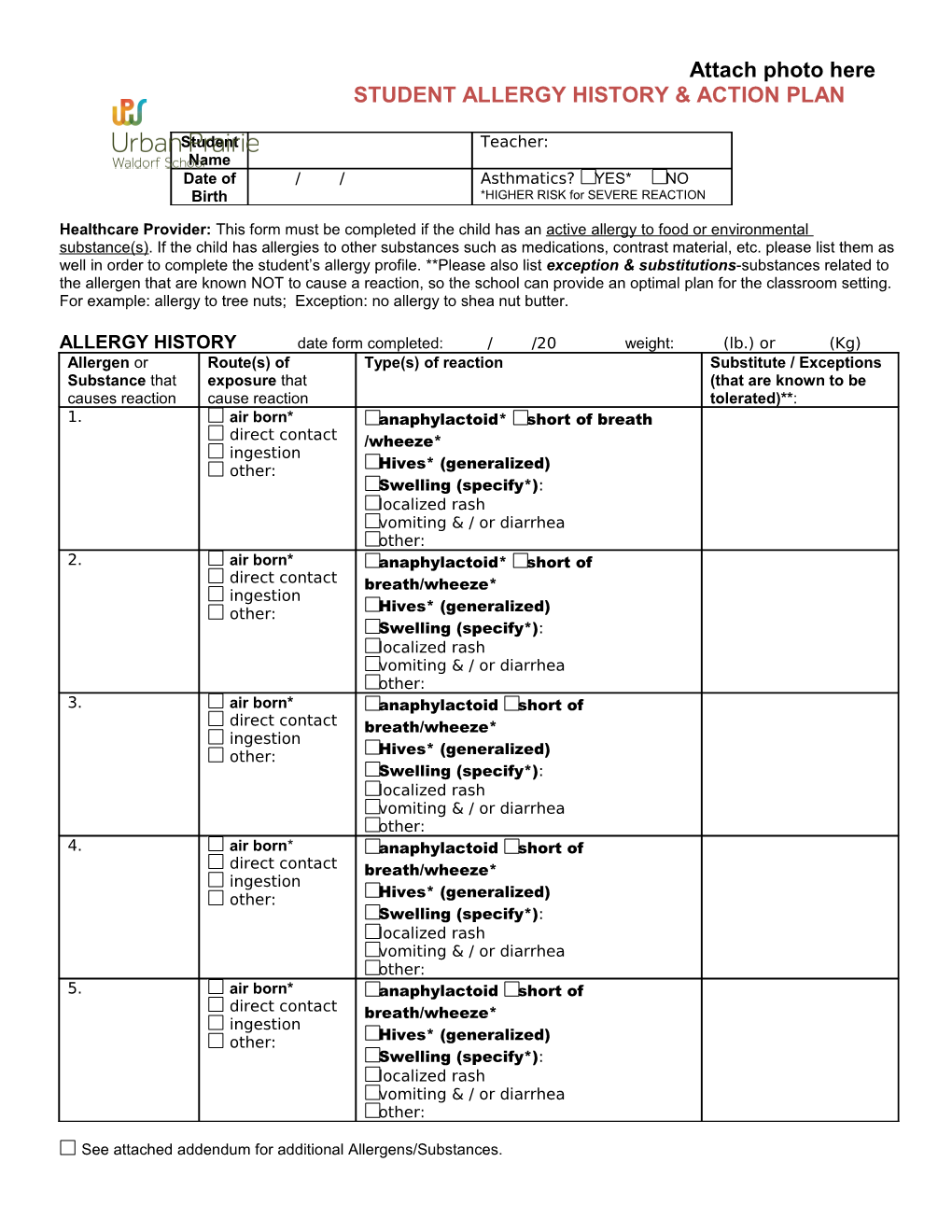
Attach photo here STUDENT ALLERGY HISTORY & ACTION PLAN
Student Teacher: Name Date of / / Asthmatics? YES* NO Birth *HIGHER RISK for SEVERE REACTION
Healthcare Provider: This form must be completed if the child has an active allergy to food or environmental substance(s). If the child has allergies to other substances such as medications, contrast material, etc. please list them as well in order to complete the student’s allergy profile. **Please also list exception & substitutions-substances related to the allergen that are known NOT to cause a reaction, so the school can provide an optimal plan for the classroom setting. For example: allergy to tree nuts; Exception: no allergy to shea nut butter.
ALLERGY HISTORY date form completed: / /20 weight: (lb.) or (Kg) Allergen or Route(s) of Type(s) of reaction Substitute / Exceptions Substance that exposure that (that are known to be causes reaction cause reaction tolerated)**: 1. air born* anaphylactoid* short of breath direct contact /wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: 2. air born* anaphylactoid* short of direct contact breath/wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: 3. air born* anaphylactoid short of direct contact breath/wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: 4. air born* anaphylactoid short of direct contact breath/wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: 5. air born* anaphylactoid short of direct contact breath/wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other:
See attached addendum for additional Allergens/Substances. CLASSROOM RESTRICTIONS *Substances known to cause 1) anaphylactoid reactions, shortness of breath/wheezing, generalized hives or, or airway/mouth/throat/generalized swelling via AIRBORN EXPOSURE or DIRECT CONTACT or 2) any reaction via air born exposure will be restricted from child’s classroom. If other substances pose a health risk in the child’s classroom, please list substance(s) here:
Page 1 of 2
TREATMENT (to be given at school) Page 2 of 2 Symptoms Treatment(s) Determined by Physician or Provider authorizing treatment; medication(s) checked must be provided to school. Severe symptoms: swelling of tongue or tightening Epinephrine of throat, generalized flushing/hives with any of the Antihistamine following: lightheadedness, dizzy, unconscious, thread Steroid (oral) pulse, pale or blue skin color. difficulty breathing, repetitive cough, wheezing, Epinephrine hoarseness. Antihistamine Bronchodilator (inhaler) Steroid (oral) generalized hives or swelling / redness of face or Epinephrine extremities. Antihistamine lip or mouth swelling, itching, tingling (only) Epinephrine Antihistamine Steroid (oral) Vomiting, nausea, cramps, or diarrhea Epinephrine Antihistamine Local reactions: skin rash (itching, red), Antihistamine
MEDICATIONS authorized to be given by school (medication, dose, route must be specified) Epinephrine: EpiPen Jr.® (0.15 mg) EpiPen® (0.3 mg) intramuscularly CALL 911 if used. TwinJect Jr.™0.15 mg TwinJect Jr.™0.3 mg intramuscularly (other): Antihistamine: diphenhydramine (Benedryl®) liquid 12.5mg/tsp chewable 12.5mg/tab 25mg tablet mg by mouth cetirizine (Zyrtec®) liquid 5mg/tsp 10mg tablet mg by mouth (other):
Bronchodilator: albuterol inhaler 1 puff every minute x 2
Steroid (oral): drug: dose: by mouth
Others:
CONTACTS
PARENT/GUARDIANS Phone #1 Phone #2 1) ( ) - ( ) - 2) ( ) - ( ) -
EMERGENCY CONTACTS Phone #1 Phone #2 1) ( ) - ( ) - 2) ( ) - ( ) -
Dr. ( ) - ( ) -
Parent / Guardian Signature: date: Physician/Provider Signature: date:
ADDENDUM: ALLERGY HISTORY
Allergen or Route(s) of Type(s) of reaction Exceptions (substances Substance that exposure that that are known to be causes reaction cause reaction tolerated)**: 6. air born* anaphylactoid* short of breath direct contact /wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: 7. air born* anaphylactoid* short of direct contact breath/wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: 8. air born* anaphylactoid short of direct contact breath/wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: 9. air born* anaphylactoid short of direct contact breath/wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: 10. air born* anaphylactoid short of direct contact breath/wheeze* ingestion other: Hives* (generalized) Swelling (specify*): localized rash vomiting & / or diarrhea other: