Wake County Retiree Benefits Election Form Annual Open Enrollment 2015
This form is used to enroll in health plan coverage for the January 1, 2015 through December 31, 2015 Plan Year.
Name:
Social Security Number (last 4 digits only): Phone Number:
Email: ______** If your mailing address has changed, please note it below (otherwise, leave blank):
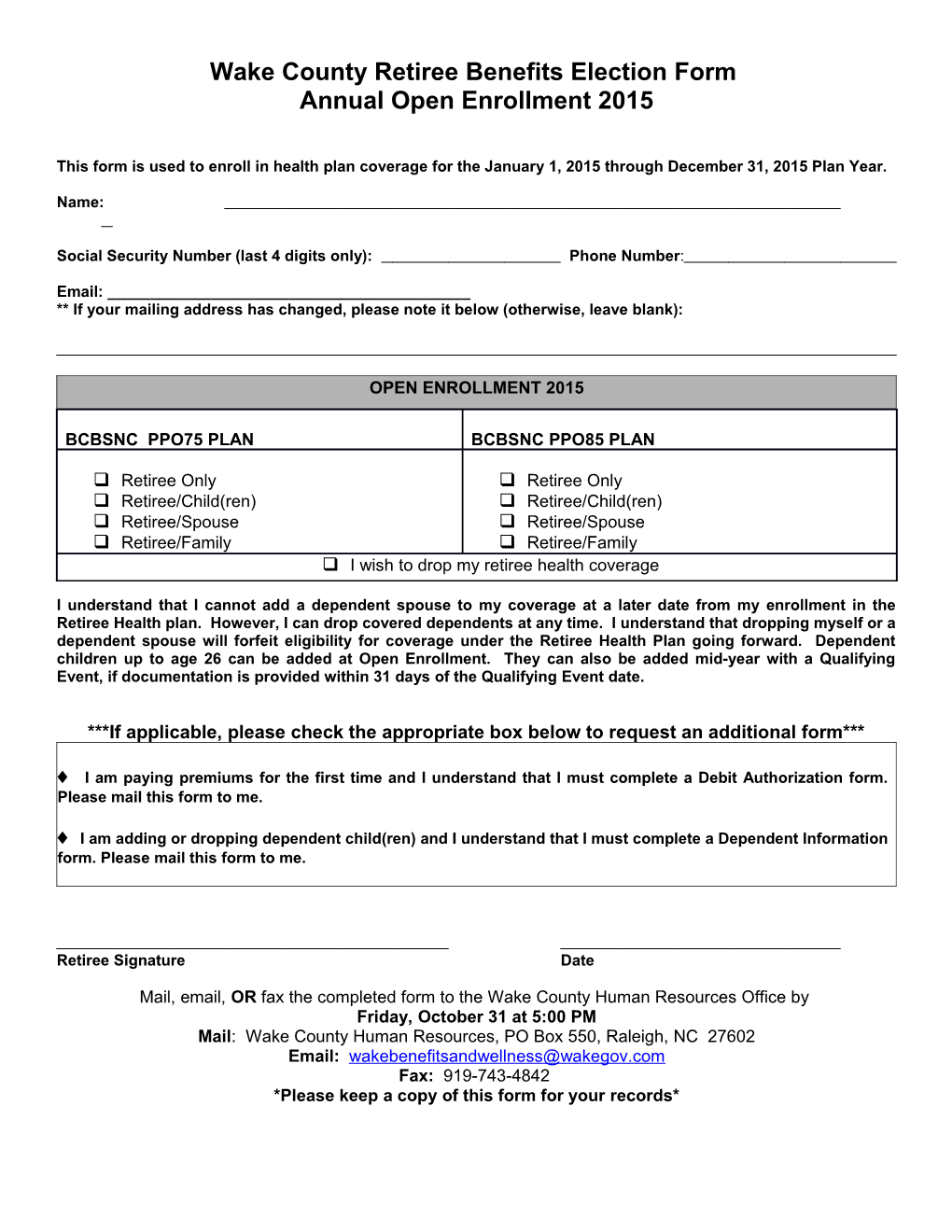
OPEN ENROLLMENT 2015
BCBSNC PPO75 PLAN BCBSNC PPO85 PLAN
Retiree Only Retiree Only Retiree/Child(ren) Retiree/Child(ren) Retiree/Spouse Retiree/Spouse Retiree/Family Retiree/Family I wish to drop my retiree health coverage
I understand that I cannot add a dependent spouse to my coverage at a later date from my enrollment in the Retiree Health plan. However, I can drop covered dependents at any time. I understand that dropping myself or a dependent spouse will forfeit eligibility for coverage under the Retiree Health Plan going forward. Dependent children up to age 26 can be added at Open Enrollment. They can also be added mid-year with a Qualifying Event, if documentation is provided within 31 days of the Qualifying Event date.
***If applicable, please check the appropriate box below to request an additional form***
I am paying premiums for the first time and I understand that I must complete a Debit Authorization form. Please mail this form to me.
I am adding or dropping dependent child(ren) and I understand that I must complete a Dependent Information form. Please mail this form to me.
Retiree Signature Date
Mail, email, OR fax the completed form to the Wake County Human Resources Office by Friday, October 31 at 5:00 PM Mail: Wake County Human Resources, PO Box 550, Raleigh, NC 27602 Email: [email protected] Fax: 919-743-4842 *Please keep a copy of this form for your records*