or economic capital. As noted in Chapters 5 and 6, this may reflect a difference between information and support, where, as argued above and in the previous chapter, parents sought information across peer online support and static websites, as well as wider offline sources. Also, while the survey specifically asked about decontextualised benefits accrued online, interview data was able to shed light on how the use of online support and information sources were embedded in the use of wider sources of information, both online and offline. This section explores two aspects of use that could shed more light on different practices among parents holding different levels of cultural capital. Firstly, how linguistic capital influenced the kinds of wider information sources that were used. Secondly how the ‘goods’ gained online differed by social group. These are discussed as they relate to quantitative findings reported in Chapter 5.
7.2.1 The role of linguistic capital in accessing ‘goods’ online As described in Chapter 3, linguistic capital is an important way of differentiating oneself from others, and may lead to the effective exclusion of people without commensurate linguistic capital from certain social settings. As also argued in Chapter 3, linguistic capital may therefore affect the accessibility of the range of online information sources available to parents of people with Rett syndrome, particularly with regard to interpreting relevant research and treatment developments. As described in Chapter 6, some parents benefited from the bridging capital of other parents who were able to synthesise and explain research in an accessible way on forums but were not able to interrogate primary sources themselves. This section aims to explore the impact of linguistic capital in the use of online sub-fields and how this affected parents’ accumulation of ‘goods’ from a range of information sources. In all interviews, parents were asked if they had ever encountered jargon or language they didn’t understand on any online peer support site. This information was available for all but three parents – one who had not completed a full interview, the husband of interviewee #133, who didn’t tend to use the Internet, and one parent whose answer was ambiguous. Given the significance of research interpretation among this group of parents, interviewees’ level of education was mapped against their level of understanding of different online sources and a suggestive pattern emerged. Interviewees holding postgraduate qualifications described encountering sources of information where their linguistic capital was adequate for reading most sources – certainly online peer support sites – and was sometimes higher than that used on some sites, which in one case had put one interviewee off from using a particular site.
Um... i-it's i- i- and q-quite badly written! (laughs) [JH: Mm, yeah] I sound very pedantic, but a lot of it is quite hard to follow [JH: Yeah] It's got spelling mistakes.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
No parents in this education grouping described encountering a site where they felt their linguistic capital was lower than the level of the group, except for the parent from the UAE, who would need local abbreviations explained on occasion. Six parents who held qualifications below a postgraduate level reported some difficulty with understanding jargon or language on a site. This included the parent quoted in Chapter 6, who had a higher education qualification but reported needing to rely on parents’ summaries of medical research due to her lack of medical knowledge. The information presented on a single site or group could vary in terms of linguistic complexity. Linguistic capital was therefore part of the decision to read information posted online and for one parent with a basic or secondary level of education, this would influence the kinds of information she read on a particular site:
if I hear of sort of some treatments that have been happening or you know tests or trials or something that might be happening I might sort of, pop in to see if they’re in plain English [laughs] like [?] if I can understand what’s going on [JH: Yeah and so if they’re not then that tends to, to put you off?] Yeah. [Interviewee #30, mother in her 30s of a 12-year-old girl with Rett syndrome, diagnosed 9 years ago]
Other parents in this group reported finding medical and scientific jargon hard to understand. This had been accessed through following links to professional forums, scientific blogs and research journals posted in charities’ online email groups and pages.
sometimes they’ll, if a new paper’s come out they’ll publish it on the website, which is great, but sometimes [laughing] I don’t understand a word of it because it’s all medical jargon and I think, ‘oh,’ and I don’t understand that
[Interviewee #75, mother in her 40s of a 14-year-old girl with Rett syndrome, diagnosed 10 years ago].
However, for one parent with this level of education, it was only the names of medicines that caused her any difficulty
Only time I struggle is when certain drug names are mentioned, we are lucky [my daughter] isn’t on any serious medication
[Interviewee #194, mother in her 40s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago]
Five parents, all of whom held a higher education qualification, described how they could usually work out what something meant or would search online for a definition or ask other users of a site if they didn’t understand a piece of language. For two parents (one in her 40s and one in her 50s) this included colloquial acronyms There might be some LOLs in all this new tech speak that’s the only other thing probably that some of the colloquial stuff that I have never come across. But you can normally interpret what the sentence means.
[Interviewee #86, mother in her 40s of a 13-year-old girl with Rett syndrome, diagnosed 11 years ago]
The ability to look up information on the Internet alongside the use of such groups and sites was important because it was a benefit of the asynchronous nature of online sources of social capital, where an initial lack of linguistic capital did not become a bar to participation as it might in a synchronous form of communication. However, it is worth noting that none of the parents with a basic or secondary level of education mentioned using one of these strategies to ameliorate difficulties with understanding language or jargon. This could relate to the potential differences in using more than one source of information hinted at earlier, or to a relative level of confidence in asking about jargon, which could possibly be related to possessing a certain level of linguistic capital. This can only be a speculation in relation to the data presented here, but could be a fruitful area for future research into the social differentiation of the accessibility of different sources of information. It is worth noting that ten parents, spanning different educational groups, described having no problem understanding the language on at least some sites or groups that they used, meaning that level of education did not act as a bar to understanding all the content seen on at least some sites. This highlights an important limitation with the data presented above. This was potential underlying differences in the kinds of information sought and read online by different interviewees. It was therefore difficult to assess how, for example, some interviewees might fare with more complex information than that presented on a particular site, or whether all parents had attempted to read research articles. However, the differences highlighted above broadly support the idea that many parents holding higher-level qualifications – particularly post- graduates - are able to understand a wider range of information presented on a wide range of sources and appear more likely to use a range of strategies to interpret unknown jargon.
7.2.2 Accruing online ‘goods’ The uses of online sources for three kinds of advantages are explored next in terms of how they may be differentiated by education, income and age. These advantages are knowledge and expertise, economic capital, and emotional support.
Accessing knowledge and expertise As argued in the previous chapters, there were some hints that wealthier and more educated parents may benefit more from the use of some forms of online support. As found in Chapter 5, the use of blogs was differentiated by income, with wealthier respondents more likely to have ever read a blog related to caring for someone with Rett syndrome. In Chapter 6, and as discussed above, some accounts suggested parents with a higher education qualification (a proxy for cultural capital) may be more willing to draw upon a range of primary sources of information without relying upon third party interpretations, although with some medical topics this could be limited for some parents in this educational bracket. This subsection explores some of the wider social capital resources that different groups of interviewees discussed drawing upon to build their expertise in relation to caring for their child with Rett syndrome. As noted in Chapter 6, this was particularly pertinent for older parents, who had accessed offline resources before online resources were available to them. Data was restricted to what was contained within the interviews and survey responses, which may not reflect the full range of sources that interviewees had accessed. Survey data summarised in Table 7.1 showed that respondents used a range of sources of support, both online and offline. Interviewees mentioned using a range of other sources of information alongside online support and information. This included books, magazines, telephoning charities, attending events, reading charities’ newsletters and magazines, other parents of people with Rett syndrome accessed outside online support forums, specialist Rett clinics run through Rett UK and specialists at Great Ormond Street Hospital. As reported in Chapter 5, 63.2 per cent of people who had ever used generic online support rated it as important to some degree. This was lower than the percentage that rated the following sources of support as important: local health professionals (90%), telephone support (81%), and local group support (73%). Ninety-three per cent of those who had ever read online peer support reported that they ‘probably’ or ‘definitely’ intended to read online peer support again suggesting those who had read it considered it an important source of support. However this may reflect the interests of respondents motivated to participate in this research.
Table 7.1 Use of different modes of support by survey respondents
Source of support n %
Local health professional support 172 96.6%
Generic online support36 159 89.3%
Telephone support 150 82.4%
Local group support 142 80.2%
Online peer support37 127 66.8%38
As reported in Chapter 5, 72 per cent of respondents reported that information and advice shared in online peer support sites had helped them to solve problems. This was not significantly differentiated by income or education, but by years since diagnosis, where it was found most useful by parents whose children had been diagnosed fewer than seven years ago. In interviews parents described using online support alongside other sources of information and support, choosing according to the information they were seeking. All interviewees, except Interviewee #133-H39 described gaining some knowledge through online peer support. Six parents across all
36 Support and advice available from a range of online sources, not restricted to peers 37 Support exchanged through peer messages on websites. 38 This reflects percentage of all respondents, not just current Internet users. Among Internet users, use of online peer support was 71.3% age, income and education groups described having gained information through online searches with an additional three having accessed sources of further information through an online search (two described having done both). Although parents discussed following links to research presented online, only one parent mentioned having independent access to journals (through her postgraduate course) and of using this access to explore primary sources of research on Rett syndrome around the time of diagnosis. Interviewees from across income, education and age groups reported having used online peer support sites to gain certain kinds of information. This included understanding the meaning of the diagnosis and prognosis or gaining information to understand and interpret new behaviours and symptoms. This reflected the use of online support sites as sources of ‘case histories’ to understand prognosis outlined in the research carried out by Schaffer and colleagues (2007) and Skinner & Schaffer (2006). Other kinds of information found in online support groups across demographic groups included useful caring strategies, information about services (excluding children’s educational needs) and information about specialist equipment. Twelve interviewees from a range of demographic groups described using online peer support sites to keep up to date with new developments (expert carer work) into therapies and treatments. This included research into a cure but also promising treatments and information about symptom management. There appeared to be some social differentiation in terms of information gleaned online. However, this does not mean that other groups did not seek them, but may reflect topics parents recalled during the interview. Peer online support was used to gain medical information by three parents, all of whom had a household income of over £70,000 and a higher education qualification. The discussions and information described related to managing a seizure (what to do in addition to calling an ambulance), deciding whether a child was ill enough to take her to hospital and tapping into medical expertise from parents with a medical background. Three interviewees discussed finding information about special educational needs online. All had school-age children, had household earnings of over £40,000 per year and held higher education qualifications.
39 This interviewee did not contribute in detail to a joint interview set up with his wife, but did mention using the Internet very little. Interestingly, two parents with basic or secondary education and school age children had some contact with a Speech and Language Therapist in a Facebook Group, suggesting again the possibility of accessing bridging social capital in Facebook Groups. There were some differences among the use of different kinds of support by parents of different ages, particularly those with adult children, who had not used peer online support for ideas about day-to-day caring, special educational needs and medical information. In terms of use of medical information, there was some indication that this may relate to different ‘dispositions’ (habitus) toward peer-professional relationships. Of twelve interviewees who expressed views about the relative importance of peer and professional information, seven parents noted that peer expertise should be considered ‘opinions’ and medical expertise should be trusted instead; three of these parents were in their 50s or (two with adult children). Additionally no parents in their 50s or with adult children endorsed views expressed by some younger parents of younger children as to the relative value or greater importance of peer information on some medical issues. For some parents of adult children, this reflected a more ‘natural’ trust in doctors, which this interviewee put down to age and which may reflect a generational difference in habitus in relation to attitudes to health professionals.
[JH: Ok, so if you if you need to know s’ about something in more de- so, say, epilepsy medication] Yeah [JH: How would you go about finding out about it initially?] Um… I feel really guilty in saying there’s been a vague acceptance that what what the Doctor has said b’ g’ is is ok [JH: Yeah yeah] and I, you know, I criticise u […] we criticise our mothers [JH: Yeah] for seeing doctors and teachers and clergymen as as the font all knowledge and you never ever um accept anything they say, and here’s me saying, ‘oh well actually I just [laughing] accept it!’ [JH laughs] [laughs] so yeah, so that’s bad, isn’t it, you know, I think that’s an age thing, I do genuinely think that’s an age thing [Interviewee #132, mother in her 50s of a 28-year old woman with Rett syndrome, diagnosed 17 years ago]
However, following the findings reported in Chapter 6, it is possible this may also reflect a greater store of expertise and access to trusted sources of information, including trusted medical and other professional allies. The use of peer online support seemed very accessible as it was used to gain information by parents from across the spectrums of age, education and income and could provide access to some professional information, research and links to external sources of information. However it is possible that the concentration of use in this sample is due to the recruitment and eligibility criteria of this study, which focused on charities and online peer support forums, with all interviewees having recently used peer online support. Therefore these sampling frames may over select parents who are already actively engaged in seeking information and support. There was a hint in this data that more educated and wealthier parents in this sample sought information early to try to establish a diagnosis and seek information about special educational needs. Nonetheless, two key aspects of this analysis were supported by other, less tenuous findings. Firstly, the differences in how more experienced parents use the Internet and other sources for support and information, which were described at the beginning of Chapter 6. Secondly, the use of primary sources of information among more educated parents, rather than relying upon summaries provided by third parties, also described in Chapter 6, although there were limits to what some parents with a higher education could understand in terms of medical research.
Economic capital Nine interviewees described gaining some actual or potential economic benefits from online peer support sites. As above in relation to alternative sources of information, this was dependent upon interviewees raising this within an interview and parents were not specifically questioned about this benefit. This means the information presented here may underrepresent the financial benefits experienced by all interviewees. This included both gaining ‘goods’ in the form of knowledge that had the potential or actually had been converted into economic capital. This included learning about eligibility for benefits and reductions to council tax, selling equipment, saving money on equipment and dietary supplements, access to available funds and grants, and accessing reports in support of funding for equipment written by professionals.
Yeah I mean I was I was trying to get travel insurance for [my daughter], um and two years ago we paid over £400 for her travel insurance and then someone said to me, ‘oh you you know the Family Fund are now doing a special deal for families like ours’, um at only £51 [JH: Oh wow] So you know, that sort of information
[Interviewee #30, mother in her 30s of a 12-year-old girl with Rett syndrome, diagnosed 9 years ago]
so um, funding for Eye-gaze computers, that’s a big deal, people talk about that a lot online and.. um, yeah, hearing about, what other people have been able to… do, so, for example, um, yeah th- there’s b- there was some sharing of um Speech and Language Therapy reports that were written in support of funding for an eye-gaze computer that kind of thing
[Interviewee #76, mother in her 40s of a 5-year-old girl with Rett syndrome, diagnosed 3 years ago].
These parents spanned the income groups and were represented in each educational group. However only one of the five parents of adult children mentioned having ever used an online peer support site to gain economic capital. When the type of benefit and whether it was a potential or actual economic gain was explored, some interesting patterns emerged. For parents on incomes below £30,000, two parents received an actual benefit (reduction in council tax and reduction on the cost of a small needed item). Parents with household incomes above £30,000 per year had increased their economic capital through selling old equipment in an online peer support group, and had accessed information about potential benefits (Disability Living Allowance) that might be useful in the future, seen Speech and Language Therapy Reports used to argue for statutory funding for an eye-gaze computer, found out about and gained statutory funding to build a bedroom extension and found a much reduced price for fish oil tablets, used regularly. Although it is difficult to quantify how much each group benefitted from online information, it appears that parents earning more money had received greater lump sum benefits (e.g. the cost of building an extension) through information gained online. However, there were parents within the lowest household income group who discussed the benefits and statutory support they were already claiming – so this may reflect a lack of prior knowledge rather than differences in ability to gain the larger amounts of economic capital available. For instance, one interviewee told me how the council had paid for all the adaptations to her house and additional care for her daughter, which enabled her to care for her daughter full-time. In terms of educational differences, little emerged in terms of actual benefits, with parents across the board gaining actual economic benefits of different kinds, although these did appear to reflect larger economic capital gains for more educated parents. Among parents of adult children and parents in their 50s, no actual economic benefits were discussed in relation to information gained in online peer support forums and only one potential benefit (Disability Living Allowance) was mentioned as having been identified online. This may relate to parents already having a stockpile of relevant expertise and having potentially already having benefitted from such cost savings with information from other sources. There was therefore some suggestion – though speculative – that wealthier, younger and more educated parents may be benefitting disproportionately from economic capital gained through online sources. This is an area worthy of further research as it may contribute to widening inequalities between these groups. It is interesting that most interviewees were accessing similar sites - except one parent who exclusively read blogs – yet it was these groups that appeared most able to convert this expertise into economic capital. This suggests that availability of information is not the key factor here, but how this is used in wider fields.
Emotional and companionship support As noted in Chapter 2, Ferlander’s (2007) notion of emotional support was used here to describe the benefits of support gained online that could not be captured in terms of Bourdieu’s capital benefits. In the survey, 84 per cent of respondents who had used online support described that reading about other parents’ experiences in online support sites made them feel less alone. Fourteen interviewees also noted gaining this benefit from online peer support. This was described in terms of not feeling alone and could apply to reading an account from another parent as well as to interactions. This was connected to the accounts described in Chapter 6 about parents of people with Rett syndrome describing how they felt they were living in a different lifeworld from other parents. These parents described feeling understood and feeling less isolated as a result of reading about other parents’ experiences.
It feels like genuine experience somebody's having. And because it's so similar to your experience, um, it... (pause) makes you feel... less alone.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
As soon as I was invited to join the group (by another Rett Mum), the support was there pretty instantly. As soon as I commented on something or posted something the replies were always very supportive, welcoming, warm and understanding.
[Interviewee #194, mother in her 40s of a 12-year-old girl with Rett syndrome, diagnosed 8 years ago] As noted in Chapter 5, experiencing this benefit was differentiated by years since diagnosis, although as may be remembered, this was not in a linear way. Among interviewees, two of the four parents of preschoolers, all but one of the parents of school-age children and about two of the five parents of adult children had experienced this benefit from online peer support. These differences related to the reduced access to online peer support for one of the preschooler’s parents, who was in the earlier stages of building social capital. However, for the other parent it was an aspect that did not emerge in her account, which focused far more on practical aspects of support. For older parents, emotional support from any source was not mentioned in the interview and may therefore relate to the reduced need for support and navigation of the emotional aspects of the diagnosis related to biographical disruption among older parents or a reduced propensity to seek support overall as discussed in Chapter 6. It might also be related to the stated perception of three of the five interviewees with adult children that online forums were used mainly by parents of children, not adults, which was also supported by data among survey respondents, although this cannot be used to generalise to all users of online support.
For the parents of adult children who did find emotional support online, this benefit could be situation-specific. For one parent, who generally did not seek support from other parents, a link to an American blog written by a parent of a child of a similar age struck a chord.
this is by a parent […] her daughter, her 22-year-old daughter has got Rett. And I read it, and I thought, “She lists things that I felt with [my daughter]”, erm, and sort of, you know, she’s downstairs and she’s got the baby monitor on, for her 22-year-old daughter, who is upstairs in her bedroom watching telly. Erm, but then, what else she said, she was the same as [my daughter] with her like, walking and everything, um and then it’s her thoughts, and I thought, you know, this has gone through my mind as well, that um don’t let anything happen to me because I’ve got to be there to care for her, and don’t dare let her die young, because I can’t bear to lose her, but don’t let her outlive me either, [Husband of 133: Mm] because who’ll take care of her. So it really is, and I mean, [Husband of 133: Yeah] […] So, I don’t very often print things out, but I – as I started reading it I thought, “That is”, you know, “It feels like me”.
[Interviewee #133 and husband, parents of an 18-year-old woman with Rett syndrome, diagnosed 16 years ago]
For the other parent of an adult child this was a case of benefitting from emotional support retrospectively, of being reassured that the way she felt when her daughter was younger was ‘normal’:
[JH: have you ever found it helpful just to read about other parents’ experiences on it or or not really?] Yes. Yes, I think reading other peoples’ experience is always helpful because it’s it’s you feel less alone, even now even after being a carer for 20-something years you still feel oh god all those feelings I had eighteen years ago, it wasn’t just me then, yes, feeling guilty not looking after [my daughter] not doing something for her, mm. [JH: Yeah. That’s really interesting. So it’s it’s it’s not so much how you feel now but it’s sort of looking back and and comparing yourself to how you felt then?] Yes.
[Interviewee #116, mother in her 50s with an adult daughter with Rett syndrome, diagnosed 17 years ago].
As reported in Chapter 5, significantly more parents who held higher education qualifications experienced feeling less alone when reading about other parents’ experiences. There was no evidence in interviews to shed light on this intriguing finding, with interviewees from across different educational groups all reporting this benefit. It is possible that this may relate to reading blogs where one’s parenting practices are supported, but this was not possible to ascertain from this data.
All interviewees were asked about experiencing Ferlander’s notion of ‘companionship’ – “spending social time with others, i.e. leisure time” (Ferlander, 2007) - as a form of support in online peer support sites. For other parents this existed outside the group, because they had met up with some of the parents who used the forum, but here the focus was on companionship experienced purely online. This was relatively rare and tended to take the form of wider conversation not focused on Rett syndrome. Only five interviewees reported experiencing this benefit online.
[JH: And what is that you that you particularly like about it?] Um, well sometimes it’s just the silly bantering about [laughs] anything, about the weather, about about anything really.
[Interviewee #116, mother of a 20-year old woman with Rett syndrome, diagnosed 17 years ago]
so she posted some more recent photos, saying how much she’s grown up and I just got I commented, cos actually [?] they were gorgeous, she was so pretty and I just went, ‘I love her hair,’ it was completely irrelevant, nothing to do with Rett’s at all
[Interviewee #193, mother of a four-year-old girl with Rett syndrome, diagnosed 2 years ago]
Interviewees from across income, education and age groups (although predominantly those aged in their 30s and 40s with school-age children) reported having experienced a companionship benefit from visiting an online support group or site.
7.3 ‘What do I know, I’m just a mother’: converting online ‘goods’ into symbolic power in wider caring fields This section explores social differentiation in how capitals gained online are converted into symbolic capital in wider caring fields. As noted in Chapter 2, parents faced a number of challenges within wider fields including medicine, education and social care. These included gaining a diagnosis from medical professionals and access to other ‘goods’ and resources in these fields, such as access to certain kinds of treatments and therapies. A vivid example of the less powerful position held, even by parents with greater initial cultural capital through education, was given in the following account by a parent who held a Masters qualification in a Psychology-related topic.
When [my daughter], before she had her diagnosis... was going through a regression... I... was told that she was Autistic, most likely [JH: Mm-hm] Which I did not believe [JH: yeah] Um... I like to think I know enough about... er Autism or you know - psychological things generally [JH: Mm- hm] and I'm her mum [JH: Yeah] But... eh - when I said I didn't think it was Autism, basically what I was told was, um, yeah, we're not sure it's Autism either, it could be one of a hundred things. We're investigating Autism because we think that's what it is [inhales] but it's not clear, um, particularly because she made really great eye contact and she's very loving, which is typical of Rett girls. Um, but ultimately that I - what do I know, I'm just a mother and, not only that, that mothers compensate, that they see what they want to see, not the reality, so, for example, I... said ‘she's losing words, she's losing words, she's losing words’ and I was told, 'she's not losing words... she never had those words, you think you heard them because mothers want to hear words, she was babbling, you heard words you wanted to hear, and that's good', I was told, ‘because we'll do that because when we - think we've heard a word we act as if we've heard the word, the child learns to say it again, it becomes a word’, but that, be-c- that - I had - never heard those words so [my daughter] had never lost them. [Inhales] None of which I agreed with (laughs) [JH: No (laughs) of course not.] Er-hum, but I was uncertain - and very anxious, so, I started to read for myself and I read a lot. [JH: Yeah] about Autism. [Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
This section explores how parents used or ‘borrowed’ (after McKeever & Miller, 2004) ‘goods’ gained online in order to gain the symbolic power necessary to access additional support and equipment within wider caring fields. Interviewee #118, quoted above, was very active in gathering information that she could use as ‘ammunition’. As noted above, this was like the ‘borrowed’ capital described by McKeever & Miller (2004), only the expertise borrowed was from other, more experienced parents, not professionals.
But then also other people's experiences even if they're not relevant now, ok [?] [JH: Yeah]. I read a really long chain of comments, um on the blog I mentioned where... one of the little girls had - cos they had the feeding tube and the button that's in their tummy had fallen out [JH: OK] and they had been told by the Nurse that that never happens, they didn't need a spare [JH: Right] And in the middle of the night it did happen [JH: Yeah] and it was a crisis [JH: Yeah] And then there was a lot of comment on how it had happened to other people [JH: OK] and I sort of - although that's not relevant to us at the minute [JH: Yeah] I filed it away in my head [JH: Yeah] that when a Nurse helpfully tells me [JH: Yeah] that we don't need a spare and I don't know – need [JH:Yeah] to learn how to... sort it out, I can say, no, no [JH: Yeah] I know that lots of parents have had this problem and you must teach me this.
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
One important function of the online peer support groups was of what parents termed ‘moral support’ in deciding when to engage in a symbolic capital struggle in a wider field. One parent described how support online had given her ‘the strength’ to challenge a local decision to exclude her daughter from horse riding. my daughter’s ridden since she was about three. [JH: Yeah.] Infrequently, but this school, because she’s got seizures, is refusing riding lessons. [JH: Yup.] And I st-. I know I need to deal with that with her epilepsy consultant, erm, but I did vent. I went on[line] and vented. [JH: Yeah.] Er, because one of the parents is a is a you know is a she has horses with a daughter with a disability. So she knows what the issues are. She knows what the health and safety controls are, and the risk assessments. And it helps that, you know, other people support you. [JH: Yeah.] That you’re not wrong for realising that their decision is wrong. [JH: Yeah, yeah.] And I think on that was on [two of the peer support sites], I think at round about the same time, some child they [inaudible] to take them to riding lessons because they had seizures. So there’s along along the same lines and it happened at the same time. [JH: Mm.] So, I think we all vented together. [JH: Yeah, yeah. OK.] And I think sometimes when you you’re told ‘no’, by a body or a community, the easiest thing to do is just to say ‘fine, OK’ and back off. And I think if you get the support from other parents, so [?] no they’re not always right, again, parents aren’t always right but, um I think sometimes you need some moral um support to say ‘you need to fight that one’ [JH: Yeah, so it sort of helps you to choose your battles, in a way?] Yeah, yeah. [JH: Yeah. OK.] And again, you know, parents aren’t always right. Um, but if you get the moral support or you get the knowledge from other families who’ve gone through it, it does give you, you know, the strength to carry on.
[Interviewee #25, mother in her 40s of an 8-year-old-girl with Rett syndrome, diagnosed six years ago]
For this parent, who lived in the United Arab Emirates, but used European and American sites, parental support helped him to feel supported to make radical dietary changes in the face of medical skepticism.
So we took our daughter and, er, it was telling doctors, “Doctors, my daughter had a big traditional meal rich of wheat, does that mean something?’ [JH: Yeah.] Doctors, they take the medicine, the the blood sample, they make the test and they come with negative answer and I do feel, I do, I do found the, do find er two respondents, saying, “don’t listen to those stupid doctors.” [JH: Right.] “Fee- uh listen to your gut.” [JH: Yeah, yeah.] And, and I do believe in this. [JH: Yeah.] And er, erm, just after that I stopped giving her wheat derivatives or bread, cake, macaroni, spaghetti, everything stopped. [JH: Yeah.] Okay. Er, no seizures… [JH: Wow.] …for two months…[JH: Great.] …for two months and then came back, [JH: Oh] the seizures came back. [JH: Yeah.] And er the doctor say, “See, seizures have come back, so are you happy that seizures have come to prove your po- your, your argument.” I just said “No, but you were saying that those uh stupid websites, that was the [inaudible] they used. Stupid website groups that are talking about this subject um and now you know, doctors, they think, it’s very difficult to change the mind of a doctor. [JH: Yeah, yeah.] You know, because he used to study things scientifically and he will never understand something, he will never accept something which is not proven. [JH: Okay, yeah, yeah yeah.] That’s it. So I returned after three months giving my daughter bread […] And, erm, seizures are the same, till one day we had, er, traditional meal […] it’s a complete green wheat. [JH: Right.] […] and uh uh that day my daughter got four major, er, er seizures. [JH: Yeah.] You know, it is like, those seizures have been like you have a bulldozer sitting on my daughter, how she was squeezed and her body is moving, it’s like a bulldozer sitting on it. [JH: Yeah, yeah.] So I went back to the hospital. We admitted her in the hospital for, erm, a day and I told the doctor, “She had wheat again and this happened.” [JH: Yeah.] And the doctor insisted that one as a rational man I accept the scientific side, that’s my, that’s how I have been raised. [JH: Yeah.] […] When I go to the site again the parents agree with me, “Don’t listen to doctors, stop wheat, stop bread, stop cakes, stop, er, spaghetti, stop everything even don’t give her hamburger, ‘cause hamburger itself has some wheat in it.” […] And I stopped everything again, although I did the gluten uh antibodies test and it came negative. [JH: Mm hm.] I did, er, er, […] we have taken a sample from her intestine, okay, to test, erm, what do you call it, erm, er, cyclic disease […] came negative. And when my daughter takes wheat… [JH: Yeah.] …she gets major seizures […] I don’t personally, I don’t believe that if I didn’t have that insistence from those parents, “Don’t give her wheat anymore, don’t listen to those, er, doctors, telling you no, she has nothing related to gluten,” I would have continued giving her wheat…
[Interviewee #141, father in his 40s of a 13-year-old young woman with Rett syndrome, diagnosed eight years ago]
For more experienced parents, the forums could be used to encourage other parents to challenge medical decisions and to trust their own instincts.
and that’s where, you know what, as a younger parent with a young Rett girl [JH: yeah] you don’t know that you can stand up for yourself and say, ‘No!’ [JH: yeah] ‘I don’t want you to do that’ [JH: yeah yeah] I put a bit of that out on there, which I suppose is a bit negative, if you’re not happy with that, that or what’s done [JH: Mm-hm] ask to see somebody else. [JH: Yeah] refer it back you know, [JH: yeah yeah yeah] people don’t realise they can do that [JH: yeah] people don’t realise they can’t [sic] stand up to Doctors […] [JH: so you’ve, having had those experiences you’re able to say to people on the forum you don’t have to put up with this, and to trust your your opinion and so on] Gut instinct! Gut instinct [JH: Yeah. Yeah yeah.] is right you know that happens with lots of people [JH: Yeah] It’s like they say when people get mugged [JH: Mm-hm] they they reckon there’s a thirty second window before you get mugged that actually there’s that fight or flight or fight [JH: yeah] and do you, you know what you’re gonna do [JH: Yeah yeah] that person doesn’t look like it’s gonna mug you, but something tells you that [JH: yeah] something’s not right and I think it’s the same with girls [JH: yeah yeah] with Rett girls [JH: yeah] and actually if you watch their body language [JH: yeah] you’ve got a pretty good idea at what’s right or wrong with Rett girls [Interviewee #174, mother in her 40s of a 14-year-old young woman with Rett syndrome, formally diagnosed eight years ago although mother realised 12 years ago]
However, not all parents were prepared to challenge medical advice. As discussed in section 7.2, this could be interpreted as relating to habitus connected to beliefs around the relative importance of peer and professional advice or having access to trusted medical support. However, it could also be due to having a bad experience following peer advice, as in the account quoted below. This account is interesting in terms of how this interviewee presents both being willing to take peer advice on medication, but also presents herself as tending to defer to her doctor’s view – indeed seeking her doctor’s advice before making this change. As can be seen, this interviewee was younger than the other parents quoted in section 7.2.
she was telling me that I should take her off one of the tablets that she’s on [JH: Ooh. Mm.] Which, um with agreeing with the Doctor we did [JH: Yup] but we took her off it immediately which then caused withdrawal and she ended up in hospital for a week having convulsions and [JH: Ooh] getting all shakes so I think she was withdrawing from the drug [JH: Yeah yeah] and we just took her off and just changed her over but now we’ve put her back on and I don’t really talk to this [laughing slightly] other parent anymore [JH: No] but she’s very sort of this one was very sort of herbal, herbal remedies and things like that as well and trying to get her daughter off all her drugs and you know [JH: Mm] […] generally I go along with what the Doctor tells me and you know if they say this is the one that’s best for her I’ll give it to her, you know [JH: Yeah] I don’t tend to, then go researching into all the problems that it could cause, I just sort of [JH: Yeah] give it to her and go along with it.
[Interviewee #30, mother in her 30s of a 12-year-old girl with Rett syndrome, diagnosed 9 years ago] Another helpful aspect of online support groups was having access to wider knowledge about what had been funded in other authority areas. Two parents who held higher education qualifications discussed their current attempts to use this kind of information to change their child’s situation within wider caring fields. They differed in terms of household income, one being a single parent reliant on benefits to care for her daughter, the other parent earning over £40,000 per year.
hearing, uh, what other people, do, and h-have been able to get or or whatever that kind of [JH: Yeah] that can be quite empowering [JH: Yeah] to get a better sense of, you know, what might be available if only you know what to ask for [JH: Oh ok] all that can help [JH: Yeah] Um, so yeah, there’s lots of good advice [JH: Ok] about things like that [JH: Can you think of an example where you saw something that made you think differently about what what you could, what was available and] Um, well I gave the example of music therapy, [JH: oh yeah] I haven’t managed to, I haven’t been successful with it yet, but [JH: Yeah, yeah] uh, it was very useful to know that there are lots of girls who do have music therapy on their Statement [JH: Ok, yeah] you [inaudible], there’s no there’s no intrinsic reason why it shouldn’t be done.
[Interviewee #76, mother in her 40s of a 5-year-old girl with Rett syndrome, diagnosed 3 years ago].
and someone’s coming to look at eye tech gaze technology with her [JH: Oh yeah] I was unaware of eye-gaze technology [JH: Ok. and you found about that through the] Yeah [JH: (the online peer support group)] Yeah.
[Interviewee #174, mother in her 40s of a 14-year-old young woman with Rett syndrome, formally diagnosed eight years ago although mother realised 12 years ago] As noted above, peer support groups sometimes involved the sharing of reports that had been used to gain funding for services. This was described by the following interviewee as something that online peer support could offer that institutions (charitable organisations) could not offer
and... um, yeah, hearing about, what other people have been able to… do, so, for example, um, yeah th- there’s b- there was some sharing of um Speech and Language Therapy reports [JH: Yeah] that were written in support of funding [JH: Oh ok] for an eye-gaze computer [JH: Yeah, yeah] that kind of thing [JH: Ok] So you see, that’s the kind of thing that’s shared among parents that I just don’t think a [non- peer, charitable] organisation […] is in a position to help with [JH: Yeah] you know, we we just do it ourselves and they don’t have, you know, there’s there’s things they can add [JH: Yeah] but, e-, yeah, sharing that experience is really [JH: Yeah, yeah] is really good
[Interviewee #76, mother in her 40s of a 5-year-old girl with Rett syndrome, diagnosed 3 years ago].
In support of this idea, one couple described how they had not been able to get information about challenging services from a charity.
Because we thought…well, it wasn’t them first of all but they did come into it, because I thought, “Well, they’re the experts on Rett. […] they may suddenly come up with all these things like, ‘Oh yeah, we’ve had other families that have been through this fight and they’ve got what they wanted’, or you know, something like that, because they’ve gone about it in this way”, but actually, they didn’t, did they? [JH: Mm. Okay.] So I gave up on them. [JH: Yeah.] Um because they just said, “Oh well, you know, it’s very difficult. The economy is this, that and the other…”[Husband of 133: I think through all this thing we were by ourselves.] Yeah, we were by ourselves in the end. [Interviewee #133 and husband, parents of an 18-year-old woman with Rett syndrome, diagnosed 16 years ago]
Three parents discussed having gained a tangible benefit in wider caring fields through information gleaned from online support groups. All three were parents of children rather than adults with Rett syndrome.
if there's a new - intervention or some therapy or [JH: Yup] something, then I would want to know about that. [JH: Mm-hm] Um, and that's been really helpful for me [JH: Yeah] Because, one of the things I've done is, I managed to get hydrotherapy onto [my daughter’s] statement, which in [local area] is very rare [JH: Yeah] they don't put hydrotherapy on statements [JH: Ok] That's their view [JH: Yeah] Um, but I was able to go in with articles [JH: Yup] That showed that hydrotherapy's really good for girls with Rett syndrome [JH: Ok] Um and that I really felt it had to be on. [JH: Yup] Um, and in the end, they er, got tired of me phoning I think [JH: yeah] [Laughs] and [JH Laughs] put hydrotherapy on her statement
[Interviewee #118, mother in her 30s of a 4-year old girl with Rett syndrome, diagnosed a year ago]
Um and I think one of the threads was basically about um incontinence pads. [JH: OK.] Cos I live in an area that was rationing incontinence pads. [JH: Oh yeah, yeah.] And it was basically through Mumsnet that I realised that what they were doing wasn’t right. [JH: Yeah.] So we’ve gone through a long process, appealed and we finally got there.
[Interviewee #25, mother in her 40s of an 8-year-old-girl with Rett syndrome, diagnosed six years ago]
I wanted to get [my daughter] a Peapod chair [JH: Mm-hm] Um and I had been looking at it and I said, as- said to people, you know is there any places I can get funding for this [JH: yeah] um and someone suggested trying the OT before I went down the route of getting a grant [JH: Mm-hm?] because you know it’s a chair that she needs [JH: Yup] um and I followed their advice and the OT paid for it.
[Interviewee #30, mother in her 30s of a 12-year-old girl with Rett syndrome, diagnosed 9 years ago]
Overall there was no strong evidence that wealthier or more educated parents had unequal gains in terms of converting online ‘goods’ into symbolic capital in wider fields, with parents with basic levels of education and lower earnings both able to reap the benefits of the information available online. Thus access to a wider group of peers online gave some parents the opportunity to discover when a local decision had been challenged or had not been applied in another area and provided a space where parental experience or ‘gut instinct’ could be privileged over medical expertise. However, picking up a key finding within this research, none of the parents who described having sought or gained symbolic capital in wider caring fields had adult children. There were a number of possible reasons for this difference, which reflect the findings described in Chapter 6. Firstly, one parent of an adult children described having gained similar benefits from an offline source: information about seizures at a Rett UK event that led to gaining a referral to a specialist clinic. This reflects the greater social capital resources that interviewees with adult children may have drawn upon over time. Secondly, as noted in the section about similarity to other posters and reflected in the survey findings, a significantly smaller proportion of parents of older children and parents of children who had received a diagnosis more than seven years ago reported experiencing benefits from online support sites. As noted above and argued in Chapter 6, this reflected parents’ perceptions and survey findings that suggested that online support groups were used disproportionately by younger parents and the ‘goods’ available there were largely irrelevant to older parents, save for information about emerging treatments and research and some new equipment. Thirdly, as discussed in Chapter 6, the volume of novel difficulties faced may have reduced, with parents already having in place strategies, equipment and support to meet many of their daughter’s needs. Finally, there was some limited evidence that older parents may be less disposed towards challenging medical professionals, although this could also be explained by the possibility of having found helpful professional allies who could advocate for them, raised in Chapter 6.
7.4 The role of online peer support sites within wider caring fields and existing power structures
This chapter aimed to explore the position of online peer support sites within wider power structures in terms of both wider social (and digital) inequalities and institutional interests within wider caring fields. Section 7.1 presented data that suggested that institutional and elite voices are privileged in Facebook Pages and parents’ blogs (partly due to the architecture of these sites) and that even in online peer support sites such as Facebook Groups, wider symbolic struggles among institutions can be played out among parents. In this way, some aspects of online peer support among this group of interviewees can effectively suppress or sideline the voices and views of less powerful individuals. Section 7.2 problematised the notion of distinct ‘lay’ and institutional sources of information online, noting how interviewees and institutions used online peer support sites to link to communications from wider fields, such as research. There was some support for the idea raised in Chapter 6 that some interviewees holding greater cultural and specific kinds of linguistic capital can access and understand a wider range of primary sources, particularly research papers. There was also some suggestion that more educated interviewees used strategies to discover the meaning of unknown jargon that less educated parents did not. However, without a wider knowledge of the range of information sources parents had ever accessed, it was difficult to draw conclusions for the whole interviewee group. Where information ‘goods’ had ever been gained from online sources, many aspects did not appear to be socially differentiated among interviewees, suggesting some democratic sharing of some kinds of information in certain forums (‘case history’ information, services outside education, specialist equipment, expert carer work into developments in therapies and research). This included parents with basic or secondary education accessing professional advice from Speech and Language Therapists in an online peer support group. There were a few indications of some possible differentiation in some areas of expertise. Some interviewees who were also wealthier and more educated sought medical information and information about special educational needs online. Parents of adult children did not report having used online peer support sites for suggestions about daily care, special educational needs and medical information. This may reflect a combination of differing needs, a lack of relevant ‘goods’ within groups and differing habitus with relation to peer- professional relationships. However, these findings were limited to topics discussed by parents within the interviews, so may not be exhaustive and cannot be generalised to a wider group of parents or even survey respondents. In addition, the method of sampling may have over selected parents who may be more actively involved in information and support seeking. There was some suggestion that wealthier, younger and more educated parents may have gained greater economic capital benefits from the information found through online support groups, however this cannot reflect how these benefits may have been gained through other sources of information offline, or already have been gained before online support was used. Finally, emotional support and companionship could be experienced across all groups from online peer support sources, although this was predominantly experienced by younger parents. Section 7.3 explored how online ‘goods’ were converted into symbolic capital in wider caring fields. This shed some light on how online peer support interactions can influence relationships with professionals. Some parents described how they ‘borrowed’ other parents’ expertise to challenge medical decisions, using online discussions as sources of moral support or evidence for certain approaches. However, not all parents were prepared to do so, reflecting earlier discussions about parents’ disposition towards challenging medics. There was no compelling evidence in interviewees’ accounts that wealthier or more educated parents had unequal gains in terms of successfully converting online capital into symbolic capital in wider caring fields. Again, none of the parents who discussed using online support ‘goods’ to seek or gain symbolic capital in wider caring fields were parents of adult children. This may relate to a number of differences in the experiences of parents of adult children as discussed in this chapter and Chapter 6, or to having already gained these kinds of benefits through alternative sources or not recalling these benefits in an interview due to elapsed time since this had happened. Chapter 8 closes this thesis by bringing together the findings reported so far, interpreting how they have addressed the research questions and assessing the contribution to the literature outlined in Chapters 2 and 3. Chapter 8. Towards a more coherent understanding: the role of online support and information in the caring practices of parents of people with a rare syndrome
This chapter draws together the findings of this thesis, assessing how they have answered each of the research questions and how they contribute to existing literature on the role of online support and information in the lives of parents of people with rare syndromes. In this thesis I set out to provide a more coherent understanding of the role of online support and information in the lives of parents of people with a rare syndrome. It has been argued that online information and support could provide particular benefits for this group due to the lack of expertise among local health professionals and a likely lack of contact with peers whose children face the same issues. However, very little research has explored the role of online peer support within this group. Existing literature exploring the use of online information and support among carers of people with rare syndromes is fragmented and has either focused on mostly qualitative micro processes of the use of online information and support or mostly quantitative macro studies of the differentiation of use. In Chapters 3 and 4 I argued that this fragmentation was related to a theoretical pluralism in the wider field. This reflected wider epistemological divisions that focused either on the structural inequalities involved in accessing online support and information or on descriptions of individual practices. I proposed that Bourdieu’s concepts of social, economic and cultural capital, fields and habitus might provide a way to explore how both structure and agency might be involved in the use of online support and information in everyday caring practices. In particular, I posed four research questions, which were:
1. Are younger, wealthier and more educated parents of people with Rett syndrome more likely to use online support and information than others? 2. Are different platforms for online peer support socially differentiated so that parents of people with Rett syndrome are brought together ‘in a seemingly fortuitous way’? 3. How does an individual’s habitus and possession of different forms of relevant cultural and social capital affect their use of caring-related online support and information? 4. How does the use of online peer support sites influence wider caring practices? Is there any evidence of differentiation of benefits by age, income or education?
I argued that the best way to explore these questions was with a mixed method approach, combining survey and interviews to explore use within a single case study group of parents of people with a specific rare condition: Rett syndrome. The following sections summarise my findings in relation to these four research questions. Within each section I assess the limitations, strengths and contribution of this work to the wider literature. I conclude this thesis with a summary of how this work has changed this field and suggestions for further research.
8.1 The social differentiation of online peer support and information use
Are younger, wealthier and more educated parents of people with Rett syndrome more likely to use online support and information than others?
This section assesses the attempt to answer the above research question. In doing so it draws together the rationale behind exploring the structural differentiation of the use of online support within a case study group of parents of people with Rett syndrome, and describes the contribution to existing findings. 8.1.1 Assessing structural differentiation among a case study group of parents of people with Rett syndrome Following the reasoning of Bourdieu (1984) and the methodological recommendations of Fries (2009) and Harrits (2011), I began my study by trying to establish whether there was any evidence of structural differentiation of the use of the Internet for caring-related information and support within this group. Due to the rare nature of Rett syndrome and the lack of a comprehensive sampling frame, it was not possible to draw a large or a randomised sample of parents. This meant that my findings could not be generalised to the wider population of parents of people with Rett syndrome, but instead served as a large case study group from which interviewees were drawn. Comparisons with Rett UK’s membership database, the most up-to-date sampling frame available, suggested that women and full-time carers might have been over-represented in my sample. However, these groups may provide the richest data about how online support and information relates to household caring practices. A follow-up question about non-response suggested that at least some parents who did not use the Internet had not responded due to a lack of interest in this topic. It is also possible that, due to the available sample frames used (Rett UK members and online support sites) my sample were particularly engaged users of information and support. However, my main focus in this study was on how current users of online support and information use this within their wider caring practices, so this bias did not affect my ability to explore this area. Therefore, as intended I was able to explore the interplay of structural and micro processes in the use of online information and support within the wider caring practices of this case study group. As outlined in Chapter 2, existing research into the use of the Internet by carers is methodologically flawed and research into micro-processes tends to be based on relatively small samples. This research therefore contributes a larger (effectively qualitative) study to the limited research into the use of the Internet – and particularly online peer support sites – among parents of people with rare syndromes. Moreover, by combining quantitative and qualitative data within the same wider case study group, this research is novel in presenting a coherent picture of the uses of online support and information at both a macro and micro level within the same case study group of carers of people with a particular rare syndrome. As argued in Chapter 1, this is valuable for two reasons. Firstly, because it avoids confounding results among carers providing different kinds of care, for different periods of time to people with different support needs. Secondly, because Rett syndrome is a good early example of the repercussions of the Human Genome Project on the use of information and support available to carers of – and people with – specific genetic syndromes. This, as noted in Chapter 2, has already changed the nature of genetic knowledge, available technology and the kinds of online information and support available (Skinner & Schaffer, 2006).
8.1.2 Interpreting the social differentiation of the use of online support among respondents Internet users were likely to be overrepresented in my sample, but even so, Internet use was not ubiquitous and reflected OxIS findings (Dutton & Blank, 2013) in that income and age were strongly related to use. This is an important finding in that it establishes that even though the Internet provides great potential for carers, it is not used universally and social differentiation of use may reflect wider digital inequalities. The most striking aspect of the survey findings was the low role that income (economic capital) and education (cultural capital) played in differentiating the use of online support in caring practices among respondents. This ran counter to existing research, which suggested that a greater proportion of professionals used a Rett syndrome-specific online peer support group (Leonard et al., 2004). However, this research was itself limited in its ability to generalise to the general population of parents of people with Rett syndrome as respondents were recruited through a single email group. This may have led to the over selection of active, current users of this specific forum, who may not reflect the wider group that has ever used any kind of online peer support. One possible reason for the lack of a relationship with income was a relatively large number of full-time carers in my sample, even when compared to the sampling frame from Rett UK. These families would have reduced overall household income compared with the general population. However, this does not explain the lack of differentiation by higher education, which was found by both Leonard and colleagues (2004) and Porter & Edirippulige (2007)40. However, as both these other studies were not representative of their wider populations either, neither can really shed light upon wider use. Instead, the key differentiating factor among respondents was age and other time-related variables (child’s age and years since diagnosis). As might be suspected there were high correlations between these three variables as all ultimately related to time. A significantly larger proportion of younger parents had ever used generic online support41. Significantly more younger parents, parents of younger children and of children who received a diagnosis more recently had ever used online peer support, and significantly more parents of younger children and those with a more recent diagnosis had visited an online peer support site within the last month42. Having mobile access to the Internet and having a higher self-rated ability to use the Internet were also associated with ever having used generic online support and online peer support. In line with findings among the general population (Dutton & Blank, 2013), increased age was highly related to lower use of mobile access and lower self-rated Internet use ability. This suggested the possible role of a form of generational digital inequality among older parents within this sample, arguably related to distinguishing practices (not using mobile access to the Internet) and possibly fewer opportunities to develop online skills (although this could not be tested here). As noted in Chapter 5, due to the small sample and problems of multicollinearity, it was not possible to test the relative importance of each variable. However it was argued that artificially disaggregating these influences on the use of the Internet would provide limited information in understanding how micro processes fitted within wider structural differentiation. Instead an appreciation of the intersection of multiple structural influences on the lives of interviewees was a valuable context within which to explore the use of online support and information within everyday caring practices.
40 Unlike Leonard and colleagues (2005), Porter and Edirippulige (2007) sent a survey to a wider group of parents, although, as noted in Chapter 2, their recruiting method was limited and this work was also not generalisable. 41 Comparisons across age of child and years since diagnosis could not be carried out. 42 Comparisons by age of parent could not be carried out Chapter 6 presented interviewees’ accounts to explore how these intersecting variables provided a context for the differentiated use of online support. These revealed changes over time relating to the changing care needs of a child with Rett syndrome, parents’ management of the biographical disruption involved in receiving a diagnosis, accumulation of relevant expertise and finding and narrowing down social capital resources. These are all explored under the other sections of this chapter as they relate variously to possession of habitus and related practices and tastes, and social capital (see section 8.3) and the differentiation of benefits gained from online support (see section 8.4). It was not possible to disentangle the relative impacts of time, age of parent, cohort of parent, age of child and the changing nature of communication and fields of knowledge and support. However, interpreting these intersecting influences on parents’ use of online support was valuable in exploring the necessarily socially and historically situated nature of parents’ practices. This thesis therefore follows Bourdieu's (1993) argument that practices can only be properly understood within their specific socio-historical context. In conclusion, this first research question could only be answered among this group of respondents, but provided an informative case study of the practices of a large group of parents of people with a specific rare syndrome. Among respondents, younger parents – but also parents of younger children and children with a more recent diagnosis – were most likely to have ever used online peer support. Except for economic capital differentiation in the use of the Internet, economic and cultural capital did not affect the use of online support. Section 8.3 summarises findings that explored how parents’ possession of alternative forms of social capital and relevant ‘goods’ was related to these forms of age- and time- related differentiation.
8.2 Fortuitously among like others? The social differentiation of online peer support sites Are different platforms for online peer support socially differentiated so that parents of people with Rett syndrome are brought together ‘in a seemingly fortuitous way’?
On the whole, and in line with Dutton and Blank’s (2013) findings, the use of all online support platforms was socially differentiated by age of parent and age of child and - except for website comments - by years since diagnosis. This followed the pattern outlined above, where use was highest among the youngest parents, parents of younger children and parents of children who had received their diagnosis more recently43. However, as before, these results did not reflect results in the wider population (Dutton & Blank, 2013) because income did not differentiate use except among blog use, which is discussed in detail later in this section. Facebook was the most used platform for online peer support among current Internet users within the survey sample (59%) and the use of Facebook Groups and Pages were a prominent feature of interviews, so deserve particular attention here. Within the survey respondent sample, older parents were underrepresented44 and interviewees with adult children perceived such groups as predominantly used by parents of children, which was also reflected in the statistics available on survey respondents45. In interviewee accounts, parents of adults suggested that this age imbalance meant Facebook Groups provided no relevant ‘goods’ in terms of parental advice about daily caring. Interview accounts described in Chapter 7 suggested that wider institutional interests were reflected within Facebook sources of peer support. Firstly, Facebook Pages for charities - although sometimes initially perceived by interviewees as possible sites to contact peers - were structured to privilege the views of the organisation over those who visit the page46. This is a good example
43 As noted above, these variables are highly correlated, so these groups are likely to overlap and provide, as argued above, evidence of multiple, interrelated structural constraints within interviewees’ lived experiences. 44 46.4% of 45-66 year old respondents and 20% of 67-89 year old respondents used these groups compared to 87.1% of 23-44 year old respondents. 45 78.0% of survey respondents with children aged under 18 used Facebook while only 37.9% of respondents with adult children did. 46 As noted in Chapter 7, Facebook Pages and Groups are designed for different purposes. Facebook Pages are ‘official profiles’ for businesses and brands, while of the importance of considering the impact of online algorithms and technology on the social use of the Internet, as discussed in Chapter 2 (Halford & Carrigan, 2014; Kivits, 2013; Seale, 2005). Although parents did not quote Facebook policy, some interviewees became aware the limitation of Pages through failed attempts to engage with other parents and an awareness that comments added by visitors to the Page were automatically given less prominence than posts by the organisation. This changed how interviewees used these kinds of pages in terms of the language they used and the questions they asked (those befitting formal communication with an organisation). Secondly, the ideological approaches of different charities – in essence, fundraising for parental support or for ‘cure’ or treatment research – were reflected in symbolic struggles within Facebook Groups. As I argued in Chapter 7, these aspects of Facebook Groups and Pages showed how wider institutional power structures were represented and reproduced in an undemocratic way. This ran counter to ‘celebratory’ theories about online support being inherently empowering and was more supportive of the ‘contingent’ perspective to online support outlined in Chapter 2 (Nettleton et al., 2005). It also supports the idea of an e-scape where sites managed by biomedical and commercial interests are represented alongside ‘lay’ health knowledge (Nettleton, 2004b) – sometimes in the same online space. Additionally, it adds support to arguments that online support and at least certain parts of the Internet should be understood as reflecting subfields of wider fields (Smith & Stewart, 2012; Sterne, 2003) rather than treating the Internet as a separate field (Julien, 2014). Interestingly - in a finding that initially appears to reflect some of the early ‘utopian’ research into the potential for the Internet to be a place of relative equality – interviewees reported finding it hard to establish someone’s social background through Facebook group contact. This is a surprising finding given that Facebook users are not anonymous and share ostensibly personal information on their profiles. One interviewee described how a lack of the cues present in someone’s voice – potentially an indicator of linguistic or cultural
Facebook groups “are the place for small group communication and for people to share their common interests and express their opinion” (https://www.facebook.com/notes/facebook/facebook-tips-whats-the- difference-between-a-facebook-page-and-group/324706977130) capital - was one aspect that was seen as missing in making this kind of judgement. Another interviewee, who was a single parent, was aware that nobody online knew this aspect of her background and she told me she not stated this in any obvious way on her profile or during her interactions within the group. However, as argued below, aspects of practice and taste were used to differentiate Facebook contacts with whom one might have an ‘affinity’, which suggested parents were attuned to differences in markers in habitus that indicated social position (after Bourdieu’s conceptualisation in Distinction, 1984). As noted in the previous section, blogs were the only place where there was clear social differentiation by income, with greater use by wealthier survey respondents. There was evidence within the interview data reported in Chapters 6 and 7 of how this differentiation in blog use affected parents’ experiences of online peer support. This was reflected in how interviewees described the ‘likeness’ of others, with one wealthier and more educated parent describing how she felt a particular affinity with a blogger, who wrote well and who had quotes on her blog that she liked, which suggested indications of shared cultural capital and taste, reflecting shared habitus. Another interviewee who wrote a blog only tended to respond to other bloggers’ posts and avoided Facebook because she felt it would not involve contributing toward the relationships she had built up with other parents within the blogging community. She instead chose to share information about useful equipment on her blog. However, if survey and interview results were any indication, this may mean there was less likelihood of this information being seen by less privileged parents. This recalled Bourdieu’s (1986) description of how differentiated forms of social capital require exchanges that are ‘subjectively felt’ as ‘durable obligations’ (Bourdieu, 1986, p. 52). This did not appear to be driven by a deliberate attempt to exclude dissimilar others, but was something that happened as a result of being part of this particular group. This was similar to what Bourdieu (1986) has argued in relation to the operation of social settings that bring together homogenous groups of people in a ‘seemingly fortuitous’ way. While blogs were also ostensibly a place where parents could exchange messages with one another47, some interviewees’ accounts suggested that
47 Therefore reflecting my conceptualisation of an ‘online support site’. bloggers held greater symbolic power because, through their posts, they set the agenda for the discussions in the comments below. Another aspect of this power was reflected in the accounts of the two bloggers interviewed, who reported very little or no challenges to the content of their posts, which would touch on aspects of parenting practices48. This suggests both a possible sharing of habitus with the wealthier, younger survey respondents who read these blogs and how bloggers’ voices could be privileged over the views of their peers. Given the wider evidence of blogs being produced more often by wealthier people (Dutton & Blank, 2013), this suggests that the views of wealthier parents in the Rett syndrome blogosphere may be privileged, although this can only be suggested by this data, which cannot be generalised more widely to the whole population of parents using these sites and groups.
In summary, in relation to the research question posed above, there was evidence that blogs were socially differentiated and functioned as places where a disproportionate proportion of wealthier respondents could find ‘like’ others, support one another and share expertise. Additionally, there was some evidence of some voices and views that reflected institutional ideologies holding additional symbolic power within Facebook Pages, but also, to a certain extent, within Facebook Groups, where wider institutional ideologies and symbolic struggles could be reproduced.
8.3 The role of habitus and cultural and social capital in the use of online support and information
How does an individual’s habitus and possession of different forms of relevant cultural and social capital affect their use of caring-related online support and information?
48 This was in contrast to the existence of conflicts in Facebook Groups about parenting practices, which were described as a relatively more common experience. This question was explored in Chapters 6 and 7, as it relied upon qualitative data that could shed light on micro practices in information seeking and how they might relate to parents’ dispositions (habitus), possession of cultural capital (education) and social capital (alternative sources of support). As I argued in Chapters 2 and 3, a coherent understanding of the role of online support needed to take into account parents’ access to alternative sources of social capital, their possession of cultural capital, and the influence of habitus on information- seeking, parenting and online practices. These aspects are explored below in terms of the findings reported in previous chapters and how they contribute to the existing literature outlined in Chapters 2 and 3.
8.3.1 The influence of alternative social capital resources on the use of online support Interviewees reported drawing upon a range of sources of information alongside online support, and in some cases, before they had access to online support. In fact, among survey respondents, a lower proportion had ever used online peer support (66.8%) than had used local group support (80.2%), telephone support (82.4%), or generic online support (89.3%). Other sources of support mentioned in interviews included books, magazines, telephoning volunteers, attending charity-run events, reading charities’ newsletters and magazines, talking to other parents of people with Rett syndrome they knew offline, attending specialist Rett clinics run through Rett UK and consulting a genetic specialist at Great Ormond Street Hospital. This interweaving of online and offline sources of support recalls the arguments presented in Chapter 2 on the importance of understanding the use of the Internet as part of everyday life, with the underlying dynamics of communication (in this case, information seeking) being the focus of research rather than the medium itself (Baym, 2009). In interviews, parents described using whichever relevant sources of information were available at the time and their use being driven by level of need. Therefore while many interviewees described a period of intensive information gathering around the time of diagnosis, this was carried out using whichever channels of information were available at the time, both online and offline. As argued in Chapter 6, parents tended to narrow these sources of social capital to trusted allies and ‘like’ others over time. Sometimes this meant taking online contacts made in online support groups offline. In choosing whether or not to use an online peer support site, interviewees reported weighing up the alternative sources of support and information available to them at the time. This was often related to the kinds of ‘goods’ that were offered by a particular online peer support site in relation to other sources of information and support, which is explored in section 8.4. Aspects of habitus fit and misfit, which is explored in section 8.3.3, also influenced use of different sources.
8.3.2 The influence of cultural capital on the use of online support sites and information The survey found no significant differences in the use of online peer support and generic online support among parents of people with different levels of education (cultural capital). As will be discussed in section 8.4, there appeared to be no additional apparent benefits accruing to those holding more cultural capital. However, as discussed in Chapters 6 and 7, there was some evidence within the interview data of a differentiated use of available sources of online information. Firstly, all interviewees with a basic or secondary level of education described how they posted on online peer support sites as their primary source of information when seeking advice, while parents with a higher level of education reported how they would seek information from other sources first. However, this was somewhat speculative given that these discussions were not part of every interview. This would, however, make an interesting topic for further research. Secondly, parents’ use of online support and information could be bounded by their understanding of jargon, particularly within summaries of scientific research. However, more educated parents reported fewer problems with jargon and used strategies to deal with any terms with which they were unfamiliar. A limitation of this finding was that while all parents were asked about jargon on sites and groups, it was not clear whether all had tried to access scientific papers or not, making comparisons difficult. Interestingly, one parent who had difficulties understanding primary research papers reported that other parents would post digested summaries of this information online. This parent held a higher education qualification, suggesting that a very specific form of cultural capital may be needed to interpret medical research. This was at odds with Bourdieu’s (1986) conceptualisation of social capital offline, representing a kind of bridging capital rather than an (unintentional) exclusion of people possessing fewer relevant capitals or goods. However, as noted in section 8.2, there was also evidence of a parent from a higher economic capital bracket withholding useful goods from some online peer support settings, preferring to post them in a blog setting instead, where they may be more likely to be accessed by more privileged parents. As noted above, these conclusions were somewhat speculative and further research is needed to explore these findings in a more systematic way. For example, a survey could explore the use of different kinds of information accessed by education, comparing the use of different sources accessed online including research papers and popular online peer support sites.
8.3.3 Indications of the role of habitus in online support site use As argued in Chapter 3, I reject criticisms of Bourdieu’s concept of habitus as socially deterministic. My data supported this interpretation, which I argue below reflects Bourdieu’s (1998) conceptualisation of agency constrained within wider structural differentiation, but with the ability to challenge the ‘rules of the game’ within fields and to accrue relevant capitals and goods to gain symbolic capital, as explored in section 8.4. There were a number of practices, tastes and dispositions described in the following subsections that were used as markers of whether online support sites were a good ‘fit’ with an individual’s own dispositions. These were understood within this research to reflect Bourdieu’s concept of habitus as a way of distinguishing between other people in different social positions (Bourdieu, 1998), particularly as interviewees claimed that it was hard to assess someone’s social background online, even on Facebook. Some parents discussed how they would befriend some parents of people with Rett syndrome with whom they had an ‘affinity’. As noted in Chapter 6, these aspects of interviewees could be difficult, with parents concerned they appeared snobbish, and quick to point out that they did have friendships with people from different social backgrounds. As noted in Chapter 6 and above, it could be difficult for interviewees to assess traditional markers of background online, so instead parents talked about having more in common with some people than with others. Following Bourdieu (1984), interview data was explored in terms of how parents discussed distinguishing tastes and practices and five key areas emerged. These were parenting practices, digital taste, emotional expression and illness narratives (discussed in Chapter 6) and attitudes towards peer versus professional opinions (discussed in Chapter 7).
Parenting practices Interviewees noted that there could be disagreements, particularly on Facebook groups, about parenting practices. These related to a number of parenting choices, such as decisions about medication, whether or not to have respite care for your child, decisions about whether to take a child to hospital, whether or not to go ahead with a second pregnancy with a foetus diagnosed as having Rett syndrome, dietary changes and the use of supplements. These could lead to ‘vigorous’ disagreements. As noted above, it was rare for the two interviewees who wrote blogs to experience criticism of their blog posts. Although suggestive, this is an interesting difference, suggesting that blogs – perhaps through the greater symbolic capital held by a blogger - are ‘safer’ places for parents to discuss their parenting choices, sometimes even to present counter-narratives as discussed in Chapter 6. It may also suggest a shared habitus, demonstrated by shared tastes in parenting practices. Given the social differentiation of the use of blogs, this is an area where further research might explore whether blogs are places where homogenous groups of parents with shared habitus might meet. Both blog writers expressed their preference for interacting with other parents through their blogs rather than on Facebook, with one parent having never used Facebook and the other having chosen to withdraw from Facebook groups after active participation. Digital taste A key differentiating factor that emerged in coding for differences in practices and tastes was a preference for either more information-based or more emotionally-based interactions online. The first kind was more likely to be encountered on older mediums of peer support, such as email groups, and could be seen to reflect the pre-participatory web style of interaction. By contrast, the second kind tended to be found on more ‘participatory web’ style social media sharing sites, like Facebook. A key area of habitus fit or misfit was between the propensity to communicate in one way and the kind of interactions that tended to happen on different kinds of sites. Older interviewees tended to prefer information-based communications, but some younger parents also expressed this preference. As argued in Chapter 6, this also appeared to be related to wider habitus differences around emotional expression and the fit between illness narratives and biographical disruption, discussed next. This fits within Bourdieu’s (1998) argument that habitus is not socially determined, but may partly reflect wider structural differences or inequalities. It also fits with the move away from socially deterministic narratives of the Internet into discussions of ‘types’ of users that may share some demographic characteristics (e.g. ‘cultures of the Internet’: Dutton & Blank, 2013).
Emotional expression Perhaps due to the range of sites used by this group – where none allowed anonymity – parents did not make distinctions between privately and publically accessible sites when talking about posting about their emotions. Parents’ approaches to sharing their emotions online varied along a continuum, with parents who would never share anything personal or emotional online, even on a private site, to those who were very open on any site. This was partly related to the strength of ties online, where weak, colleague-like ties inhibited emotional expression and stronger ties allowed greater disclosure. However for some parents, the choice about whether or not to share whether one was coping or not was related to broader emotional habitus, learned through socialisation. It was also linked to concerns about the kind of illness narrative presented (see below), where such posting could be seen as ‘negative’, and like a chaos narrative (see below). Propensity to share ones emotions had some relationship to age, where no interviewee in their 50s described themselves as willing to ‘expose’ themselves online at all.
Illness narratives A key point of contention for some interviewees in visiting online support groups was a misfit between their own views and the illness narratives produced in that space. Some interviewees discussed the presence of online narratives that appeared to reflect Frank's (1995) definition of ‘chaos narratives’, in that they represented unresolved stories and issues. The most extreme version of a chaos narrative described by interviewees was one in direct conflict with the narratives around the possibility of a cure for Rett syndrome. This was considered by some interviewees as too damaging for the group and a number of sanctions were reported as having been applied by different members to discourage posting of this nature. More common forms of chaos narrative involved ‘ranting’ or ‘venting’, where parents shared frustrating experiences, or their fears and anxieties about their child or their child’s symptoms – but without solutions, like an incomplete story. Parents who had reached a point of repair with biographical disruption, who tended to have older children, did not have a good habitus fit with these kinds of narratives, which they described as ‘negative’. One reaction to these kinds of posts was for interviewees to co-create more positive narratives to ‘counterbalance’ chaotic narratives. Sometimes this was offering some relevant advice to solve a problem, but at other times this involved the posting of alternative perspectives on children with Rett syndrome, challenging a deficit model of disability and illness and focusing instead on their child as a child first, or sharing positive experiences their child had enjoyed. This reflects recent research suggesting that online forums could be places where positive narratives of closure were co-created (Orgad, 2005), or where parents could share the achievements of their disabled children (Jones and Lewis, 2001). Peer versus professional expertise Parents of adult children did not discuss having gained medical advice from online peer support sites. This may partly reflect a lower need for medical information, as outlined in Chapter 6. However, given that parents were asked about their use of online peer support across their caring career, this may be due to differences in disposition related to the relative status of peer and professional opinions. This was an aspect that arose in some interview accounts, where parents argued that medical expertise should be trusted over the ‘opinions’ of parents. This was something that emerged in interviews and was not specifically explored for all parents, but could benefit from further research. As with some other aspects of habitus this was a popular view among older interviewees (expressed by three out of the five parents in their 50s) but was not restricted to this age group. Nonetheless, no parent in their 50s endorsed the view expressed by some interviewees that peer expertise had an equal or greater value than medical expertise. However, given the earlier findings showing how older parents had often found a network of trusted professionals, this may instead reflect changing experiences of medical support over time and greater opportunities to have found suitable expert, medical support. I aimed to answer the exploratory question of how an individual’s habitus and possession of different forms of relevant cultural and social capital affects their use of caring-related online support and information. In terms of the impact of alternative social capital resources, this research was illuminating in that it highlighted how parents’ use of different sources of support becomes more differentiated over time, while being weighed up alongside alternatives that are available both online and offline. This was an important finding because it places the use of online support and information within the realm of everyday practices, adding to the limited research that explores the use of online support contexts within a wider set of practices (e.g. see Baym, 2009), and how sources of online and offline support mesh and can be complementary (Lowe et al., 2009). The evidence relating to cultural capital was suggestive, mostly because it emerged from accounts rather than being explored in all interviews. Nonetheless, there were some intriguing findings that bear further exploration in future research. These hinted at the differential use of primary sources of information, particularly research papers and blogs, as well as a tendency to research across a number of sources rather than to ask peers for advice as a primary information-seeking strategy. However, there was also evidence of parents gaining summaries of this research from other parents in online support settings, suggesting a form of bridging capital. Together these findings hint at a differentiated use of information in seeking understanding about rare genetic syndromes, which requires further research, for instance a survey exploring use of research papers in online searching rather than non-specific ‘information searching’ or use of ‘lay health’ sites. The evidence of how tastes, dispositions and practices influenced the use of online support sites was significant because it provided evidence that moved beyond social determinism and suggested how parents may identify other ‘like’ parents with whom to create closer bonds. It was also useful to identify that illness narratives online may influence parents’ engagement with certain online spaces. There were some interesting intimations that digital taste, illness narratives, emotional expression online and attitudes toward medical advice may partly be connected to differentiation among generations. These are areas worthy of further exploration in that they provide ways to extend current conceptualisations of the differential use of the Internet (as in Dutton and Blank’s ‘cultures of the Internet’, 2013) as a way of exploring generational differences in use, but without being socially deterministic. However, without more evidence of the prevalence of these attitudes among certain age groups (ideally through quantitative data), the ambiguity around the connection with age is difficult to resolve. Nonetheless, these findings highlight the importance of understanding how the use of the Internet relates not only to issues of technical ability but also to preferences in wider information seeking and caring practices. This supports Kivits’s (2009) argument that the use of the Internet in health should take into account everyday media, health and information seeking practices.
8.4 The social differentiation of benefits from online support sites How does the use of online peer support sites influence wider caring practices? Is there any evidence of differentiation of benefits by age, income or education?
Chapters 5 and 7 presented quantitative and qualitative data about the differentiation of benefits accrued from online support sites. These findings are discussed below in terms of social capital benefits, knowledge and expertise ‘goods’, economic capital and symbolic capital in wider caring fields.
8.4.1 Social capital benefits Chapter 5 presented the rated importance of generic online support and the benefits of online peer support, which were based on measures reflecting Ferlander’s (2007) categories of emotional support, informational support and instrumental support. Online generic support was rated as important by 63.2 per cent of survey respondents who had ever used it. A significantly higher proportion of younger parents, parents of younger children and parents of children diagnosed in the last seven years rated it as important when compared to their peers. Its importance was also related to a greater number of years using the Internet and having mobile access. This result appears to be in line with other findings related to age reported in this thesis that suggest that older parents benefitted less from online information, having already established a certain level of expertise and trusted social capital sources upon which to rely for advice and information when it is needed. Eighty-four per cent of parents agreed that reading others’ experiences made them feel less alone (emotional support). In interviews, parents described how they felt less isolated knowing that other parents experienced some of the same difficulties and emotional reactions. This was most strongly differentiated by time since diagnosis, but not in a linear way, although the smallest proportion of agreement was among parents whose child had been diagnosed more than 25 years ago. Interviewees’ accounts showed that parents of children who had been diagnosed less recently were still able to gain emotional support benefits, either when reading accounts written by parents of adult children or as a way of reinterpreting their own early reactions to their child’s diagnosis. Interestingly, parents with a higher education qualification were more likely to report experiencing this kind of emotional support. Interview data did not provide any further clues as to why this may be, but this is an interesting area worthy of further research. A similar question explored agreement with having someone to talk to online if one felt alone. This was asked of respondents who had communicated with at least one carer exclusively online. This was only significantly differentiated by age of child, with a linear relationship where the younger the child, the higher the proportion agreeing with this statement. This may partly reflect a lower level of alternative social capital resources used by younger parents, as found among the interviewees. A comparison across occupational group could not be carried out on this aspect of online social capital benefit. Rarely, parents described feeling a sense of companionship online, with some conversations that were not direct requests for information and more chatty. However, most of the time, interviewees reported that forums were used to provide caring-specific advice, information and support. These findings partly reflected wider literature, in that younger parents were more likely to report benefits related to online peer support, although differences by occupation (after Leonard et al., 2004) either could not be carried out or were not significant.
8.4.2 Knowledge and expertise ‘goods’ In interview accounts, which covered use of online peer support across a caring career, parents reported certain benefits across age, education and income groups. This reflected benefits summarised in the literature cited in Chapter 2, such as understanding the meaning of the diagnosis and prognosis and gaining information to understand and interpret new behaviours and symptoms. This reflected the use of online support sites as sources of ‘case histories’ to understand prognosis that was described by Schaffer and colleagues (2007) and Skinner & Schaffer (2006). Parents of adult children did not report having used online peer support for day-to-day caring advice and information about special educational needs and medical information. This may reflect both the level of already-accrued expertise with regard to caring practices, their children’s age stage and the lower level of novel health problems experienced by the children of these interviewees. More educated and wealthier interviewees discussed seeking different forms of knowledge from online peer support groups, including information about the daily management of health issues and advice about aspects of special educational provision. However, as noted in Chapter 7, these benefits were those reported by parents within interviews, and it was possible that in retrospective accounts, some topics were less memorable to parents of older children than others.
8.4.3 Economic capital Similarly, it was difficult to assess differences in economic capital gains as these were not explicitly covered within interviews, but emerged in some interview accounts in response to questions about receiving practical help or help to solve a problem. A range of parents across different social groupings reported having gained information that had or could potentially be converted into economic capital gains. As described in Chapter 7, there was some suggestion that younger, wealthier and more educated parents had gained the largest actual ‘lump sum’ benefits, for example, having an extension to their house funded. However it was not possible to ascertain whether some parents had never gained such information online or whether they already gained this information from an alternative source. This is an area where further research that explicitly explores the benefits gained by carers across a range of support sources, both online and offline, would shed further light on this speculative finding.
8.4.4 Symbolic capital in wider fields Even parents with high levels of relevant cultural capital (for instance, a Psychology-related Masters) reported a sense of feeling powerless in initial medical encounters. An important aspect of online support was therefore the possibility of ‘borrowing’ cultural capital from more experienced parents to argue for additional support, or to decide when to challenge a local decision about services. This was similar to what McKeever & Miller (2004) described as borrowing symbolic capital in caring fields, only instead of borrowing capital from a professional when dealing with another professional, interviewees described how online peer support allowed them to borrow the expertise of more experienced parents, or parents who had managed to challenge a local decision, or were allowed access to a service in another area. This borrowed capital could be used to support parents’ ‘gut instincts’ in making medical decisions or in daily management of health problems or could even include access to professional reports that had been used to argue for funding for specialist equipment. However, as described in section 8.3.3, not all parents were prepared to challenge medical advice, which arguably related to wider differences in habitus regarding judgements of the relative importance of peer and professional advice, or having access to trusted medical expertise. In terms of actual benefits reported, these included gaining additional support on a statement, challenging a decision to limit services or gaining a piece of equipment. There was no evidence that wealthier or more educated parents had disproportionately benefitted from this kind of information, but no parents of adult children reported gaining such benefits. Again this is likely to reflect the different needs, greater expertise and lower incidence of novel issues faced by parents of adult children and perhaps limitations to the recall of past events in a retrospective account.
8.5 Key contributions to our understanding of the role of online support and information in modern health and caring practices
As discussed above, I aimed to provide a more coherent account of the role of online peer support within the wider caring practices of parents of people with a rare syndrome. In doing so, I hoped to deal with what I argue is the currently fragmented nature of our understanding of this field. Overall I believe that this research has provided a valuable contribution to the field and succeeded in developing a deeper understanding of the links between structure and agency-based accounts of the use of online peer support among carers. In this final section I bring this thesis to a close by highlighting what I believe to be the main contributions to existing research.
8.5.1 Meshed practices: the importance of understanding the use of online peer support in context I began this thesis by arguing that current research was methodologically and theoretically fragmented. My research proposed to provide a more coherent account by using Bourdieu’s concepts of capitals, fields and habitus within a mixed methodological approach. My aim was to understand the use of online peer support groups and sites as they exist within an embedded social context, taking into account the ‘meshing’ of online and offline sources of support, the e- scaped nature of health and the social differentiation of Internet use. By researching the use of such sites from the perspective of potential and actual users within a single case study group, this research has explored how the social differentiation of different forms of online peer support within this group relates to everyday information-seeking, online and caring practices, without being socially deterministic. The main benefit of using this method has been the ability to bring together macro social differentiation data and micro data about everyday practices in order to explore both the wider context and detail of how online support interactions occur within a wider, and socially structured social context. This has paid dividends in demonstrating how the use of online support is used in a dynamic way over a carer’s career for the building of expertise and valued social capital, depending upon a potential user’s existing alternative resources, stockpiles of relevant expertise, cultural capital, habitus, child’s health and state of biographical disruption and preferred illness narrative.
8.5.2 Questioning digital inequality: the role of expertise and alternative sources of support A key contribution to the literature was the ability to interrogate the apparent digital inequality experienced by older parents of people with rare syndromes. As discussed in Chapter 2, there have been debates about whether social differentiation in the use of the Internet should be understood as digital inequality or the result of digital choice. This research presented a third way by demonstrating how online support and information was used as one tool among many and should be understood within the context of existing expertise, sources of support and information needs. Although my interviewees did not include parents aged over 60, the parents aged in their 50s demonstrated how they were able to use the Internet alongside other sources of support and information to carry out ‘expert carer’ work. Through their interview accounts they demonstrated that, rather than being intimidated by or unfamiliar with online sources of support, they did not value the goods available, having acquired more expertise and often having little in common with the younger parents who appeared to be more active in such online spaces.
8.5.3 The reproduction of symbolic power online There were some interesting suggestions in the data that the interests of influential institutions and more socially privileged people were privileged and reproduced online, both through the unequal symbolic power conferred by the structure of some online platforms and the kinds of conflicts that were reproduced in some online support settings. Similarly, the use of blogs suggested a possible online space where privileged groups could ‘fortuitously’ find similar others, where parenting and other practices were rarely criticised and expertise could be traded in an ostensibly public, but actually differentiated social space. These are also areas worthy of further research.
8.5.3 Troubling the concept of lay health support sites As described in Chapter 7, I had approached this research with an expectation of finding online lay support sites that would be distinct from sites where institutional interests would be represented. This was in part due to the emphasis on lay health information within the literature and the anxieties about the credibility of such information when presented alongside other forms of information. Yet through interviews it became clear that forums that were set up for and by parents were used for wider purposes than for sharing lay health information and emotional support. They were also used as a means to exchange different kinds of information, to link to outside sites related to research and for parents’ own summaries of current research. This perhaps reflects the particular tasks that the ‘expert carer’ of someone with a rare genetic syndrome might engage in, as reflected in Skinner and Schaffer’s (2006) account of parents in online advocacy networks presenting research that was used to fight for experimental treatments. It may also reflect the broader use and connectivity of social networking sites and their use by parents to connect to wider networks of interested parties, such as researchers, clinicians and charities, and vice versa. This suggests that traditional concepts such as lay versus other forms of research need rethinking when discussing (particularly more educated) parents and patients who can and do develop specialist, expert forms of knowledge that combine both lay understanding and skills in synthesising research.
8.5.4 It’s about time: the importance of understanding practices within a wider socio-historical context As argued above, this research presented the role of online peer support among a case study group of parents of people with a rare syndrome, who had experienced their caring careers during a time of great social and technological change. It is worth noting that these parents were already engaged with various sources of support, both online and offline, so may have been more proactive in seeking information than parents not represented in this research. Nonetheless, this research still provided a coherent exploration of the role of the Internet within the wider social practices of these parents. Statistically it was not possible to differentiate between the impact of parents’ age, their child’s age and the time since their child’s diagnosis in understanding differences in use of the Internet for caring-related purposes. Even with a larger sample (which is not possible within a small group of parents of people with a rare syndrome, unless an extremely comprehensive database exists), issues of multicollinearity would prevent teasing out the relative impact of these variables, which all relate to time. However, by combining qualitative with quantitative data it was possible to explore how these intersecting aspects of parents’ lives influenced their use of online support, and a much richer picture emerged, as described above. It is possible – and likely – that as the Internet becomes increasingly embedded in everyday life, and the younger group of parents in this study ages, that use of the Internet for support and information by parents of people with rare syndromes will become commonplace. This research therefore follows Bourdieu (1993) in arguing that it is important, when exploring practices, to understand them within the social and historical context in which they occur. This thesis has shed light on how carers’ use of the Internet reflects their socio-historical position, wider social practices and the cultural and social capital resources available to them. However, it has not downplayed parents’ active agency within these constraints to gain expertise, support and other goods that have the potential to benefit their children. I therefore believe that this research has succeeded in bringing together macro and micro data to develop a greater understanding of the contingent use of online support and information in the wider caring practices of parents of people with a rare syndrome. Bibliography
Baum, L. S. (2004). Internet parent support groups for primary caregivers of a child with special health care needs. Pediatric Nursing, 30, 381–388, 401. Baym, N. K. (2009). A Call for Grounding in the Face of Blurred Boundaries. Journal of Computer-Mediated Communication, 14(3), 720–723. doi:10.1111/j.1083-6101.2009.01461.x Beck, U. (1992). Risk Society: Towards a New Modernity. London: Sage. Blackburn, C., & Read, J. (2005). Using the Internet? The experiences of parents of disabled children. Child: Care, Health and Development, 31(5), 507–515. Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1365- 2214.2005.00541.x/full Blackburn, C., Read, J., & Hughes, N. (2005). Carers and the digital divide: factors affecting Internet use among carers in the UK. Health & Social Care in the Community, 13(3), 201–210. Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1365- 2524.2005.00547.x/full Bourdieu, P. (1973). Cultural Reproduction and Social Reproduction. In R. K. Brown (Ed.), Knowledge, Education, and Cultural Change: Papers in the Sociology of Education (pp. 71–112). London: Tavistock. Bourdieu, P. (1977). Outline of a Theory of Practice. Cambridge: Cambridge University Press. Bourdieu, P. (1978). Sport and social class. Social Science Information, 17(6), 819–40. Bourdieu, P. (1984). Distinction: A Social Critique of the Judgement of Taste. Padstow: T.J. Press. Bourdieu, P. (1986). The Forms of Capital. In J. Richardson (Ed.), Handbook of Theory and Research for the Sociology of Education. Bourdieu, P. (1990). The Logic of Practice. Cambridge: Polity Press. Bourdieu, P. (1991). Language and Symbolic Power. Cambridge: Polity Press. Bourdieu, P. (1993). The Field of Cultural Production. Cambridge: Polity Press. Bourdieu, P. (1995). Social space and symbolic power. In D. McQuarie (Ed.), Readings in contemporary sociological theory: from modernity to post- modernity (pp. 323–34). Englewood Cliffs, N.J.: Prentice-Hall, Inc. Bourdieu, P. (1998). Practical Reason. Cambridge: Polity Press. Bourdieu, P. (2002). The Social Structures of the Economy. New York: Polity. Bourdieu, P., & Passeron, J. C. (1977). Reproduction in Education, Society, and Culture. Beverly Hills, CA: Sage. Bourdieu, P., & Wacquant, L. J. D. (1992). Towards a Reflexive Sociology: a Workshop with Pierre Bourdieu. Cambridge: Polity Press. Brock, A., Kvasny, L., & Hales, K. (2010). Cultural Appropriations of Technical Capital. Information, Communication & Society, 13(7), 1040–1059. doi:10.1080/1369118X.2010.498897 Bryman, A. (2008). Social Research Methods. Oxford: Oxford University Press. Bury, M. (1997). Health and illness in a changing society. London: Routledge. Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357. Retrieved from http://www.sciencedirect.com/science/article/pii/S003329090760074 4 Coleman, J. (1990). Foundations of Social Theory. Cambridge, MA: Belknap Press. Coleman, J. S. (1988). Social Capital in the Creation of Human Capital. American Journal of Sociology, 94, S95–S120. doi:10.1086/228943 Coleman, J. S. (1994). Foundations of Social Theory. London: Belknap Press. Cunningham, C. (1996). Families of children with Down syndrome. Down Syndrome Research and Practice, 4, 87–95. Cure Rett. (n.d.). We are working to reverse the symptoms of and cure Rett Syndrome. Retrieved from http://www.curerett.org.uk/about-us/ Davidson, J. (2008). Autistic culture online: Virtual communication and cultural expression on the spectrum. Social & Cultural Geography, 9(7), 791–806. Retrieved from http://www.tandfonline.com/doi/abs/10.1080/14649360802382586 Dillman, D. A., Christian, L. M., & Smyth, J. D. (2009). Internet, mail, and mixed- mode surveys: the tailored design method (3rd ed.). Hoboken, N.J.: Wiley. DiMaggio, P., Hargittai, E., Celeste, C., & Shafer, S. (2004). Social Inequality. In K. Neckerman (Ed.), Social Inequality (pp. 355–400). New York: Russell Sage Foundation. Retrieved from http://www.eszter.com/research/c05- digitalinequality.html Durieux, D. (2003). ICT and social inclusion in the everyday life of less abled people. Liege, Belgium: LENTIC, University of Liege. Dutton, W. ., & Blank, G. (2013). Cultures of the Internet : The Internet in Britain. Oxford Internet Survey 2013. Eysenbach, G. (2008). Medicine 2.0: social networking, collaboration, participation, apomediation, and openness. Journal of Medical Internet Research, 10(3), e22. doi:10.2196/jmir.1030 Ferlander, S. (2007). The importance of different forms of social capital for health. Acta Sociologica, 50(2), 115–128. Retrieved from http://asj.sagepub.com/content/50/2/115.short Field, A. (2009). Discovering statistics using SPSS. London: Sage. Field, J. (2008). Social Capital (2nd ed.). Abingdon: Routledge. Frank, A. W. (1995). The Wounded Storyteller: Body, Illness and Ethics (2nd Ed.). London: The University of Chicago Press. Frank, A. W. (2014). From Sick Role to Narrative Subject: The Sociological Career of Ill People and What’s Called “Experience.” Retrieved from http://vimeo.com/109902249 Fries, C. J. (2009). Bourdieu’s Reflexive Sociology as a Theoretical Basis for Mixed Methods Research: An Application to Complementary and Alternative Medicine. Journal of Mixed Methods Research, 3(4), 326–348. doi:10.1177/1558689809336660 Galston, W. A. (1999). (How) Does the Internet Affect Community? Some Speculations in Search of Evidence. In E. C. Kamarck & J. S. Nye (Eds.), democracy.com? Governance in a Networked World (pp. 45–61). Hollis, N.H.: Holllis Publishing. Giddens, A. (1991). Modernity and Self-Identity. Oxford: Polity. Giddens, A. (1993). New rules of sociological methods (2nd ed.). Cambridge: Polity Press. Gilbert, M. (2010). Theorizing Digital and Urban Inequalities. Information, Communication & Society, 13(7), 1000–1018. doi:10.1080/1369118X.2010.499954 Granovetter, M. S. (1973). The strength of weak ties. American Journal of Sociology, 78(6), 1360–1380. Retrieved from http://www.jstor.org/stable/10.2307/2776392 Groves, R. M., Fowler, F. J., Couper, M. P., Lepkowski, J. M., Singer, E., & Tourangeau, R. (2004). Survey Methodology. New Jersey: John Wiley & Sons. Gundersen, T. (2011). “One wants to know what a chromosome is”: the internet as a coping resource when adjusting to life parenting a child with a rare genetic disorder. Sociology of Health & Illness, 33(1), 81–95. Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1467- 9566.2010.01277.x/full Guy, J., Gan, J., Selfridge, J., Cobb, S., & Bird, A. (2007). Reversal of Neurological Defects in a Mouse Model of Rett Syndrome. Science, 315(5815), 1143– 1147. Hagberg, B. (2002). Clinical manifestations and stages of rett syndrome. Mental Retardation and Developmental Disabilities Research Reviews, 8(2), 61–65. doi:10.1002/mrdd.10020 Hagberg, B., Aicardi, J., Dias, K., Ramos, O. (1983). A progressive syndrome of autism, dementia, ataxia and loss of purposeful handuse in girls: Rett’s syndrome: Report of 35 cases. Annals of Neurology, 14, 471–479. Halbach, N. S. J., Smeets, E. E. J., van den Braak, N., van Roozendaal, K. E. P., Blok, R. M. J., Schrander-Stumpel, C. T. R. M., … Curfs, L. M. G. (2012). Genotype-phenotype relationships as prognosticators in Rett syndrome should be handled with care in clinical practice. American Journal of Medical Genetics Part A, 158A(2), 340–350. doi:10.1002/ajmg.a.34418 Hale, T. M. (2013). Is there such a thing as an online health lifestyle? Examining the relationship between social status, Internet access, and health behaviors. Information, Communication & Society, 16(4), 501–518. doi:10.1080/1369118X.2013.777759 Halford, S., & Carrigan, M. (2014). Susan Halford : “ Semantic web innovations are likely to have implications for us all .” LSE: The Impact Blog. Retrieved August 1, 2014, from http://blogs.lse.ac.uk/impactofsocialsciences/2014/07/18/the- philosophy-of-data-science-series-susan-halford/ Halford, S., & Savage, M. (2010). Reconceptualizing Digital Social Inequality. Information, Communication & Society, 13(7), 937–955. doi:10.1080/1369118X.2010.499956 Han, H. R., & Belcher, A. E. (2001). Computer-mediated support group use among parents of children with cancer--an exploratory study. Computers in Nursing, 19(1), 27–33. Hardey, M. (1999). Doctor in the house: the Internet as a source of lay health knowledge and the challenge of expertise. Sociology of Health and Illness, 21(6), 820–835. Hardey, M. (2001). “E-health”: the internet and the transformation of patients into consumers and producers of health knowledge. Information, Communication & Society, 4(3), 388–405. doi:10.1080/713768551 Hargittai, E. (2007). A Framework for Studying Differences in People’s Digital Media Uses. In N. Kutscher & H.-U. Otto (Eds.), Cyberworld Unlimited (pp. 121–137). Berlin: VS Verlag fuur Sozialwissenschaften/GWV Fachverlage GmbH. doi:10.1007/978-3-531-90519-8_7 Hargittai, E. (2008). The Digital Reproduction of Inequality. In D. Grusky (Ed.), Social Stratification (pp. 936–944). Boulder: Westview Press. Hargittai, E., & Hinnant, A. (2008). Digital Inequality: Differences in Young Adults’ Use of the Internet. Communication Research, 35(5), 602–621. doi:10.1177/0093650208321782 Harrits, G. S. (2011). More Than Method?: A Discussion of Paradigm Differences Within Mixed Methods Research. Journal of Mixed Methods Research, 5(2), 150–166. doi:10.1177/1558689811402506 Hawe, P., & Shiell, A. (2000). Social capital and health promotion: a review. Social Science & Medicine (1982), 51, 871–85. doi:10.1016/S0277- 9536(00)00067-8 Haythornthwaite, C., & Wellman, B. (2002). The Internet in Everyday Life: An Introduction. In B. Wellman & C. Haythornthwaite (Eds.), The Internet in everyday life (pp. 3–41). Oxford: Blackwell Publishing Ltd. Helsper, E. J. (2008). Digital inclusion: An analysis of social disadvantage and the information society. London: Department for Communities and Local Government. Retrieved from http://www.communities.gov.uk/documents/communities/pdf/digitali nclusionanalysis Helsper, E. J. (2012). A Corresponding Fields Model for the Links Between Social and Digital Exclusion. Communication Theory, 22(4), 403–426. doi:10.1111/j.1468-2885.2012.01416.x Henwood, F., Wyatt, S., Hart, A., & Smith, J. (2000). Turned on or turned off? Accessing health information on the Internet. Scandinavian Journal of Information Systems, 14(2), 79–90. Henwood, F., Wyatt, S., Hart, A., & Smith, J. (2003). “Ignorance is bliss sometimes”: Constraints on the emergence of the “informed patient” in the changing landscapes of health information. Sociology of Health and Illness, 25(6), 589–607. doi:10.1111/1467-9566.00360 Hine, C. (2015). Ethnography for the Internet: Embedded, Embodied and Everyday. London: Bloomsbury. Huws, J., Jones, R. S. P., & Ingledew, D. K. (2001). Parents of Children with Autism using an Email Group: A Grounded Theory Study. Journal of Health Psychology, 6(5), 569–584. doi:10.1177/135910530100600509 IRSF. (2008). History. www.rettsyndrome.org. Retrieved from http://web.archive.org/web/20111022104745/http://www.rettsyndro me.org/index.php?option=com_content&task=view&id=21&Itemid=816 Ishikawa, A., Goto, T., Narasaki, M., Yokochi, K., Kitahara, H., & Fukuyama, Y. (1978). A new syndrome of progressive psychomotor retardation with peculiar stereotyped movements and autistic tendency: a report of three cases. Brain Development, 3, 258. Johnsson, B. (2013). Life with Rett Syndrome: It is so much more than the facts, the stats and the science. The Independent Blogs. Retrieved from http://blogs.independent.co.uk/2013/03/25/life-with-rett-syndrome- it-is-so-much-more-than-the-facts-the-stats-and-the-science/ Jones, R. S., & Lewis, H. (2001). Debunking the pathological model--the functions of an Internet discussion group. Down’s Syndrome, Research and Practice : The Journal of the Sarah Duffen Centre / University of Portsmouth, 6(3), 123–127. doi:10.3104/reports.103 Julien, C. (2014). Bourdieu, Social Capital and Online Interaction. Sociology. doi:10.1177/0038038514535862 Kerr, A. M. (2002). Annotation: Rett syndrome: recent progress and implications for research and clinical practice. Journal of Child Psychology and Psychiatry, 43(3), 277–287. Kerr, A. M., Armstrong, D. D., Prescott, R. J., Doyle, D., & Kearney, D. L. (1997). Analysis of deaths in the British Rett Survey. European Child and Adolescent Psychiatry, 6, 71–4. Kivits, J. (2009). Everyday health and the internet: A mediated health perspective on health information seeking. Sociology of Health and Illness, 31(5), 673–687. doi:10.1111/j.1467-9566.2008.01153.x Kivits, J. (2013). E-Health and Renewed Sociological Approaches to Health and Illness. In K. Orton-Johnson & N. Prior (Eds.), Digital Sociology: Critical Perspectives (pp. 213–226). Basingstoke: Palgrave Macmillan. Koteyko, N., Hunt, D., & Gunter, B. (2015). Expectations in the field of the Internet and health: an analysis of claims about social networking sites in clinical literature. Sociology of Health & Illness. doi:10.1111/1467- 9566.12203 Lash, S. (2002). Critique of Information. London: Sage. Leonard, H., Slack-Smith, L., Phillips, T., Richardson, S., D’Orsogna, L., & Mulroy, S. (2004). How can the Internet help parents of children with rare neurologic disorders? Journal of Child Neurology, 19(11), 902–907. Retrieved from http://jcn.sagepub.com/content/19/11/902.short Lewis, T. (2006). DIY selves?: Reflexivity and habitus in young people’s use of the internet for health information. European Journal of Cultural Studies, 9(4), 461–479. doi:10.1177/1367549406069068 Lofland, J., Snow, D., Anderson, L., & Lofland, L. H. (2006). Analyzing social settings: a guide to qualitative observation and analysis. London: Wadsworth/Thompson Learning. Lotan, M., Merrick, J., Kandel, I., & Morad, M. (2010). Aging in Persons with Rett Syndrome: An Updated Review. The Scientific World Journal, 10, 778–787. doi:10.1100/tsw.2010.79 Lowe, P., Powell, J., Griffiths, F., Thorogood, M., & Locock, L. (2009). Making it all normal: the role of the internet in problematic pregnancy. Qualitative Health Research, 19, 1476–1484. doi:10.1177/1049732309348368 Mari, F., Caselli, R., Russo, S., Cogliati, F., Ariani, F., Longo, I., … Reniere, A. (2005). Germline mosaicism in Rett syndrome identified by prenatal diagnosis. Clinical Genetics, 67(Table 1), 258–260. doi:10.1111/j.1399- 0004.2005.00397.x Mason, J. (2002). Qualitative Researching (2nd ed.). London: Sage. McKeever, P., & Miller, K.-L. (2004). Mothering children who have disabilities: a Bourdieusian interpretation of maternal practices. Social Science & Medicine, 59(6), 1177–1191. doi:10.1016/j.socscimed.2003.12.023 Meyen, M., Pfaff-Rudiger, S., Dudenhoffer, K., & Huss, J. (2010). The internet in everyday life: a typology of internet users. Media, Culture & Society, 32(5), 873–882. doi:10.1177/0163443710374792 Muir Gray, J. A. (2002). The Resourceful Patient. Oxford: eRosetta Press. Nettleton, S. (2004). The Emergence of E-Scaped Medicine? Sociology, 38(4), 661–679. doi:10.1177/0038038504045857 Nettleton, S., Burrows, R., & O’Malley, L. (2005). The mundane realities of the everyday lay use of the internet for health, and their consequences for media convergence. Sociology of Health and Illness, 27(7), 972–992. doi:10.1111/j.1467-9566.2005.00466.x Nettleton, S., Burrows, R., O’Malley, L., & Watt, I. (2004). Health E-types? Information, Communication & Society, 7(4), 531–553. Retrieved from http://www.tandfonline.com/doi/abs/10.1080/136911804200030563 8 Neul, J. L., Kaufmann, W. E., Glaze, D. G., Christodoulou, J., Clarke, A. J., Bahi- Buisson, N., … for the RettSearch Consortium (Members listed in the Appendix). (2010). Rett syndrome: Revised diagnostic criteria and nomenclature. Annals of Neurology, 68(6), 944–950. doi:10.1002/ana.22124 Neurological Alliance. (2003). Neuro numbers: a brief review of the numbers of people in the UK with a neurological condition. London: Neurological Alliance. NHS. (2012). Rett syndrome - NHS Choices. Retrieved January 12, 2013, from http://www.nhs.uk/conditions/rett-syndrome/Pages/Introduction.aspx Nieckarz Jr, P. P. (2005). Community in cyber space?: The role of the Internet in facilitating and maintaining a community of live music collecting and trading. City & Community, 4(4), 403–423. Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1540- 6040.2005.00145.x/abstract North, S., Snyder, I., & Bulfin, S. (2008). Digital tastes: Social class and young people’s technology use. Information, Communication & Society, 11(7), 895–911. doi:10.1080/13691180802109006 Opdenakker, R. (2006). Advantages and disadvantages of four interview techniques in qualitative research. Forum: Qualitative Social Research, 7(4). Retrieved from http://www.qualitative- research.net/index.php/fqs/article/view/175/391 Orgad, S. (2005). Storytelling Online: Talking Breast Cancer on the Internet. New York: Peter Lang Publishing, Inc. Paterson, B. L., Brewer, J., & Stamler, L. L. (2013). Engagement of Parents in On-line Social Support Interventions. Journal of Pediatric Nursing, 28(2), 114–124. doi:10.1016/j.pedn.2012.05.001 Porter, A., & Edirippulige, S. (2007). Parents of Deaf Children Seeking Hearing Loss-Related Information on the Internet: the Australian Experience. Journal of Deaf Studies and Deaf Education, 12(4), 518–529. doi:10.1093/deafed/enm009 Putnam, R. D. (1993). Making Democracy Work: civic traditions in modern Italy. Princeton NJ: Princeton University Press. Putnam, R. D. (1995). Tuning In, Tuning Out: The Strange Disappearance of Social Capital in America. PS: Political Science and Politics, 28(4), 664–83. Putnam, R. D. (2000). Bowling Alone: the collapse and revival of American community. New York: Touchstone. Putnam, R. D. (2002, February). Bowling Together: The United State of America. The American Prospect, 20. Read, J., & Blackburn, C. (2005). Carers’ Perspectives on the Internet: Implications for Social and Health Care Service Provision. British Journal of Social Work. Rett UK. (n.d.). RettUK : Rett Syndrome - About Rett UK. Retrieved January 21, 2012, from http://www.rettuk.org/rettuk-public/rettuk/about- rettuk.html Rettie, R. (2008). Mobile Phones as Network Capital: Facilitating Connections. Mobilities, 3(2), 291–311. doi:10.1080/17450100802095346 Reverse Rett. (n.d.). Research. Retrieved April 3, 2013, from http://www.reverserett.org.uk/what-we-do/research/ Robinson, L. (2009). A Taste for the Necessary. Information, Communication & Society, 12(4), 488–507. doi:10.1080/13691180902857678 Robinson, L. (2011). Information-channel preferences and information- opportunity structures. Information, Communication & Society, 14(4), 472–494. doi:10.1080/1369118X.2011.562224 Rose, N. (2001). The politics of life itself. Theory, Culture and Society, 18, 1–30. Sapsford, R. (2007). Survey Research (2nd ed.). London: Sage. Saukko, P. (2009). Genetic risk online and offline: Two ways of being susceptible to blood clots. Health, Risk & Society, 11(1), 1–16. Retrieved from http://www.tandfonline.com/doi/abs/10.1080/13698570802538894 Schaffer, R., Kuczynski, K., & Skinner, D. (2007). Producing genetic knowledge and citizenship through the Internet: Mothers, pediatric genetics, and cybermedicine. Sociology of Health & Illness, 30(1), 145–159. Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1467- 9566.2007.01042.x/full Schradie, J. (2011). The digital production gap: The digital divide and Web 2.0 collide. Poetics, 39(2), 145–168. doi:10.1016/j.poetic.2011.02.003 Seale, C. (2005). New directions for critical internet health studies: Representing cancer experience on the web. Sociology of Health and Illness, 27(4), 515–540. doi:10.1111/j.1467-9566.2005.00454.x Skinner, D., & Schaffer, R. (2006). Families and Genetic Diagnoses in the Genomic and Internet Age. Infants & Young Children, 19(1), 16–24. doi:10.1097/00001163-200601000-00003 Smeets, E. E. J., Pelc, K., & Dan, B. (2011). Rett Syndrome. Molecular Syndromology, 2(3-5), 113–127. doi:10.1159/000337637 Smith, A. C., & Stewart, B. (2012). Body Perceptions and Health Behaviors in an Online Bodybuilding Community. Qualitative Health Research, 22(7), 971–985. Retrieved from http://qhr.sagepub.com/content/22/7/971.short Sterne, J. (2003). Bourdieu, Technique and Technology. Cultural Studies, 17(3- 4), 367–389. doi:10.1080/0950238032000083863 Sterne, J. (2005). Digital Media and Disciplinarity. The Information Society, 21(4), 249–256. doi:10.1080/01972240591007562 Tashakkori, A., & Teddlie, C. (1998). Mixed Methodology: combining qualitative and quantitative approaches. Thousand Oaks, CA: Sage. Tichenor, P., Donohue, G., & Olien, C. (1970). Mass Media Flow and Differential Growth of Knowledge. Public Opinion Quarterly, 34, 159–70. Valentine, G., & Skelton, T. (2008). Changing spaces: the role of the internet in shaping Deaf geographies. Social & Cultural Geography, 9(5), 469–485. Retrieved from http://www.tandfonline.com/doi/abs/10.1080/14649360802175691 Van Alstyne, M., & Brynjolfsson, E. (1996). Electronic Communities: Global Village or Cyberbalkanization? Retrieved from http://web.mit.edu/marshall/www/papers/CyberBalkans.pdf Van den Hooff, B., de Ridder, J., & Aukema, E. (2004). Exploring the Eagerness to Share Knowledge: The Role of Social Capital and ICT in Knowledge Sharing. In M. Huysman & V. Wulf (Eds.), Social Capital and Information Technology (pp. 163–186). Massachusetts: MIT Press. Van Deursen, A., & van Dijk, J. (2010). Internet skills and the digital divide. New Media & Society, 13, 893–911. doi:10.1177/1461444810386774 Wasko, M. M., & Faraj, S. (2005). Why should I share? Examining social capital and knowledge contribution in electronic networks of practice. Mis Quarterly, 9(1), 35–57. Retrieved from http://www.jstor.org/stable/10.2307/25148667 Webster, A. (2002). Innovative Health Technologies and the Social: Redefining Health, Medicine and the Body. Current Sociology, 50(3), 443– 57. Wellman, B., Boase, J., & Chen, W. (2002). The Networked Nature of Community: Online and Offline. IT & Society, 1(1), 151–165. Williams, D. C. (2006). On and Off the ’Net: Scales for Social Capital in an Online Era. Journal of Computer-Mediated Communication, 11(2), 593– 628. doi:10.1111/j.1083-6101.2006.00029.x Woolcock, M. (2001). The Place of Social Capital in Understanding Social and Economic Outcomes. Isuma: Canadian Journal of Policy Research, 2(1), 11–17. Retrieved from http://www.rwbsocialplanners.com.au/spt2006/Social Capital/Canadian Jnl of PR - S C - the place of soc.cap.pdf Wyatt, S., Henwood, F., Hart, A., Platzer, H. (2010). Transforming health? The Internet and everyday life: talking about health and illness. In P. Murdock, G., Golding (Ed.), Digital dynamics: engagments and disconnections (pp. 3–22). Cresskill, NJ: Hampton Press. Zaidman-Zait, A., & Jamieson, J. R. (2007). Providing web-based support for families of infants and young children with established disabilities. Infants & Young Children, 20(1), 11–25. Retrieved from http://journals.lww.com/iycjournal/Abstract/2007/01000/Providing_ Web_based_Support_for_Families_of.3.aspx Zhang, W. (2010). Technical Capital and Participatory Inequality in Edeliberation. Information, Communication & Society, 13(7), 1019–1039. doi:10.1080/1369118X.2010.495988 Zhao, S., & Elesh, D. (2007). The Second Digital Divide: Unequal Access to Social Capital in the Online World. International Review of Modern Sociology, 33(2), 171–192. Retrieved from http://www.allacademic.com/meta/p96480_index.html Ziebland, S. (2004). The importance of being expert: the quest for cancer information on the Internet. Social Science & Medicine, 59(9), 1783– 1793. Retrieved from http://www.sciencedirect.com/science/article/pii/S027795360400078 4 Ziebland, S., & Wyke, S. (2012). Health and Illness in a Connected World: How might sharing experienes on the Internet affect people’s health. The Millbank Quarterly, 90(2), 219–49. doi:10.1111/j.1468- 0009.2010.00608.x Zillien, N., & Hargittai, E. (2009). Digital Distinction: Status-Specific Types of Internet Usage. Social Science Quarterly, 90(2), 274–291. doi:10.1111/j.1540-6237.2009.00617.x Please see Volume II for Appendices.