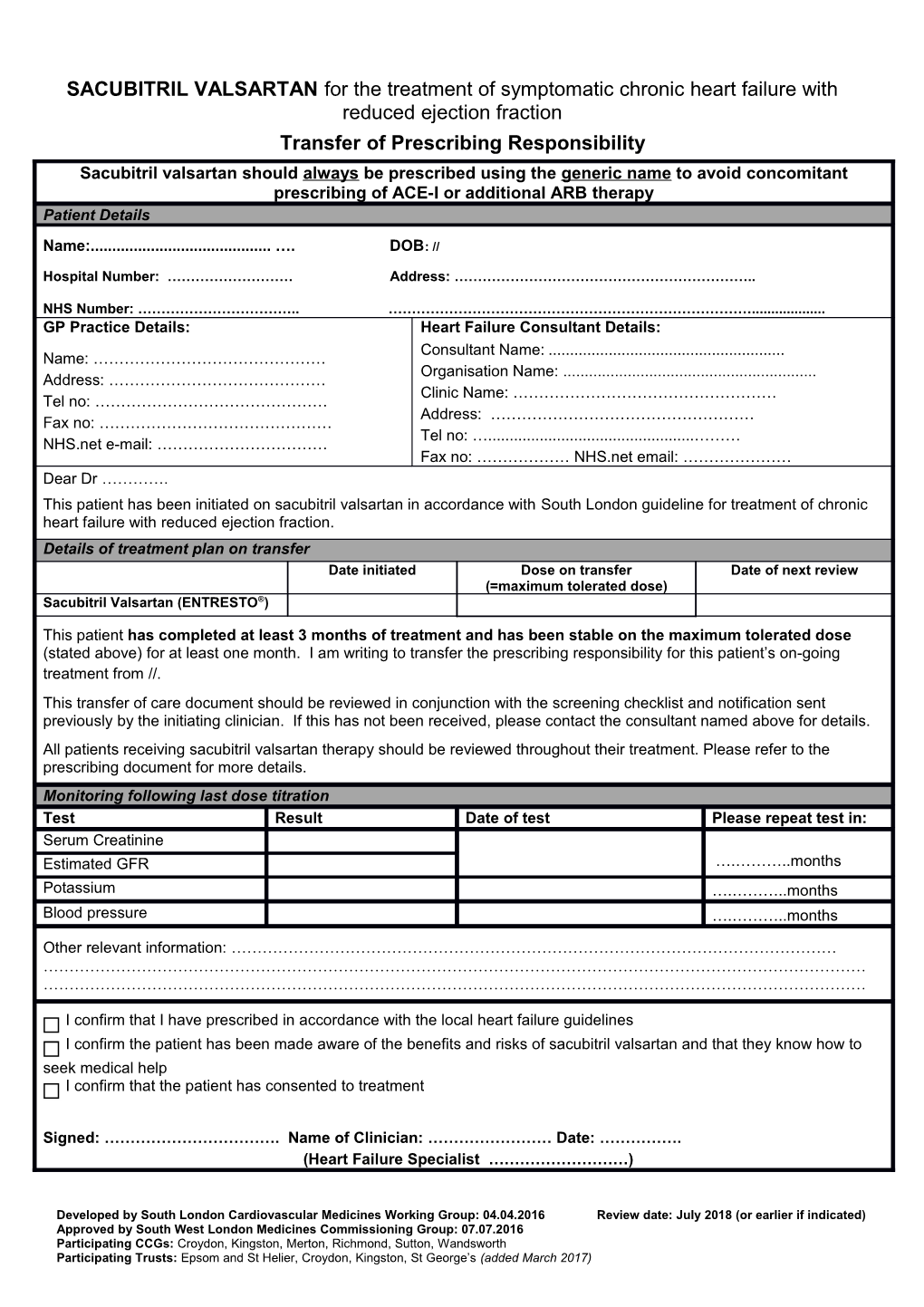
SACUBITRIL VALSARTAN for the treatment of symptomatic chronic heart failure with reduced ejection fraction Transfer of Prescribing Responsibility Sacubitril valsartan should always be prescribed using the generic name to avoid concomitant prescribing of ACE-I or additional ARB therapy Patient Details
Name:...... …. DOB: //
Hospital Number: ……………………… Address: ………………………………………………………..
NHS Number: …………………………….. ……………………………………………………………………...... GP Practice Details: Heart Failure Consultant Details: Consultant Name: ...... Name: ……………………………………… Organisation Name: ...... Address: …………………………………… Clinic Name: …………………………………………… Tel no: ……………………………………… Address: …………………………………………… Fax no: ……………………………………… Tel no: …...... ……… NHS.net e-mail: …………………………… Fax no: ……………… NHS.net email: ………………… Dear Dr …………. This patient has been initiated on sacubitril valsartan in accordance with South London guideline for treatment of chronic heart failure with reduced ejection fraction. Details of treatment plan on transfer Date initiated Dose on transfer Date of next review (=maximum tolerated dose) Sacubitril Valsartan (ENTRESTO®)
This patient has completed at least 3 months of treatment and has been stable on the maximum tolerated dose (stated above) for at least one month. I am writing to transfer the prescribing responsibility for this patient’s on-going treatment from //. This transfer of care document should be reviewed in conjunction with the screening checklist and notification sent previously by the initiating clinician. If this has not been received, please contact the consultant named above for details. All patients receiving sacubitril valsartan therapy should be reviewed throughout their treatment. Please refer to the prescribing document for more details. Monitoring following last dose titration Test Result Date of test Please repeat test in: Serum Creatinine Estimated GFR ….………..months Potassium ….………..months Blood pressure ….………..months
Other relevant information: ……………………………………………………………………………………………………… …………………………………………………………………………………………………………………………………………… ……………………………………………………………………………………………………………………………………………
I confirm that I have prescribed in accordance with the local heart failure guidelines I confirm the patient has been made aware of the benefits and risks of sacubitril valsartan and that they know how to seek medical help I confirm that the patient has consented to treatment
Signed: ……………………………. Name of Clinician: …………………… Date: ……………. (Heart Failure Specialist ………………………)
Developed by South London Cardiovascular Medicines Working Group: 04.04.2016 Review date: July 2018 (or earlier if indicated) Approved by South West London Medicines Commissioning Group: 07.07.2016 Participating CCGs: Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth Participating Trusts: Epsom and St Helier, Croydon, Kingston, St George’s (added March 2017) (In the event that there are any concerns regarding the acceptance of the prescribing responsibility for this medication please contact the initiating prescriber or heart failure team via )
Developed by South London Cardiovascular Medicines Working Group: 04.04.2016 Review date: July 2018 (or earlier if indicated) Approved by South West London Medicines Commissioning Group: 07.07.2016 Participating CCGs: Croydon, Kingston, Merton, Richmond, Sutton, Wandsworth Participating Trusts: Epsom and St Helier, Croydon, Kingston, St George’s (added March 2017)