Online Appendix to CCMED-D-10-00817 This appendix contains the tabular and graphical data supporting the deliberations of the jury. While they are integral to the consensus document, conservative use of printed space prompted collection in an appendix available online in perpetuity. The figures and table collected herein define the GRADE process of systematic analysis used in the deliberations.
The “included studies” tables compare the trials included in each analysis. Funnel plots accompany those tables where the number of included studies is sufficient to make a visual estimate of the degree of symmetry.
Summary of findings tables collect the GRADE evidence assessment and illuminate the rationale for each GRADE ranking. Each of these summary tables is referenced in the text. Legend to Figures and Tables Table 1: Organizers, speakers and jurors
Table 2: Studies defining levels of temperature management, degrees centigrad e
Table 3: Different temperature ranges for target terms, degrees centigrade
Table 4: Physiological variables for consideration in planning and reporting targeted temperature management
Table 5: Randomized controlled trials evaluated comparing targeted temperature management to unstructured management in cardiac arrest. VF: ventricular fibrillation, VT: ventricular tachycardia, PEA: pulseless electrical activity, d/c: discharge, PAC: pulmonary artery catheter, SD: standard deviation.
Table 6: GRADE summary of findings table for jury analysis of targeted temperature management in ventricular fibrillation/pulseless ventricular tachycardia out-of-hospital cardiac arrest.
Table 7: GRADE summary of findings table for jury analysis of targeted temperature management in asystole/pulseless electrical activity out-of-hospital cardiac arrest.
Table 8. Controlled trials comparing targeted temperature management to unstructured management in perinatal asphyxia. D/C: discharge, SD: standard deviation. Numbers assessed for mortality are listed separately when follow-up was different for this outcome or the neurologic outcome was not assessed.
Table 9: GRADE summary of findings table for jury analysis of targeted temperature management in perinatal asphyxia.
Table 10: Randomized controlled trials evaluated comparing targeted temperature management to unstructured management in traumatic brain injury. NS: not stated, SD: standard deviation.
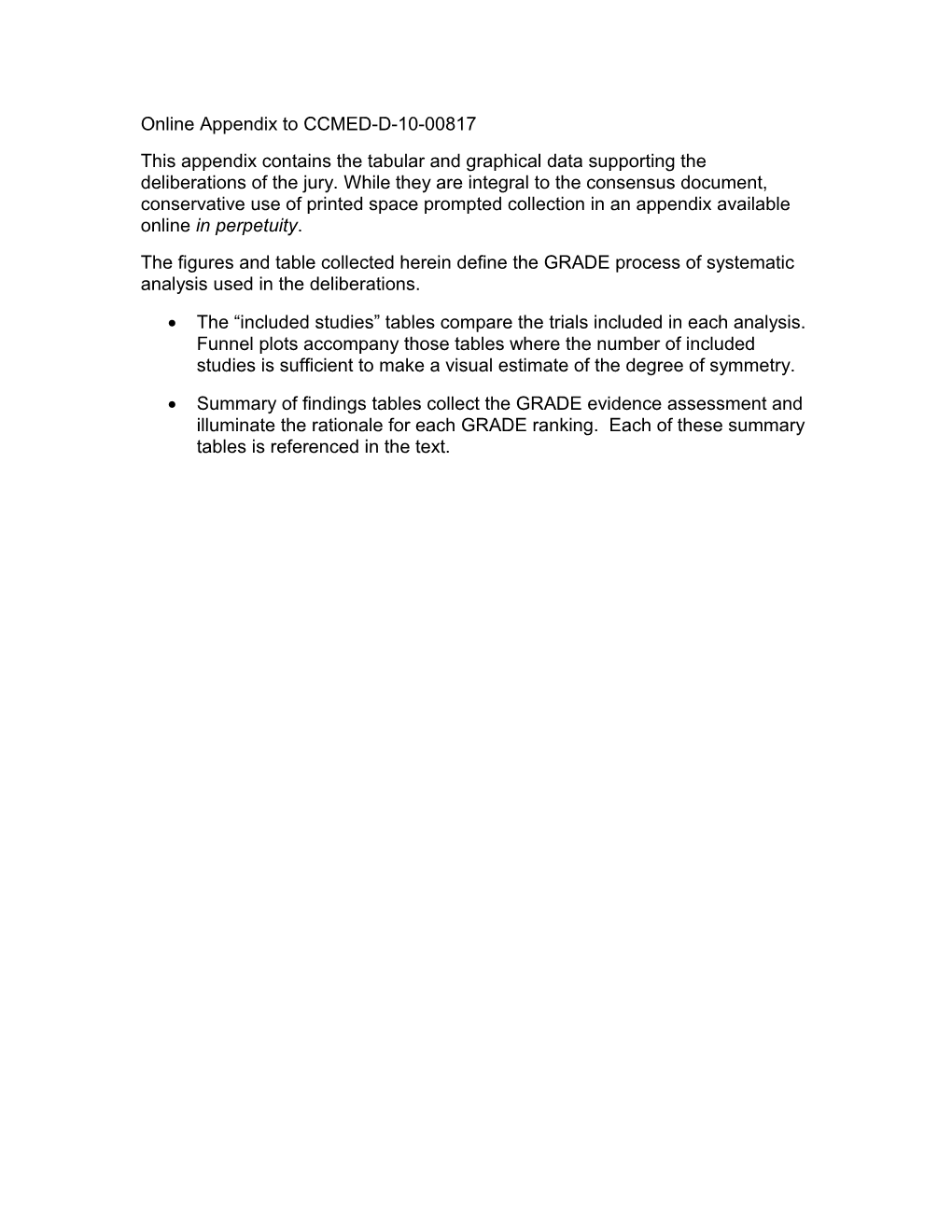
Table 11: GRADE summary of findings table for jury analysis of targeted temperature management in traumatic brain injury. Figure 1. Schematic profile of targeted temperature management
Figure 2: Forest plot: targeted temperature management versus control for ventricular fibrillation/pulseless ventricular tachycardia out-of-hospital cardiac arrest, outcome of survival, follow-up range discharge to 6 months. M-H: Mantel- Haenszel test, CI: confidence interval.
Figure 3: Forest plot: targeted temperature management versus control for ventricular fibrillation/pulseless ventricular tachycardia out-of-hospital cardiac arrest, outcome of favorable neurologic outcome (cerebral-performance category of 1 (good recovery) or 2 (moderate disability), follow-up range discharge to 6 months. M-H: Mantel-Haenszel test, CI: confidence interval.
Figure 4: Forest plot: targeted temperature management versus control for asystole/pulseless electrical activity out-of-hospital cardiac arrest, outcome of survival, in-hospital follow-up. M-H: Mantel-Haenszel test, CI: confidence interval.
Figure 5: Forest plot: targeted temperature management versus control for asystole/pulseless electrical activity out-of-hospital cardiac arrest, favorable neurologic outcome, defined as no, mild or moderate disability by outcome score, in-hospital follow-up. M-H: Mantel Haenszel test, CI: confidence interval.
Figure 6: Forest plot of Holzer M et al.’s meta-analysis of targeted temperature management for cardiac arrest. Outcome: survival to hospital discharge with a favorable neurologic outcome. The risk ratio and 95% confidence interval (CI) are slightly different (1.52 [1.19, 1.95] versus 1.68 [1.29, 2.07]), likely the result of a slightly different statistical method. M-H: Mantel-Haenszel test.
Figure 7: Forest plot, target temperature management versus control for mortality in perinatal asphyxia, follow-up range: discharge to 18 months. M-H: Mantel-Haenszel test, CI: confidence interval. Figure 8: Forest plot, targeted temperature management versus control for death or major disability, defined as severe disability in cognitive or outcomes index, in perinatal asphyxia, follow-up range: 6 to 22 months. M-H: Mantel-Haenszel test, CI: confidence interval.
Figure 9: Forest plot, targeted temperature management versus control for major disability in survivors, defined as severe disability in cognitive or outcomes index, in perinatal asphyxia, follow-up range: 6 to 22 months. M-H: Mantel-Haenszel test, CI: confidence interval.
Figure 10: Funnel plot: targeted temperature management for perinatal asphyxia, outcome of mortality. SE: standard error, OR: odds ratio.
Figure 11: Funnel plot: targeted temperature management for perinatal asphyxia, outcome of death or major disability, follow-up 6-22 months. SE: standard error, OR: odds ratio.
Figure 12: Funnel plot: targeted temperature management for perinatal asphyxia, outcome of major disability in survivors, follow-up range: 6 to 22 months. SE: standard error, OR: odds ratio.
Figure 13: Cochrane meta-analysis: Targeted temperature management for newborn hypoxic ischemic encephalopathy, outcome of mortality stratified by follow-up interval (Jacobs SE, Hunt R, Tarnow-Mordi WO, Inder TE, Davis RG, 2009, The Cochrane Library). M-H: Mantel-Haenszel test, CI: confidence interval.
Figure 14: Cochrane meta-analysis: targeted temperature management for newborn hypoxic ischemic encephalopathy, outcome of death or major disability stratified by follow-up interval (Jacobs SE, Hunt R, Tarnow-Mordi WO, Inder TE, Davis RG, 2009, The Cochrane Library). M-H: Mantel-Haenszel test, CI: confidence interval.
Figure 15: Forest plot, targeted temperature management versus control for mortality in traumatic brain injury, follow-up 3 to 24 months. M-H: Mantel Haenszel test, CI: confidence interval.
Figure 16: Forest plot, targeted temperature management versus control for favorable neurologic outcome in traumatic brain injury, defined as no, mild or moderate disability in cognitive or outcomes index, follow-up 3-24 months. M-H: Mantel-Haenszel test, CI: confidence interval.
Figure 17: Funnel plot: targeted temperature management for traumatic brain injury, outcome of mortality. SE: standard error, OR: odds ratio. Figure 18: Funnel plot: targeted temperature management for traumatic brain injury, outcome of favorable neurologic outcome. SE: standard error, OR: odds ratio.
Figure 19: Cochrane meta-analysis: targeted temperature management for traumatic head injury, outcome: death at final follow-up (Sydenham E, Roberts I, Alderson P, 2009 The Cochrane Library). M-H: Mantel-Haenszel test, CI: confidence interval.
Figure 20: Cochrane meta-analysis: targeted temperature management for traumatic head injury, outcome: unfavorable neurological outcome at final follow- up (Sydenham E, Roberts I, Alderson P, 2009 The Cochrane Library) M-H: Mantel-Haenszel test, CI: confidence interval. Chairs Scientific Advisors Clifford S. Deutschman, MD, MC, FCCM Patrick M. Kochanek, MD, FCCM University of Pennsylvania School of Medicine University of Pittsburgh Medical Center Philadelphia, Pennsylvania, USA Pittsburgh, Pennsylvania, USA
Antoinette Spevetz, MD, FCCM Fritz Sterz, MD Cooper University Hospital Medical University of Vienna Camden, New Jersey, USA Wien, Austria
FACULTY Peter Andrews, MD Patrick M. Kochanek, MD, FCCM Western General Hospital University of Pittsburgh Medical Center Edinburgh, Scotland, United Kingdom Pittsburgh, Pennsylvania, USA
Wilhem Behringer, MD Donald W. Marion, MD Medizinische Universität Wien Boston Medical Center Vienna, Austria Boston, Massachusetts, USA
Nicolas Deye, MD Ken Nagao, MD Lariboisière Hospital Nihon University School of Medicine Paris, France Tokyo, Japan
W. Dalton Dietrich, PhD Samuel M. Poloyac, PharmD, PhD University of Miami School of Medicine University of Pittsburgh School of Pharmacy Miami, Florida, USA Pittsburgh, Pennsylvania, USA
Michael N. Diringer, MD, FCCM John T. Povlishock, PhD Washington University School of Medicine Virginia Commonwealth University St. Louis, Missouri, USA Richmond, Virginia, USA
Simon R. Dixon, MD Stefan Schwab, MD William Beaumont Hospital University of Heidelberg Royal Oak, Michigan, USA Heidelberg, Germany
Larry M. Gentilello, MD Seetha Shankaran, MD University of Texas Southwestern Medical Wayne State University School of Medicine Center Detroit, Michigan, USA Dallas, Texas, USA Fritz Sterz, MD Michael Holzer, MD Medical University of Vienna Medical University of Vienna Wien, Austria Wien, Austria Kjetil Sunde, MD, PhD Jamie S. Hutchison, MD Ulleval University Hospital The Hospital for Sick Children Oslo, Norway Toronto, Ontario, Canada Samuel A. Tisherman, MD, FCCM Francis Kim, MD University of Pittsburgh Medical Center Harborview Medical Center Pittsburgh, Pennsylvania, USA Seattle, Washington, USA
David S. Warner, MD Duke University Medical Center Durham, North Carolina, USA JURORS Jury Chairman Timothy Buchman, MD, PhD, FCCM Gloria M. Rodriguez-Vega, MD, FCCM Washington University School of Medicine University District Hospital St. Louis, Missouri, USA San Juan, Puerto Rico
Geoffrey J. Bellingan, MD Sten Rubertsson, MD, PhD, FCCM University College London Hospitals Uppsala University Hospital London, England, United Kingdom Uppsala, Sweden
Roman Jaeschke, MD Theodoros Vassilakopoulos, MD McMaster University Evangelismos Hospital Hamilton, Ontario, Canada Athens, Greece
Jacques Lacroix, MD Craig Weinert, MD University of Montreal University of Minnesota Montreal, Quebec, Canada Minneapolis, Minnesota, USA
Bruno Mourvillier, MD Sergio Zanotti-Cavazzoni, MD Bichat Claude Bernard Hospital Cooper University Hospital Paris, France Camden, New Jersey, USA
Mark E. Nunnally, MD University of Chicago Chicago, Illinois, USA
Table 1: Organizers, speakers and jurors Author Mild Moderate Deep Wong et al. (1) 32-35 26-31 20-25 Varnathan (2) 32-35 26-31 20-25 Zeiner et al. (3) 34-36 28-33 17-27 Reuler et al.(4) 34-36 28-33 17-27 Hammer et al. (5) >32 28-32 20-28 Safar and Behringer (6) 33-36 28-32 11-27 Werner (7) 34-36 29-33 17-28
Table 2: Studies defining levels of temperature management, degrees centigrad e Author Pathology Target Temperature Term Clifton et al. (8) TBI 33.0 Moderate Bernard (9) Cardiac arrest 33.0 Moderate THACAS Group (10) Cardiac arrest 32-34 Mild Todd et al. (11) Cerebral Aneurysm 32.5-33.5 Mild Shankaran (12) Neonatal Asphyxia 33.5 Not Defined Gluckman et al.(13) Neonatal Asphyxia 34-35 Mild
Table 3: Different temperature ranges for target terms, degrees centigrade Neurologic Electroencephalogram (EEG) slowing, seizures, myoclonus
Cardiovascular Heart rate, Arrhythmias, EKG abnormalities Primary and Derived Hemodynamic measures (Cardiac Output (CO), Systemic Vascular Resistance (SVR)) Fluid balance and use of vasoactive and inotropic agents
Respiratory Increased use of mechanical ventilation (MV), MV days due to need for muscle relaxant and/or additional sedation or analgesia to prevent shivering Oxygenation, saturation Use of alpha-stat or pH stat management strategy (14)
Metabolic Hyperglycemia; insulin requirements for glycemic control Acidosis assessments, including lactate levels
GI Tolerance of enteral feeding; gastroparesis Intestinal function; requirement for parenteral nutrition Stress ulceration
Renal Urine rates and volumes Electrolyte abnormalities (e.g. K, Mg, PO4)
Hematologic Increased blood viscosity (hemoconcentration) Platelet dysfunction Bleeding
Shivering Requirements of sedation, analgesia and/or muscle relaxant CK (Creatine kinase) levels Skin integrity Pressure sore assessments
Infectious Increased risk of infection Pharmacokinetic Reduced drug clearance
Table 4: Physiological variables for consideration in planning and reporting targeted temperature management Numbers of Patients Assessed for Outcome
Mortality (reported Age (mean Durat Arrest Randomize separate or Intentio Target ion of Rhythm d VF/ from Neurologic median), Allocation n to Temper Targe Study Studied Participants VT Neuro Outcome: years Blinding Concealment? Treat? ature ting Indirectness outcome) (follow-up) 1. Bernard SA VF 77 77 77 66a Unblind No Yes 33C 12h >15% of controls 2002 (9) (hospital d/c) ed tympani estimated T>37.5C c or bladder, until PAC inserted 2. Hachimi- Asystole/ 30 0 30 75 Unblind Yes Yes 34C 4h Unclear data on Idrissi S 2001 PEA (unspecified) (median) ed bladder control temp (15) 3. Holzer M VF, 275 265 275 273 59 Unblind Yes Yes 32-34C 24h >15% of controls (HACA) 2002 Pulseless (6mo) (median) ed estimated T>37.5C (10) VT, asystole 4. Kim F 2007 VF & 125 51 125 66 Unblind Yes Yes Not Not Fever in <15% of (16) PEA (hospital ed Specifie specif controls (no VT d/c) d ied seen) Intention to Treat presumed if follow-up numbers reported and no mention of crossover. Portion of patients with T>37.5 degrees C based on SD data or error bars and assumption of a normal distribution. a average of group medians.
Table 5: Randomized controlled trials evaluated comparing targeted temperature management to unstructured management in cardiac arrest. VF: ventricular fibrillation, VT: ventricular tachycardia, PEA: pulseless electrical activity, d/c: discharge, PAC: pulmonary artery catheter, SD: standard deviation. Targeted temperature management (32-34 degrees C) compared to control (less managed) for ventricular fibrillation/pulseless ventricular tachycardia cardiac arrest Patient or population: patients with ventricular fibrillation/pulseless ventricular tachycardia cardiac arrest Settings: out-of hospital Intervention: targeted temperature management (32-34 degrees C) Comparison: control (less managed) Outcomes Illustrative comparative risks (95% CI) Relati No of Quality of the ve participa evidence(GRADE) Assumed risk Corresponding risk effect( nts(studi 95% es) CI)
Control (less Targeted Temperature managed) Management (32-34 degrees C)
Survival: Follow-up interval 428 per 1000 583 per 1000 (483 to 675) OR 403 (3 moderatea discharge to 6 mo 1.87 studies) (1.25 to 2.78)
Good outcome: CPC 1-2 @ 6mos 368 per 1000 540 per 1000(435 to 644) OR 350(2 moderatea (HACA) or D/C home or rehab 2.02 studies) (Bernard) (1.32 to 3.11) The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; CPC: Cerebral Performance Category; D/C: discharge GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. a Temperature > 37.5 degrees C in estimated 15% or more of controls in 2 studies.
Table 6: GRADE summary of findings table for jury analysis of targeted temperature management in ventricular fibrillation/pulseless ventricular tachycardia out-of-hospital cardiac arrest. Targeted temperature management (32-34 degrees C) compared to control (less managed)) for asystole/pulseless ventricular activity cardiac arrest
Patient or population: patients with non ventricular fibrillation cardiac arrestSettings: out-of hospitalIntervention: targeted temperature management (32-34 degrees C)Comparison: control (less managed)
Outcomes Illustrative comparative risks (95% CI) Relative No of Quality of the effect(9 participan evidence(GRADE) Assumed Corresponding risk 5% CI) ts(studies risk )
Control Targeted Temperature (less Management (32-34 managed) degrees C)
Survival to discharge 167 per 101 per 1000(33 to 264) OR 0.56 104(2 very lowa,b,c 1000 (0.17 to studies) 1.79)
Outcome Performance Medium risk populationd OR 5 30(1 lowe Category 1-2 @ discharge (0.22 to study) 10 per 1000 48 per 1000(2 to 534) 113.5) The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio GRADE Working Group grades of evidence: High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. a Kim et al: patients received variable amounts of cooling before admission, after admission at the discretion of receiving physician. b Nonsignificant tests for heterogeneity (p=0.09), but an I squared of 65% with poorly-overlapping confidence intervals. Only 14 events in total. c Results using the fixed model were not significant (p=0.33). d The probability of a good outcome in this small study was zero for the control group; for the purposes of calculation we have assumed this probability to be 1%.e Results using the fixed effects model were not significant (p=0.31). Only 2 events in total.
Table 7: GRADE summary of findings table for jury analysis of targeted temperature management in asystole/pulseless electrical activity out-of-hospital cardiac arrest. Number of Patients Assessed for Outcome
Neurologic Duratio Outcome, n of Including Allocation Target Targetin Study Randomized Mortalit Death: Blinding Concealment? Intention to treat? Temperature g Indirectness Participants y (Follow-Up) 1. Eicher DJ 2005 (18) 65 65 53 Unblinded Yes Yes 32.5-33.5C 48h >15% of controls (12mo) (12mo) rectal estimated T>37.5C 2. Gluckman PD 2005 234 218 Unblinded Yes Yes 34-35C 72h No data on control (13) (18mo) rectal temp 3. Gunn AJ 1998 (19) 22 22 22 Unblinded Yes Yes 35.5-36.5C 72h >15% of controls (12mo) rectal (2 estimated T>37.5C groups) 4. Lin ZL 2006 (20) 62 62 58 Unblinded No Yes 34-35C 72h >15% of controls (5-7d)a (odd or even day) rectal estimated T>37.5C 5. Robertson NJ 2008 36 36 17 Unblinded Yes Yes 33-34C 72h >15% of controls (21) (17d) rectal estimated T>37.5C 6. Shankaran S 2002 19 19 Unblinded Yes Yes 34.5C 72h >15% of controls (22) (D/C) esophageal estimated T>37.5C 7. Shankaran S 2005 208 205 Unblinded Yes Yes 33.5C 72h >15% of controls (12), 2008 (23) (18mo) esophageal estimated T>37.5C 8. Zhou WH 2002 (24) 50 50 Unblinded No Yes 34.5 (SD 72h >15% of controls (6mo) 0.3) C estimated T>37.5C rectal, 34.0 (SD 0.2) C nasopharyng eal (2 groups)
Intention to Treat presumed if follow-up numbers reported and no mention of crossover. Proportion of patients with T>37.5 degrees C based on SD data or error bars and assumption of a normal distribution. a: Head CT findings. Not included in disability assessment. Table 8. Controlled trials comparing targeted temperature management to unstructured management in perinatal asphyxia. D/C: discharge, SD: standard deviation. Numbers assessed for mortality are listed separately when follow-up was different for this outcome or the neurologic outcome was not assessed. Targeted temperature management (32.5-36.5 degrees C) compared to control (less managed ) for perinatal asphyxia Patient or population: patients with perinatal asphyxia Settings: in-hospital Intervention: targeted temperature management (32.5-36.5 degrees C) Comparison: control (less managed) Outcomes Illustrative comparative risks (95% Relative No of Quality of the CI) effect(95% participant evidence(GRADE) CI) s(studies) Assumed Corresponding risk risk
Control Targeted Temperature (less Management (32.5- managed) 36.5 degrees C)
Death: Follow-up interval 302 per 243 per 1000(184 to OR 0.74 (0.52 677(8 lowa,b discharge to 18 months 1000 312) to 1.05) studies)
Death or severe disability: 601 per 444 per 1000(364 to OR 0.53 (0.38 548(5 moderatec Follow-up interval 6-22 1000 534) to 0.76) studies) months
Severe disability in 389 per 259 per 1000(182 to OR 0.55 (0.35 380(5 moderatec survivors: Follow-up interval 1000 351) to 0.85) studies) 6-22 months The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. a Temperature > 37.5 degrees C in estimated 15% or more controls in 7 studies, no data in 1 study. b Results nonsignificant: OR 0.74 [0.52, 1.05]. c Temperature > 37.5 degrees C in estimated 15% or more of controls in 4 studies, no data in 1 study.
Table 9: GRADE summary of findings table for jury analysis of targeted temperature management in perinatal asphyxia. Number of patients assessed Age Duration (mean or Intenti Target of Random Neurologic Outcome median), Allocation on to Tempera Targetin Study ized Hospital years Blinding Concealment? treat? ture g Indirectness death 3mo 6mo other 1. Adelson PD 2005 75 75 69 67 6.91 Unblind Yes 2 TTM 32-33C 48h >15% of (25) ed pts to rectal controls control estimated T>37.5C 2. Biswas AK 2002 (26) 21 21 18 14 6.21 Unblind Unclear Yes 32-34C 48h >15% of (12mo) ed rectal controls estimated T>37.5C 3. Clifton GL 1993 (27) 46 45 45 NS Unblind Yes Yes 33C 48h >15% of (Adult) ed PAC controls estimated T>37.5C 4. Clifton GL 2001(8) 392 368 31.5 Unblind Yes Yes 33C 48h >15% of ed bladder controls estimated T>37.5C 5. Hutchison JS 2008 225 205 10.0 Unblind Yes Yes 32.5 24h Fever in <15% (28) ed (SD 0.5) of controls C esophag eal 6. Jiang J 2000 (29) 87 87 41.4 Unblind Unclear Yes 33-35C 3-14d, >15% of (12mo) ed rectal based on controls ICP estimated T>37.5C 7. Liu WG 2006 (30) 66 66 40.6 Unblind Unclear Yes 33-35C 72h No data on (24mo) ed rectal, control temp 33-35C brain group 8. Marion DW 1993 40 40 32.0 Unblind Yes Yes 33C 24h >15% of (31) ed brain controls estimated T>37.5C 9. Marion DW 1997 82 82 82 81 33 Unblind Yes Yes 32-33C 24h >15% of (32) (12mo) ed rectal controls estimated T>37.5C 10. Qiu W 2005 (33) 86 86 41.2 Unblind No Yes 33-35C 3-5d >15% of (24mo) ed nasopha (mean controls ryngeal 4.3d) estimated or brain T>37.5C 11. Shiozaki T 1993 33 33 35.4 Unblind Unclear Yes 33.5- 48h No data on (34) ed 34.5C control temp bladder 12. Shiozaki T 1999 16 16 35.8 Unblind Unclear Yes 33.5- 48h Fever in <15% (35) ed 34.5C of controls intracran ial 13. Shiozaki T 2001 91 91 NS Unblind Unclear Yes 33.5- 48h Fever in <15% (36) (1pt<9yr ed 34.5C of controls ) core or brain 14. Smrcka M 2005 72 72 41 Unblind Unclear Yes 34C 72h No data on (37) ed bladder control temp 15. Wang W 2005 (38) 40 40a NS Unblind Unclear Yes 33.5- 48h No data on ed 34.5C control temp intracran ial 16. Zhi D 2003 (39) 396 396 42.5 Unblind Unclear Yes 32-35C 1-7d No data on ed rectal (mean control temp (SD) 62(28)h) Intention to Treat presumed if follow-up numbers reported and no mention of crossover. Proportion of patients with T>37.5 degrees C based on SD data or error bars and assumption of a normal distribution. a: Favorable outcome did not include moderate disability.
Table 10: Randomized controlled trials evaluated comparing targeted temperature management to unstructured management in traumatic brain injury. NS: not stated, SD: standard deviation. Targeted temperature management (32-35 degrees C) compared to control (less managed) for traumatic brain injury Patient or population: patients with traumatic brain injury Settings: in-hospital Intervention: targeted temperature management (32-35 degrees C) Comparison: control (less managed) Outcomes Illustrative comparative risks (95% CI) Relative No of Quality of the effect participan evidence(GR Assumed Corresponding risk (95% CI) ts(studies ADE) risk )
Control Targeted Temperature (less Management (32-35 managed) degrees C)
Death: Follow-up interval 291 per 223 per 1000(165 to 293) OR 0.7 1702(15 lowa,b discharge-24mo 1000 (0.48 to studies) 1.01)
Favorable neurologic 460 per 594 per 1000(497 to 686) OR 1.72 1715(16 lowc,d outcome (GOS 4-5, CPC 1-3 1000 (1.16 to studies) @ 3-12mo) 2.56) The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; OR: Odds ratio; GOS: Glasgow Outcome Score; CPC: Cerebral Performance Category GRADE Working Group grades of evidence: High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. a I squared = 50%, Significant test for heterogeneity. b Temperature > 37.5 degrees in estimated 15% or more of controls in 8 studies, no data in 4 studies. c I squared = 66%, significant test for heterogeneity. d Temperature > 37.5 degrees in estimated 15% or more of controls in 8 studies, no data in 5 studies.
Table 11: GRADE summary of findings table for jury analysis of targeted temperature management in traumatic brain injury. Targeted Temperature Management
37 Induction phase. Typically, cooling as ) C
fast as possible, at
s 36
e least 3⁰C/hr e r g
e 35 D (
e
r Maintenance phase. u t 34 Control to within 0.5 ⁰C a r e
p Reversion phase.
m 33 Managed recovery to e T
target level, typically e r normal or just below o 32 C normal, warming rates typically 0.3 ⁰C/hr 31 0 500 1000 1500 2000 2500 3000 Profile Time (minutes)
Figure 1. Schematic Profile of Targeted Temperature Management Experimental Control Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI Bernard S 2002 21 43 11 34 17.7% 2.00 [0.78, 5.08] Holzer HACA 2002 81 137 62 138 71.2% 1.77 [1.10, 2.86] Kim F 2007 19 29 10 22 11.1% 2.28 [0.73, 7.10]
Total (95% CI) 209 194 100.0% 1.87 [1.25, 2.78] Total events 121 83 Heterogeneity: Chi² = 0.18, df = 2 (P = 0.91); I² = 0% 0.01 0.1 1 10 100 Test for overall effect: Z = 3.08 (P = 0.002) Favours control Favours experimental Figure 2: Forest plot: targeted temperature management versus control for ventricular fibrillation/pulseless ventricular tachycardia out-of-hospital cardiac arrest, outcome of survival, follow-up range discharge to 6 months. M-H: Mantel- Haenszel test, CI: Confidence interval. Experimental Control Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI Bernard S 2002 21 43 9 34 17.3% 2.65 [1.01, 6.98] Holzer HACA 2002 74 136 54 137 82.7% 1.83 [1.13, 2.97]
Total (95% CI) 179 171 100.0% 1.98 [1.29, 3.04] Total events 95 63 Heterogeneity: Chi² = 0.45, df = 1 (P = 0.50); I² = 0% 0.01 0.1 1 10 100 Test for overall effect: Z = 3.11 (P = 0.002) Favours control Favours experimental Figure 3: Forest plot: targeted temperature management versus control for ventricular fibrillation/pulseless ventricular tachycardia out-of-hospital cardiac arrest, outcome of favorable neurologic outcome (cerebral-performance category of 1 (good recovery) or 2 (moderate disability), follow-up range discharge to 6 months. M-H: Mantel-Haenszel test, CI: Confidence interval. Experimental Control Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI Hachimi-Idrissi 2001 3 16 1 14 11.1% 3.00 [0.27, 32.75] Kim F 2007 2 34 8 40 88.9% 0.25 [0.05, 1.27]
Total (95% CI) 50 54 100.0% 0.56 [0.17, 1.79] Total events 5 9 Heterogeneity: Chi² = 2.84, df = 1 (P = 0.09); I² = 65% 0.01 0.1 1 10 100 Test for overall effect: Z = 0.98 (P = 0.33) Favours control Favours experimental Figure 4: Forest plot: targeted temperature management versus control for asystole/pulseless electrical activity out-of-hospital cardiac arrest, outcome of survival, in-hospital follow-up. M-H: Mantel-Haenszel test, CI: Confidence interval. Experimental Control Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI Hachimi-Idrissi 2001 2 16 0 14 100.0% 5.00 [0.22, 113.50]
Total (95% CI) 16 14 100.0% 5.00 [0.22, 113.50] Total events 2 0 Heterogeneity: Not applicable 0.01 0.1 1 10 100 Test for overall effect: Z = 1.01 (P = 0.31) Favours control Favours experimental Figure 5: Forest plot: targeted temperature management versus control for asystole/pulseless electrical activity out-of-hospital cardiac arrest, favorable neurologic outcome, defined as no, mild or moderate disability by outcome score, in-hospital follow- Experimental Control Risk Ratio Risk Ratio Study or Subgroup Events Total Events Total Weight M-H, Random, 95% CI M-H, Random, 95% CI Bernard SA 2002 21 43 9 34 15.2% 1.84 [0.97, 3.49] HACA 2002 72 136 50 137 84.0% 1.45 [1.11, 1.90] Hachimi-Idrissi S 2001 3 16 0 17 0.7% 7.41 [0.41, 133.11]
Total (95% CI) 195 188 100.0% 1.52 [1.19, 1.95] Total events 96 59 Heterogeneity: Tau² = 0.00; Chi² = 1.67, df = 2 (P = 0.43); I² = 0% 0.01 0.1 1 10 100 Test for overall effect: Z = 3.31 (P = 0.0009) Favours control Favours experimental Figure 6: Forest plot of Holzer M et al.’s meta-analysis of targeted temperature management for cardiac arrest. Outcome: survival to hospital discharge with a favorable neurologic outcome. The Risk Ratio and 95% Confidence Interval (CI) are slightly different (1.52 [1.19, 1.95] versus 1.68 [1.29, 2.07]), likely the result of a slightly different statistical method. M-H: Mantel-Haenszel test. Experimental Control Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI Battin MR 2001 3 25 3 15 4.3% 0.55 [0.09, 3.13] Eicher DJ 2005 10 32 14 33 12.4% 0.62 [0.22, 1.71] Gluckman PD 2005 36 108 42 110 36.4% 0.81 [0.46, 1.41] Gunn AJ 1998 2 12 2 10 2.4% 0.80 [0.09, 7.00] Lin ZL 2006 2 32 2 30 2.5% 0.93 [0.12, 7.08] Robertson N 2008 7 21 1 15 1.0% 7.00 [0.76, 64.61] Shankaran S 2002 2 9 3 10 2.9% 0.67 [0.08, 5.30] Shankaran S 2005 24 102 38 103 38.0% 0.53 [0.29, 0.97] Zhou WH 2002 0 23 0 27 Not estimable
Total (95% CI) 364 353 100.0% 0.73 [0.52, 1.03] Total events 86 105 Heterogeneity: Chi² = 5.50, df = 7 (P = 0.60); I² = 0% 0.01 0.1 1 10 100 Test for overall effect: Z = 1.81 (P = 0.07) Favours experimental Favours control Figure 7: Forest plot, target temperature management versus control for mortality in perinatal asphyxia, follow-up range: discharge to 18 months. M-H: Mantel-Haenszel test, CI: confidence interval. Experimental Control Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI Battin MR 2001 7 25 4 13 4.2% 0.88 [0.20, 3.79] Eicher DJ 2005 14 27 19 26 10.3% 0.40 [0.13, 1.25] Gluckman PD 2005 59 108 73 110 36.3% 0.61 [0.35, 1.06] Gunn AJ 1998 3 12 3 10 2.7% 0.78 [0.12, 5.10] Shankaran S 2005 43 102 63 103 40.1% 0.46 [0.26, 0.81] Zhou WH 2002 5 23 8 27 6.4% 0.66 [0.18, 2.40]
Total (95% CI) 297 289 100.0% 0.55 [0.39, 0.77] Total events 131 170 Heterogeneity: Chi² = 1.41, df = 5 (P = 0.92); I² = 0% 0.01 0.1 1 10 100 Test for overall effect: Z = 3.48 (P = 0.0005) Favours experimental Favours control Figure 8: Forest plot, targeted temperature management versus control for death or major disability, defined as severe disability in cognitive or outcomes index, in perinatal asphyxia, follow-up range: 6 to 22 months. M-H: Mantel-Haenszel test, CI: confidence interval. Experimental Control Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI Battin MR 2001 4 22 1 10 2.1% 2.00 [0.19, 20.61] Eicher DJ 2005 4 17 5 12 8.2% 0.43 [0.09, 2.14] Gluckman PD 2005 23 72 31 68 39.7% 0.56 [0.28, 1.11] Gunn AJ 1998 1 10 1 8 1.8% 0.78 [0.04, 14.75] Shankaran S 2005 19 78 25 65 37.7% 0.52 [0.25, 1.06] Zhou WH 2002 5 23 8 27 10.5% 0.66 [0.18, 2.40]
Total (95% CI) 222 190 100.0% 0.58 [0.38, 0.89] Total events 56 71 Heterogeneity: Chi² = 1.40, df = 5 (P = 0.92); I² = 0% 0.01 0.1 1 10 100 Test for overall effect: Z = 2.51 (P = 0.01) Favours experimental Favours control Figure 9: Forest plot, targeted temperature management versus control for major disability in survivors, defined as severe disability in cognitive or outcomes index, in perinatal asphyxia, follow-up range: 6 to 22 months. M-H: Mantel-Haenszel test, CI: confidence interval. SE(log[OR]) 0
0.5
1
1.5
OR 2 0.01 0.1 1 10 100 Figure 10: Funnel plot: targeted temperature management for perinatal asphyxia, outcome of mortality. SE: Standard error, OR: Odds ratio. SE(log[OR]) 0
0.2
0.4
0.6
0.8
OR 1 0.01 0.1 1 10 100 Figure 11: Funnel plot: targeted temperature management for perinatal asphyxia, outcome of death or major disability, follow-up 6-22 months. SE: Standard error, OR: Odds ratio. SE(log[OR]) 0
0.5
1
1.5
OR 2 0.01 0.1 1 10 100 Figure 12: Funnel plot: targeted temperature management for perinatal asphyxia, outcome of major disability in survivors, follow-up range: 6 to 22 months. SE: Standard error, OR: Odds ratio. Experimental Control Risk Ratio Risk Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI 1.2.2 Long term Follow-up 18-22 months Gluckman 2005 36 108 42 110 39.0% 0.87 [0.61, 1.25] Gunn 1998 3 18 3 13 3.3% 0.72 [0.17, 3.03] Shankaran 2005 24 102 38 103 35.4% 0.64 [0.41, 0.98] Subtotal (95% CI) 228 226 77.7% 0.76 [0.58, 0.99] Total events 63 83 Heterogeneity: Chi² = 1.22, df = 2 (P = 0.54); I² = 0% Test for overall effect: Z = 2.00 (P = 0.05)
1.2.3 Short-term Folow-up 12 months or less Akisu 2003 0 11 2 10 2.4% 0.18 [0.01, 3.41] Eicher 2005 10 32 14 33 12.9% 0.74 [0.38, 1.41] ICE 2002 1 7 3 10 2.3% 0.48 [0.06, 3.69] Lin 2006 2 32 2 30 1.9% 0.94 [0.14, 6.24] Shankaran 2002 2 9 3 10 2.7% 0.74 [0.16, 3.48] Subtotal (95% CI) 91 93 22.3% 0.67 [0.39, 1.15] Total events 15 24 Heterogeneity: Chi² = 1.09, df = 4 (P = 0.90); I² = 0% Test for overall effect: Z = 1.47 (P = 0.14)
Total (95% CI) 319 319 100.0% 0.74 [0.58, 0.94] Total events 78 107 Heterogeneity: Chi² = 2.40, df = 7 (P = 0.93); I² = 0% 0.01 0.1 1 10 100 Test for overall effect: Z = 2.45 (P = 0.01) Favours experimental Favours control Test for subgroup differences: Not applicable Figure 13: Cochrane Meta-Analysis: Targeted temperature management for newborn hypoxic ischemic encephalopathy, outcome of mortality stratified by follow-up interval (Jacobs SE, Hunt R, Tarnow-Mordi WO, Inder TE, Davis RG, 2009, The Cochrane Library). M-H: Mantel-Haenszel test, CI: confidence interval. Experimental Control Risk Ratio Risk Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI 1.1.1 High quality follow-up at 18-22 months Gluckman 2005 59 108 73 110 44.5% 0.82 [0.66, 1.02] Gunn 1998 7 18 4 13 2.9% 1.26 [0.46, 3.44] Shankaran 2005 45 102 64 103 39.2% 0.71 [0.54, 0.93] Subtotal (95% CI) 228 226 86.6% 0.79 [0.67, 0.93] Total events 111 141 Heterogeneity: Chi² = 1.60, df = 2 (P = 0.45); I² = 0% Test for overall effect: Z = 2.82 (P = 0.005)
1.1.2 Lower quality follow-up at 12 months Eicher 2005 14 27 21 25 13.4% 0.62 [0.41, 0.92] Subtotal (95% CI) 27 25 13.4% 0.62 [0.41, 0.92] Total events 14 21 Heterogeneity: Not applicable Test for overall effect: Z = 2.35 (P = 0.02)
Total (95% CI) 255 251 100.0% 0.76 [0.65, 0.89] Total events 125 162 Heterogeneity: Chi² = 2.80, df = 3 (P = 0.42); I² = 0% 0.01 0.1 1 10 100 Test for overall effect: Z = 3.42 (P = 0.0006) Favours experimental Favours control Test for subgroup differences: Not applicable Figure 14: Cochrane Meta-Analysis: targeted temperature management for newborn hypoxic ischemic encephalopathy, outcome of death or major disability stratified by follow-up interval (Jacobs SE, Hunt R, Tarnow-Mordi WO, Inder TE, Davis RG, 2009, The Cochrane Library). M-H: Mantel-Haenszel test, CI: confidence interval. TTM (32-35) Control (36.5-38.5) Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Random, 95% CI M-H, Random, 95% CI Adelson PD 2005 7 37 7 38 6.3% 1.03 [0.32, 3.30] Biswas AK 2002 3 10 0 11 1.3% 10.73 [0.48, 238.90] Clifton GL 1993 8 23 8 22 5.9% 0.93 [0.28, 3.16] Clifton GL 2001 53 190 48 178 13.4% 1.05 [0.66, 1.66] Hutchinson JS 2008 23 108 14 117 10.2% 1.99 [0.97, 4.11] Jiang J 2000 11 43 20 44 8.4% 0.41 [0.17, 1.02] Liu WG 2006 11 43 12 23 7.0% 0.32 [0.11, 0.92] Marion DW 1993 0 20 2 20 1.3% 0.18 [0.01, 4.01] Marion DW 1997 9 39 10 42 7.3% 0.96 [0.34, 2.69] Qiu W 2005 11 43 22 43 8.3% 0.33 [0.13, 0.81] Shiozaki T 1993 8 16 14 17 4.1% 0.21 [0.04, 1.05] Shiozaki T 1999 0 8 0 8 Not estimable Shiozaki T2001 8 45 6 46 6.4% 1.44 [0.46, 4.55] Smrcka M 2005 5 35 11 37 6.2% 0.39 [0.12, 1.28] Zhi D 2002 51 198 72 198 13.8% 0.61 [0.39, 0.93]
Total (95% CI) 858 844 100.0% 0.72 [0.50, 1.04] Total events 208 246 Heterogeneity: Tau² = 0.21; Chi² = 26.40, df = 13 (P = 0.02); I² = 51% 0.005 0.1 1 10 200 Test for overall effect: Z = 1.77 (P = 0.08) Favours experimental Favours control Figure 15: Forest Plot, targeted temperature management (TTM) versus control for mortality in traumatic brain injury, follow-up 3 to 24 months. M-H: Mantel Haenszel test, CI: Confidence interval. TTM (32-35) Control (36.5-38.5) Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Random, 95% CI M-H, Random, 95% CI Adelson PD 2005 14 32 14 36 6.9% 1.22 [0.46, 3.22] Biswas AK 2002 7 10 11 11 1.4% 0.09 [0.00, 2.07] Clifton GL 1993 12 23 8 22 5.6% 1.91 [0.58, 6.30] Clifton GL 2001 82 190 76 178 10.4% 1.02 [0.67, 1.54] Hutchinson JS 2008 70 102 80 103 9.0% 0.63 [0.34, 1.17] Jiang J 2000 20 43 12 44 7.3% 2.32 [0.95, 5.67] Liu WG 2006 28 43 8 23 6.3% 3.50 [1.21, 10.13] Marion DW 1993 12 20 8 20 5.3% 2.25 [0.63, 7.97] Marion DW 1997 24 39 16 42 7.3% 2.60 [1.06, 6.37] Qiu W 2005 28 43 16 43 7.4% 3.15 [1.31, 7.60] Shiozaki T 1993 6 16 1 17 2.4% 9.60 [1.00, 91.96] Shiozaki T 1999 6 8 7 8 1.9% 0.43 [0.03, 5.98] Shiozaki T2001 21 45 27 46 7.7% 0.62 [0.27, 1.41] Smrcka M 2005 30 35 18 37 5.9% 6.33 [2.01, 19.91] Wang W 2005 15 20 13 20 4.9% 1.62 [0.41, 6.34] Zhi D 2002 122 198 75 198 10.4% 2.63 [1.75, 3.95]
Total (95% CI) 867 848 100.0% 1.73 [1.17, 2.56] Total events 497 390 Heterogeneity: Tau² = 0.34; Chi² = 43.00, df = 15 (P = 0.0002); I² = 65% 0.005 0.1 1 10 200 Test for overall effect: Z = 2.73 (P = 0.006) Favours control Favours experimental Figure 16: Forest plot, targeted temperature management (TTM) versus control for favorable neurologic outcome in traumatic brain injury, defined as no, mild or moderate disability in cognitive or outcomes index, follow-up 3-24 months. M-H: Mantel-Haenszel test, CI: Confidence interval. SE(log[OR]) 0
0.5
1
1.5
OR 2 0.005 0.1 1 10 200 Figure 17: Funnel plot: targeted temperature management for traumatic brain injury, outcome of mortality. SE: Standard error, OR: Odds ratio. SE(log[OR]) 0
0.5
1
1.5
OR 2 0.005 0.1 1 10 200 Figure 18: Funnel plot: targeted temperature management for traumatic brain injury, outcome of favorable neurologic outcome. SE: Standard error, OR: Odds ratio. Hypothermia Control Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI 1.1.2 Concealled allocation Adelson 2005 HYPO I 4 25 4 25 2.0% 1.00 [0.22, 4.54] Adelson 2005 HYPO II 3 14 3 13 1.5% 0.91 [0.15, 5.58] Clifton 1992 1 5 1 5 0.5% 1.00 [0.05, 22.18] Clifton 1993 8 23 8 22 3.2% 0.93 [0.28, 3.16] Clifton 2001 53 190 48 178 21.6% 1.05 [0.66, 1.66] Hutchinson 2008 23 102 14 103 6.5% 1.85 [0.89, 3.84] Marion 1997 9 39 10 42 4.5% 0.96 [0.34, 2.69] Meissner 1998 3 12 3 13 1.3% 1.11 [0.18, 6.97] Qiu 2007 9 40 13 40 6.1% 0.60 [0.22, 1.63] Subtotal (95% CI) 450 441 47.3% 1.08 [0.79, 1.47] Total events 113 104 Heterogeneity: Chi² = 3.58, df = 8 (P = 0.89); I² = 0% Test for overall effect: Z = 0.49 (P = 0.62)
1.1.3 Non-concealed allocation Aibiki 2000 1 15 3 11 2.0% 0.19 [0.02, 2.15] Biswas 2002 3 8 0 6 0.2% 8.27 [0.35, 197.61] Hashiguchi 2003 1 9 0 8 0.3% 3.00 [0.11, 84.56] Hirayama 2004 4 12 5 10 2.2% 0.50 [0.09, 2.81] Jiang 2000 11 43 20 44 8.9% 0.41 [0.17, 1.02] Meissner 2003b 3 15 3 13 1.6% 0.83 [0.14, 5.08] Shiozaki 1993 8 16 14 17 4.1% 0.21 [0.04, 1.05] Shiozaki 1999 0 8 0 8 Not estimable Shiozaki 2001 8 45 6 46 3.0% 1.44 [0.46, 4.55] Smrcka 2005 5 35 11 37 5.5% 0.39 [0.12, 1.28] Yan 2001 13 24 16 20 4.8% 0.30 [0.08, 1.15] Zhang 2000 41 123 50 123 20.2% 0.73 [0.43, 1.23] Subtotal (95% CI) 353 343 52.7% 0.62 [0.44, 0.86] Total events 98 128 Heterogeneity: Chi² = 11.14, df = 10 (P = 0.35); I² = 10% Test for overall effect: Z = 2.83 (P = 0.005)
Total (95% CI) 803 784 100.0% 0.84 [0.67, 1.05] Total events 211 232 Heterogeneity: Chi² = 20.61, df = 19 (P = 0.36); I² = 8% 0.01 0.1 1 10 100 Test for overall effect: Z = 1.57 (P = 0.12) Favours experimental Favours control Figure 19: Cochrane Meta-Analysis: targeted temperature management for traumatic head injury, outcome: death at final follow-up (Sydenham E, Roberts I, Alderson P, 2009 The Cochrane Library). M-H: Mantel-Haenszel test, CI: confidence interval. Immediate Hypothermia Normothermia Odds Ratio Odds Ratio Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI 1.2.2 Concealed allocation Adelson 2005 HYPO I 4 25 4 25 1.6% 1.00 [0.22, 4.54] Adelson 2005 HYPO II 3 14 3 13 1.2% 0.91 [0.15, 5.58] Clifton 1992 1 5 2 5 0.8% 0.38 [0.02, 6.35] Clifton 1993 11 23 14 22 3.6% 0.52 [0.16, 1.73] Clifton 2001 108 190 102 178 22.1% 0.98 [0.65, 1.48] Hutchinson 2008 32 102 23 103 7.6% 1.59 [0.85, 2.97] Marion 1997 15 39 26 42 7.5% 0.38 [0.16, 0.94] Meissner 1998 3 12 3 13 1.0% 1.11 [0.18, 6.97] Qiu 2007 9 40 13 40 4.9% 0.60 [0.22, 1.63] Subtotal (95% CI) 450 441 50.3% 0.91 [0.69, 1.20] Total events 186 190 Heterogeneity: Chi² = 8.66, df = 8 (P = 0.37); I² = 8% Test for overall effect: Z = 0.68 (P = 0.49)
1.2.3 Non-concealed allocation Aibiki 2000 3 15 7 11 3.1% 0.14 [0.02, 0.83] Biswas 2002 3 8 0 6 0.2% 8.27 [0.35, 197.61] Hashiguchi 2003 3 9 1 8 0.3% 3.50 [0.28, 43.16] Hirayama 2004 4 12 7 10 2.5% 0.21 [0.04, 1.31] Jiang 2000 23 43 32 44 7.1% 0.43 [0.18, 1.05] Meissner 2003b 3 15 3 13 1.2% 0.83 [0.14, 5.08] Shiozaki 1993 10 16 16 17 2.8% 0.10 [0.01, 1.00] Shiozaki 1999 2 8 1 8 0.4% 2.33 [0.17, 32.58] Shiozaki 2001 24 45 19 46 4.3% 1.62 [0.71, 3.72] Smrcka 2005 5 35 19 37 7.7% 0.16 [0.05, 0.50] Yan 2001 13 24 16 20 3.9% 0.30 [0.08, 1.15] Zhang 2000 41 123 50 123 16.2% 0.73 [0.43, 1.23] Subtotal (95% CI) 353 343 49.7% 0.60 [0.44, 0.82] Total events 134 171 Heterogeneity: Chi² = 24.64, df = 11 (P = 0.01); I² = 55% Test for overall effect: Z = 3.19 (P = 0.001)
Total (95% CI) 803 784 100.0% 0.76 [0.61, 0.93] Total events 320 361 Heterogeneity: Chi² = 36.70, df = 20 (P = 0.01); I² = 45% 0.01 0.1 1 10 100 Test for overall effect: Z = 2.65 (P = 0.008) Favours experimental Favours control Test for subgroup differences: Not applicable Figure 20: Cochrane Meta-Analysis: targeted temperature management for traumatic head injury, outcome: unfavorable neurological outcome at final follow-up (Sydenham E, Roberts I, Alderson P, 2009 The Cochrane Library) M-H: Mantel-Haenszel test, CI: confidence interval.
1. Wong KC. Physiology and pharmacology of hypothermia. West J Med. 1983 Feb;138(2):227-32. 2. Varathan S, Shibuta S, Shimizu T, Mashimo T. Neuroprotective effect of hypothermia at defined intraischemic time courses in cortical cultures. J Neurosci Res. 2001 Sep 15;65(6):583-90. 3. Zeiner A, Holzer M, Sterz F, Behringer W, Schorkhuber W, Mullner M, et al. Mild resuscitative hypothermia to improve neurological outcome after cardiac arrest. A clinical feasibility trial. Hypothermia After Cardiac Arrest (HACA) Study Group. Stroke. 2000 Jan;31(1):86-94. 4. Reuler JB. Hypothermia: pathophysiology, clinical settings, and management. Ann Intern Med. 1978 Oct;89(4):519-27. 5. Hammer MD, Krieger DW. Acute ischemic stroke: is there a role for hypothermia? Cleve Clin J Med. 2002 Oct;69(10):770, 3-4, 6-7 passim. 6. Safar P, Behringer W. Brain resuscitation after cardiac arrest. . In: Layon AJ, Gabrielli A, Friedman W, editors. Textbook of neurointensive care. ed. Philadelphia: Saunders; 2003. p. 457-98. 7. Werner C. [Mild and moderate hypothermia as a new therapy concept in treatment of cerebral ischemia and craniocerebral trauma. Pathophysiologic principles]. Anasthesiol Intensivmed Notfallmed Schmerzther. 1997 Apr;32(4):210-8. 8. Clifton GL, Miller ER, Choi SC, Levin HS, McCauley S, Smith KR, Jr., et al. Lack of effect of induction of hypothermia after acute brain injury. N Engl J Med. 2001 Feb 22;344(8):556-63. 9. Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002 Feb 21;346(8):557-63. 10. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002 Feb 21;346(8):549-56. 11. Todd MM, Hindman BJ, Clarke WR, Torner JC. Mild intraoperative hypothermia during surgery for intracranial aneurysm. N Engl J Med. 2005 Jan 13;352(2):135-45. 12. Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE, McDonald SA, Donovan EF, et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med. 2005 Oct 13;353(15):1574-84. 13. Gluckman PD, Wyatt JS, Azzopardi D, Ballard R, Edwards AD, Ferriero DM, et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial. Lancet. 2005 Feb 19-25;365(9460):663- 70. 14. Kollmar R, Georgiadis D, Schwab S. Alpha-stat versus pH-stat guided ventilation in patients with large ischemic stroke treated by hypothermia. Neurocrit Care. 2009;10(2):173-80. 15. Hachimi-Idrissi S, Corne L, Ebinger G, Michotte Y, Huyghens L. Mild hypothermia induced by a helmet device: a clinical feasibility study. Resuscitation. 2001 Dec;51(3):275-81. 16. Kim F, Olsufka M, Longstreth WT, Jr., Maynard C, Carlbom D, Deem S, et al. Pilot randomized clinical trial of prehospital induction of mild hypothermia in out-of- hospital cardiac arrest patients with a rapid infusion of 4 degrees C normal saline. Circulation. 2007 Jun 19;115(24):3064-70. 17. Battin MR, Dezoete JA, Gunn TR, Gluckman PD, Gunn AJ. Neurodevelopmental outcome of infants treated with head cooling and mild hypothermia after perinatal asphyxia. Pediatrics. 2001 Mar;107(3):480-4. 18. Eicher DJ, Wagner CL, Katikaneni LP, Hulsey TC, Bass WT, Kaufman DA, et al. Moderate hypothermia in neonatal encephalopathy: efficacy outcomes. Pediatr Neurol. 2005 Jan;32(1):11-7. 19. Gunn AJ, Gluckman PD, Gunn TR. Selective head cooling in newborn infants after perinatal asphyxia: a safety study. Pediatrics. 1998 Oct;102(4 Pt 1):885-92. 20. Lin ZL, Yu HM, Lin J, Chen SQ, Liang ZQ, Zhang ZY. Mild hypothermia via selective head cooling as neuroprotective therapy in term neonates with perinatal asphyxia: an experience from a single neonatal intensive care unit. J Perinatol. 2006 Mar;26(3):180-4. 21. Robertson NJ, Nakakeeto M, Hagmann C, Cowan FM, Acolet D, Iwata O, et al. Therapeutic hypothermia for birth asphyxia in low-resource settings: a pilot randomised controlled trial. Lancet. 2008 Sep 6;372(9641):801-3. 22. Shankaran S, Laptook A, Wright LL, Ehrenkranz RA, Donovan EF, Fanaroff AA, et al. Whole-body hypothermia for neonatal encephalopathy: animal observations as a basis for a randomized, controlled pilot study in term infants. Pediatrics. 2002 Aug;110(2 Pt 1):377-85. 23. Shankaran S, Pappas A, Laptook AR, McDonald SA, Ehrenkranz RA, Tyson JE, et al. Outcomes of safety and effectiveness in a multicenter randomized, controlled trial of whole-body hypothermia for neonatal hypoxic-ischemic encephalopathy. Pediatrics. 2008 Oct;122(4):e791-8. 24. Zhou WH, Shao XM, Cao Y, al. E. Safety study of hypothermia for treatment of hypoxic-ischemic brain damage in term neonates. Acta Pharmacologica Sinica. 2002;23 (Supplement):64-8. 25. Adelson PD, Ragheb J, Kanev P, Brockmeyer D, Beers SR, Brown SD, et al. Phase II clinical trial of moderate hypothermia after severe traumatic brain injury in children. Neurosurgery. 2005 Apr;56(4):740-54; discussion -54. 26. Biswas AK, Bruce DA, Sklar FH, Bokovoy JL, Sommerauer JF. Treatment of acute traumatic brain injury in children with moderate hypothermia improves intracranial hypertension. Crit Care Med. 2002 Dec;30(12):2742-51. 27. Clifton GL, Allen S, Barrodale P, Plenger P, Berry J, Koch S, et al. A phase II study of moderate hypothermia in severe brain injury. J Neurotrauma. 1993 Fall;10(3):263-71; discussion 73. 28. Hutchison JS, Ward RE, Lacroix J, Hebert PC, Barnes MA, Bohn DJ, et al. Hypothermia therapy after traumatic brain injury in children. N Engl J Med. 2008 Jun 5;358(23):2447-56. 29. Jiang J, Yu M, Zhu C. Effect of long-term mild hypothermia therapy in patients with severe traumatic brain injury: 1-year follow-up review of 87 cases. J Neurosurg. 2000 Oct;93(4):546-9. 30. Liu WG, Qiu WS, Zhang Y, Wang WM, Lu F, Yang XF. Effects of selective brain cooling in patients with severe traumatic brain injury: a preliminary study. J Int Med Res. 2006 Jan-Feb;34(1):58-64. 31. Marion DW, Obrist WD, Carlier PM, Penrod LE, Darby JM. The use of moderate therapeutic hypothermia for patients with severe head injuries: a preliminary report. J Neurosurg. 1993 Sep;79(3):354-62. 32. Marion DW, Penrod LE, Kelsey SF, Obrist WD, Kochanek PM, Palmer AM, et al. Treatment of traumatic brain injury with moderate hypothermia. N Engl J Med. 1997 Feb 20;336(8):540-6. 33. Qiu WS, Liu WG, Shen H, Wang WM, Hang ZL, Zhang Y, et al. Therapeutic effect of mild hypothermia on severe traumatic head injury. Chin J Traumatol. 2005 Feb;8(1):27-32. 34. Shiozaki T, Sugimoto H, Taneda M, Yoshida H, Iwai A, Yoshioka T, et al. Effect of mild hypothermia on uncontrollable intracranial hypertension after severe head injury. J Neurosurg. 1993 Sep;79(3):363-8. 35. Shiozaki T, Kato A, Taneda M, Hayakata T, Hashiguchi N, Tanaka H, et al. Little benefit from mild hypothermia therapy for severely head injured patients with low intracranial pressure. J Neurosurg. 1999 Aug;91(2):185-91. 36. Shiozaki T, Hayakata T, Taneda M, Nakajima Y, Hashiguchi N, Fujimi S, et al. A multicenter prospective randomized controlled trial of the efficacy of mild hypothermia for severely head injured patients with low intracranial pressure. Mild Hypothermia Study Group in Japan. J Neurosurg. 2001 Jan;94(1):50-4. 37. Smrcka M, Vidlak M, Maca K, Smrcka V, Gal R. The influence of mild hypothermia on ICP, CPP and outcome in patients with primary and secondary brain injury. Acta Neurochir Suppl. 2005;95:273-5. 38. Wang WP, Ren HJ, Chi JY, Xu FL, Quan Y. Effects of mild hypothermia on patients with lower intracranial pressure following severe brain injury. Chin J Traumatol. 2005 Feb;8(1):54-6. 39. Zhi D, Zhang S, Lin X. Study on therapeutic mechanism and clinical effect of mild hypothermia in patients with severe head injury. Surg Neurol. 2003 May;59(5):381-5.