SUPPLEMENTARY FIGURES AND TABLES
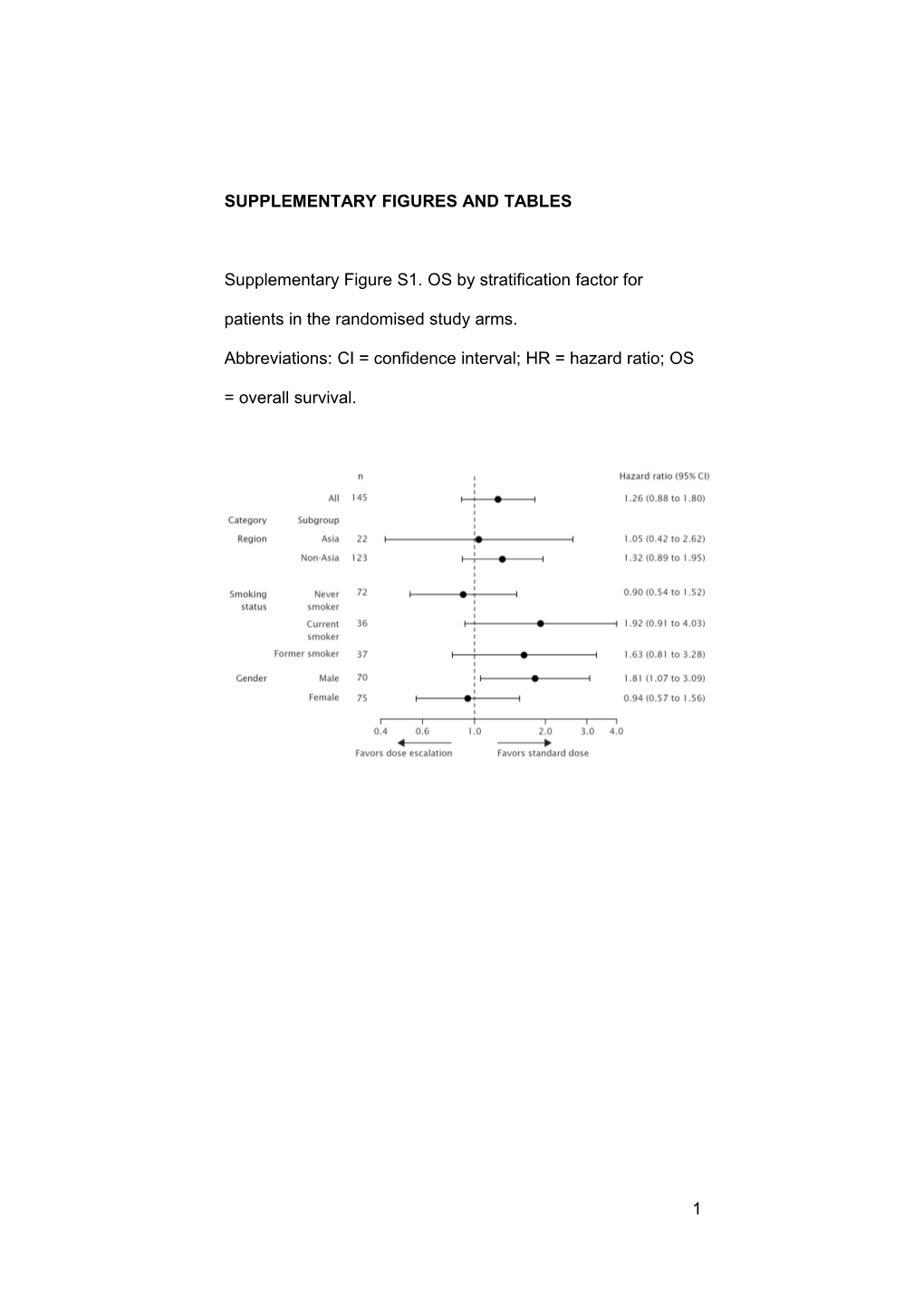
Supplementary Figure S1. OS by stratification factor for patients in the randomised study arms.
Abbreviations: CI = confidence interval; HR = hazard ratio; OS
= overall survival.
1 Supplementary Figure S2. Presence of biomarkers at initial diagnosis for the randomised study arms (patients in the standard-dose arm and patients in the dose-escalation arm) and OS stratified by biomarker status.
Abbreviations: CI = confidence interval; EGFR = epidermal growth factor receptor; FISH = fluorescence in-situ hybridization; HR = hazard ratio; IHC = immunohistochemistry;
OS = overall survival. aHR corresponding to the randomised standard-dose and dose-escalation arm.
2 3 Supplementary Table S1. Strategies for rash management in the RACHEL study
Erlotinib dose
Rash modification Treatment Grade 1 No erlotinib dose No intervention or treated with
modifications topical hydrocortisone (1% or
2.5% cream) or clindamycin (1%
gel) at the investigators’
discretion Grade 2 No erlotinib dose Hydrocortisone (2.5% cream), or
modifications clindamycin (1% gel), or
pimecrolimus (1% cream), with
the addition of either doxycycline
(100mg, po bid) or minocycline
(100mg, po bid) Grade 3 Erlotinib dose As for grade 2 rash, but with the
reductions until addition of methylprednisolone
grade ≤2 rash 4mg
achieved, at
which point the
dose could be re-
escalated Grade 4 Discontinue As for grade 3 rash
erlotinib Abbreviation: bid = twice daily; po = oral.
4 Supplementary Table S2. Incidence of grade ≥2 rash in the randomised population who had grade ≤1 rash after the 4-week run- in period
Standard dose Dose escalation
(n=75) (n=70) Patients with grade ≥2 7 (9.3) 29 (41.4) rash, n (%) 95% CI for grade ≥2 3.8–18.3 29.8–53.8 rash
Difference in rates 32.10
95% CI for difference in 18.0–46.2 rates
2 P value (χ test) <0.0001
Median time from randomisation to onset 71 (6–347) 28 (2–537) of grade ≥2 rash, days
(range) Abbreviation: CI = confidence interval.
5 Supplementary Table S3. Summary of exposure to erlotinib and
gemcitabine for the randomised arms Non-
Randomised randomised Dose
Standard dose escalationa Grade ≥2 rash (n=77) (n=71) (n=105) Total cumulative erlotinib dose (mg) Mean 17 025 26 823 13 749 SD 12 808 26 713 9067 SEM 1460 3170 885 Median 15 900 15 450 11 300 Range 2800–70 100 3200–152 350 1800–50 300 Total cumulative gemcitabine dose (mg) Mean 29 097 24 654 24 994 SD 19 335 16 279 15 519 SEM 2203 1932 1514 Median 25 200 18 700 21 600 Range 7000–10 5200 6583–83 220 5500–76 000 Abbreviations: SD = standard deviation; SEM = standard error of the
mean.
aIn the dose-escalation arm, 70 patients received 150mg/day,
49 patients then escalated to 200mg/day, 28 patients then escalated
to 250mg/day, and one patient was escalated to 300mg/day (in
error).
Supplementary Table S4. Reasons for withdrawal from trial treatment Non-
Randomised randomised Standard Dose Grade ≥2
dose escalation rash Reason for withdrawal, n
(%) (n=75) (n=71) (n=105)
6 Safety
Adverse event (including 4 (5.3) 7 (9.9) 8 (7.6)
intercurrent illness) Death 4 (5.3) 1 (1.4) 5 (4.8)
Non-safety
Insufficient therapeutic 57 (76) 52 (73.2) 84 (80)
response Violation of selection 0 (0) 1 (1.4) 0 (0)
criteria at entry Other protocol violation 0 (0) 0 (0) 1 (1.0)
Refused treatment 7 (9.3) 6 (8.5) 3 (2.9)
Other (including ‘did not 1 (1.3) 3 (4.2) 5 (4.8)
cooperate’ and ‘withdrew
consent’) Total 73 (97) 70 (99) 106 (100)
7 Supplementary Table S5. Dose reductions/interruptions Non-
Randomised randomised Dose reductions/ Standard Dose Grade ≥2 interruptions, n (%) dose escalation rash Erlotinib 14/77 (18) 31/71 (44) 33/105 (31) Gemcitabine 54/77 (70.1) 51/71 (71.8) 93/105 (88.6)
8