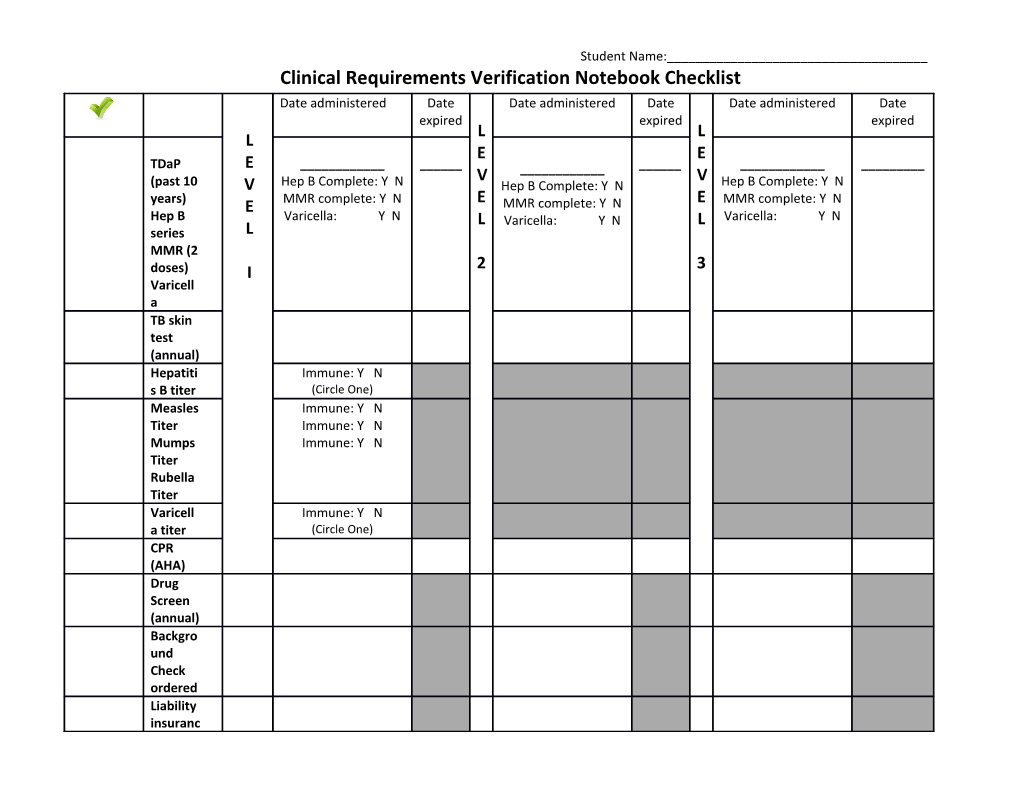
Student Name:______Clinical Requirements Verification Notebook Checklist Date administered Date Date administered Date Date administered Date expired expired expired L L L E E TDaP E ______V ______V (past 10 V Hep B Complete: Y N Hep B Complete: Y N Hep B Complete: Y N years) MMR complete: Y N E E MMR complete: Y N E MMR complete: Y N Hep B Varicella: Y N L Varicella: Y N L Varicella: Y N series L MMR (2 2 3 doses) I Varicell a TB skin test (annual) Hepatiti Immune: Y N s B titer (Circle One) Measles Immune: Y N Titer Immune: Y N Mumps Immune: Y N Titer Rubella Titer Varicell Immune: Y N a titer (Circle One) CPR (AHA) Drug Screen (annual) Backgro und Check ordered Liability insuranc Student Name:______e & Kaplan Fees Persona l Health Insuran ce Flu Vaccine Student Health Exam form CAPP Clinical Orientat ion/ (TCPS) (For instructor use): Confirmed by:
______fall ______fall ______fall ______spring ______spring ______spring