Options for the Use of Rapid Antigen Tests for COVID-19 JD
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Rapid Antigen Detection Test for Group a Streptococcus in Children with Pharyngitis (Review)
Cochrane Database of Systematic Reviews Rapid antigen detection test for group A streptococcus in children with pharyngitis (Review) Cohen JF, Bertille N, Cohen R, Chalumeau M Cohen JF, Bertille N, Cohen R, Chalumeau M. Rapid antigen detection test for group A streptococcus in children with pharyngitis. Cochrane Database of Systematic Reviews 2016, Issue 7. Art. No.: CD010502. DOI: 10.1002/14651858.CD010502.pub2. www.cochranelibrary.com Rapid antigen detection test for group A streptococcus in children with pharyngitis (Review) Copyright © 2016 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd. TABLE OF CONTENTS HEADER....................................... 1 ABSTRACT ...................................... 1 PLAINLANGUAGESUMMARY . 2 SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . ..... 3 BACKGROUND .................................... 5 OBJECTIVES ..................................... 7 METHODS ...................................... 7 RESULTS....................................... 10 Figure1. ..................................... 11 Figure2. ..................................... 12 Figure3. ..................................... 13 Figure4. ..................................... 15 Figure5. ..................................... 16 Figure6. ..................................... 18 Figure7. ..................................... 20 DISCUSSION ..................................... 21 AUTHORS’CONCLUSIONS . 23 ACKNOWLEDGEMENTS . 23 REFERENCES ..................................... 24 CHARACTERISTICSOFSTUDIES . 42 DATA ....................................... -

Diagnostic COVID-19 Testing Faqs
Diagnostic COVID-19 Testing FAQs Q: What testing is currently available to diagnose active COVID-19 infection? A: There are two types of COVID-19 tests available – a traditional PCR test that is sent to a lab and a Rapid Antigen Test that is run on site. Each test is performed by taking a swab from the nose to test for the presence of the SARS-CoV-2 (the virus causing COVID-19). Q: How long does it take to get results and how accurate are they? A: PCR Test: It takes approximately 3-5 days for a result to be returned from our lab and has a high degree of accuracy both for positives and negatives. Rapid Antigen Test: The advantage of this test is the ability to get a result while you wait, usually within 15 minutes. This test has a high accuracy rate for positive test results, but approximately an 85% accuracy rate for negative results. Q: What does a positive test result mean? A: A positive test for COVID-19 indicates active infection with the SARS-CoV-2 virus. Q: What does a negative test result mean? A: A negative test for COVID-19 means an individual was probably not infected at the time their sample was collected. However, that does not mean they will not get sick in the future. False negatives can also be possible, particularly with antigen testing. Q: If I choose a Rapid Antigen Test and my result is negative, what should I do? A: If you are suffering from symptoms or have been exposed to someone with COVID-19, you will need to have a PCR test to verify your negative test result. -

Rapid Review: Performance and Feasibility of Rapid COVID-19 Tests
COVID-19 Scientific Advisory Group Rapid Evidence Report Do the rapid COVID-19 tests on the market represent a feasible opportunity for Alberta? 1. What are the reported performance characteristics of the rapid COVID-19 tests that have been approved for commercial (diagnostic) use in Canada? 2. What are the optimal strategies for deployment of rapid testing, to improve either clinical care or outbreak control in health care and community settings? Context • It is unclear how the rapid (point-of-care) molecular and antigen tests for COVID-19 tests compare to each other. • Five point-of-care testing devices/systems have been approved for diagnostic use by Health Canada: 1) BD Veritor System for Rapid Detection of SARS-CoV-2 (Becton Dickinson and Company) 2) BKit Virus Finder COVID-19 (Hyris Ltd.) 3) ID NOW COVID-19 (Abbott Diagnostics Scarborough Inc.) 4) Panbio COVID-19 Ag Rapid Test Device (Abbott Rapid Diagnostics) 5) Xpert Xpress SARS-CoV-2 (Cepheid). • The federal government has committed to distributing the consumables for the Abbott ID NOW and PanBio testing kits to each Canadian jurisdiction, however, the strategy for deploying the rapid test kits will be the responsibility of the public health leaders in the provincial/territorial governments. • The implementation of rapid testing in other jurisdictions offers an opportunity to learn from their experiences in deploying rapid COVID-19 tests and avoid potential missteps. These implementation activities have included mass assessments, population-level testing to determine prevalence, returned traveler assessment, staff screening at long-term care facilities, and school testing. Key Messages from the Evidence Summary • The body of evidence for rapid testing platforms is poor – many of the studies are at high risk of bias. -
Idaho Interim Guidance on Use of Rapid Antigen Tests for COVID-19
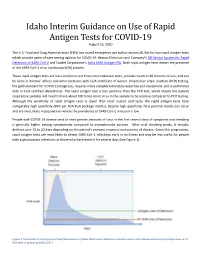
Idaho Interim Guidance on Use of Rapid Antigen Tests for COVID-19 Revised March 2021 The U.S. Food and Drug Administration (FDA) has issued emergency use authorizations (EUAs) for several rapid antigen tests, which greatly increase point-of-care testing options for COVID-19. Rapid antigen tests are less complex than most molecular tests and provide results in 30 minutes or less. As point of care diagnostics, they can be used in doctors’ offices and other facilities with a valid Clinical Laboratory Improvement Amendments (CLIA) Certificate of Waiver. Reverse transcription polymerase chain reaction (RT-PCR) testing, the gold-standard for COVID-19 diagnosis, is both highly sensitive and specific but requires more complex laboratory expertise and equipment and is not available as a point of care test. Rapid antigen tests are less sensitive than the RT-PCR test, which means that more viral particles must be present in the nose (or other approved sampling site) to generate the positive result. Lower sensitivity means that false negatives may occur more frequently, particularly very early or very late in the course of infection. All authorized rapid antigen tests have specificity similar to RT-PCR, which means that false positive results are expected to occur about as frequently as with an RT-PCR test. False positive results can occur and are most likely to occur in populations where the prevalence of SARS-CoV- 2 infection is low. People with COVID-19 disease tend to shed greater amounts of virus within the first five days of symptom onset. After viral shedding peaks, it steadily declines over 10 to 20 days depending on the patient’s immune response and the severity of disease. -

Performance Evaluation of Three Rapid Antigen Tests for the Diagnosis of Group a Streptococci
Open access Research BMJ Open: first published as 10.1136/bmjopen-2018-025438 on 5 August 2019. Downloaded from Performance evaluation of three rapid antigen tests for the diagnosis of group A Streptococci Ha-Nui Kim, Jeeyong Kim, Woong Sik Jang, Jeonghun Nam, Chae Seung Lim To cite: Kim H-N, Kim J, ABSTRACT Strengths and limitations of this study Jang WS, et al. Performance Objective To compare the diagnostic performance of evaluation of three rapid antigen three rapid antigen detection tests (RADTs) for group A tests for the diagnosis of group ► This study compared the diagnostic performance of Streptococcus (GAS). A Streptococci. BMJ Open three rapid antigen detection tests (RADTs) with two Design A hospital-based, cross-sectional, retrospective 2019;9:e025438. doi:10.1136/ references, the group A Streptococcus streptococcal study. bmjopen-2018-025438 pyrogenic exotoxin B (speB) gene PCR and culture Setting A comparative study of rapid diagnostic tests for methods. ► Prepublication history for GAS using clinical specimens in a single institute. ► The careUS Strep A Plus is a useful test that is highly this paper is available online. Participants 225 children in the outpatient clinics ofKorea comparable with the ‘reference standard’ test. To view these files please visit University Guro Hospitalwith suspicious symptoms were the journal online (http:// dx. doi. ► We used samples stored below −70°C in a 10 mL subjected to throat swab sampling. A dual-swab applicator org/10.1136/bmjopen-2018- transport tube containing 1 mL liquid Stuart’s trans- was used. Samples were stored at below −70°C in a 025438). -
COVID-19 TESTING Frequently Asked Questions
COVID-19 TESTING Frequently Asked Questions Who is eligible for COVID-19 testing at UR Medicine Urgent Care? Testing is now available for everyone – whether ill with COVID-19 symptoms or asymptomatic. For testing requested based on rapid positive results, exposure or symptoms, you may require further testing and additional costs may be incurred. What is a COVID-19 Rapid Antigen Test, and how does it differ from a PCR test? The antigen test, or rapid test, detects if a patient is currently infected with COVID-19. The PCR test is considered the “gold standard” in COVID-19 detection. This test confirms with higher accuracy if a patient currently has the virus.* Which type of test will I get? For patients without COVID-19 symptoms and not exposed to a COVID-19 positive individual, a rapid test will be administered. For individuals with COVID-19 symptoms, or have been exposed to a confirmed COVID-19 positive individual, a PCR test will be administered. How long does it take to get results from a COVID-19 test? The rapid test offers results in about 15 minutes during your visit. Typically, individuals receive PCR test results within 24 to 48 hours. However, this can be delayed due to high demand. How do I find out the results of the PCR test? The quickest way to find out your PCR test results is to sign up for MyChart atmychart.urmc.edu How much does a rapid test cost? Since the rapid test is not covered by insurance for asymptomatic, non-exposed patients, it is a self-pay service. -
Differences Between Types of COVID-19 Tests
FOR IMMEDIATE RELEASE Contact: Katherine Hoyer October 21, 2020 208-415-5108 Differences Between Types of COVID-19 Tests NORTH IDAHO – COVID-19 testing has come a long way since the beginning of the pandemic and with that may come some confusion on what test you should get, when to be tested, and how accurate are the tests. Below is a breakdown of the types of tests that are available. Molecular: also know as Diagnostic test, viral test, molecular test, nucleic acid amplification test (NAAT), RT-PCR test, LAMP test. Diagnoses active coronavirus infection. Antigen: Rapid diagnostic test (Some molecular tests are also rapid tests.) Diagnoses active coronavirus infection. Antigen tests are more likely to miss an active coronavirus infection compared to molecular tests. Your health care provider may order a molecular test if your antigen test shows a negative result, but you have symptoms of COVID-19. Antibody: Serological test, serology, blood test, serology test. This test shows if you’ve been infected by coronavirus in the past. In Idaho, public health districts are receiving the BinaxNOW Rapid Antigen Test kits produced by Abbott Diagnostics. Many pharmacies and private providers now offer antigen testing. An order from a provider is still needed just like with the PCR tests for the antigen tests. Antigen tests are intended for use in patients who are currently symptomatic. It is intended to detect a current COVID-19 infection and is highly effective at around 98% versus PCR testing which is 100%, when used correctly. BinaxNOW is a “same day” results test, meaning results will be available to practitioners in about 15 minutes. -
![PDF Pdf Icon[189K]](https://docslib.b-cdn.net/cover/5064/pdf-pdf-icon-189k-2635064.webp)
PDF Pdf Icon[189K]
Morbidity and Mortality Weekly Report COVID-19 Severity and COVID-19–Associated Deaths Among Hospitalized Patients with HIV Infection — Zambia, March–December 2020 Duncan Chanda, MBChB1; Peter A. Minchella, PhD2; Davies Kampamba, MPH1; Megumi Itoh, MD2; Jonas Z. Hines, MD2; Sombo Fwoloshi, MMed1; Mary Adetinuke Boyd, MD2; Kalongo Hamusonde, MSc2; Lameck Chirwa, MSc1; Kotey Nikoi1; Robert Chirwa1; Mpanji Siwingwa, MPH1; Suilanji Sivile, MMed1; Khozya D. Zyambo, MMed1; Aggrey Mweemba, MMed1; Nyuma Mbewe, MBChB1; Katongo H. Mutengo, MMed1; Kennedy Malama, MBChB1; Simon Agolory, MD2; Lloyd B. Mulenga, MD, PhD1 The effect of HIV infection on COVID-19 outcomes is unclear. reaction or rapid antigen test results for SARS-CoV-2, the Studies in South Africa (1) and the United Kingdom (2) found an virus that causes COVID-19. Patients with diagnosed probable independent association between HIV infection and COVID-19 cases had radiologic evidence suggestive of COVID-19 with mortality; however, other studies have not found an association acute respiratory symptoms. Treatment centers have specifically between poor COVID-19 outcomes and either HIV status among designated isolation and treatment units staffed by clinicians hospitalized patients (3–5) or HIV-associated factors such as CD4 and nurses trained in COVID-19 clinical management. All count, viral load, or type of antiretroviral therapy (ART) (6). The patients who received medical care for COVID-19 in these cen- effect of HIV infection on COVID-19 outcomes remains an ters during March–December 2020 and who provided verbal urgent question in sub-Saharan Africa, where many countries are consent to receive treatment were enrolled in the COVID-19 experiencing dual HIV and COVID-19 epidemics, and capacity clinical outcomes study. -

Performance of a Point-Of-Care Test for the Rapid Detection of SARS-Cov-2 Antigen
microorganisms Article Performance of a Point-of-Care Test for the Rapid Detection of SARS-CoV-2 Antigen Annabelle Strömer 1,†, Ruben Rose 1,†, Miriam Schäfer 2, Frieda Schön 2, Anna Vollersen 2 , Thomas Lorentz 2, Helmut Fickenscher 1 and Andi Krumbholz 1,2,* 1 Institute for Infection Medicine, Christian-Albrecht University and University Medical Center Schleswig-Holstein, Brunswiker Str. 4, 24105 Kiel, Germany; [email protected] (A.S.); [email protected] (R.R.); fi[email protected] (H.F.) 2 Labor Dr. Krause und Kollegen MVZ GmbH, Steenbeker Weg 23, 24106 Kiel, Germany; [email protected] (M.S.); [email protected] (F.S.); [email protected] (A.V.); [email protected] (T.L.) * Correspondence: [email protected]; Tel.: +49-431-22010131 † These first authors contributed equally. Abstract: The rapid detection of infections caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is necessary in the ongoing pandemic. Antigen-specific point-of-care tests (POCT) may be useful for this purpose. Here, such a POCT (SARS-CoV-2 NADAL® COVID-19 Ag) was compared to a laboratory-developed triplex real-time polymerase chain reaction (RT-PCR) designed for the detection of viral nucleoprotein gene and two control targets. This RT-PCR served as a reference to investigate POCT sensitivity by re-testing upper respiratory tract (URT) samples (n = 124) exhibiting different SARS-CoV-2 loads in terms of RT-PCR threshold cycle (Ct) values. The optical intensities of the antigen bands were compared to the Ct values of the RT-PCR. -

Flu Season Information
Staying healthy during flu season Influenza and respiratory syncytial virus (RSV) Multiple tests for optimal care In the United States, respiratory virus season usually begins in October and lasts through April, although regional variation does occur. During these months, a number of different viruses are responsible for respiratory disease. The most important of these are influenza and respiratory syncytial virus (RSV), but others such as parainfluenza, rhinovirus, adenovirus and human metapneumovirus can also cause significant disease. In general, these viruses cause a clinical syndrome termed “influenza-like illness” due to overlapping clinical signs and symptoms (fever, cough, headache, sore throat, runny nose, fatigue, possibly muscle aches). Clinical signs and symptoms of influenza-like illness vary by person, ranging from asymptomatic carriage to severe disease requiring hospitalization. These respiratory viruses are easily spread throughout the community and health care environment and contribute greatly to the morbidity and mortality of the population. As such, the laboratory plays a crucial role in facilitating an accurate diagnosis. In this regard, most laboratories rely upon so-called “rapid antigen tests” to diagnose the most common viruses – influenza and RSV. However, rapid antigen tests are unreliable (false negative test results can exceed 40 percent). False negative test results lead to adverse outcomes, including inappropriate use of antibacterial antibiotics, inability to institute proper infection control measures, and the spread of disease throughout health care facilities and the community. Beaumont Laboratory uses a FDA-approved nucleic acid amplification test (NAAT) to simultaneously detect and differentiate influenza A, influenza B and RSV from nasopharyngeal swab specimens. NAATs provide the most accurate test results with a false negative rate of 3 percent or less. -
Idaho Interim Guidance on Use of Rapid Antigen Tests for COVID-19 August 10, 2020
Idaho Interim Guidance on Use of Rapid Antigen Tests for COVID-19 August 10, 2020 The U.S. Food and Drug Administration (FDA) has issued emergency use authorizations (EUAs) for two rapid antigen tests which provide point-of-care testing options for COVID-19: Becton-Dickinson and Company’s BD Veritor System for Rapid Detection of SARS-CoV-2 and Quidel Corporation’s Sofia SARS Antigen FIA. Both rapid antigen tests detect the presence of the SARS-CoV-2 virus nucleocapsid (N) protein. These rapid antigen tests are less complex to use than most molecular tests, provide results in 30 minutes or less, and can be done in doctors’ offices and other locations with CLIA certificate of waiver. Polymerase chain reaction (PCR) testing, the gold-standard for COVID-19 diagnosis, requires more complex laboratory expertise and equipment, and is performed only in CLIA certified laboratories. The rapid antigen test is less sensitive than the PCR test, which means the patient respiratory samples will need to have about 100 times more virus in the sample to be positive compared to PCR testing. Although the sensitivity of rapid antigen tests is lower than most nucleic acid tests, the rapid antigen tests have comparably high specificity (99% per FDA-EUA package inserts). Despite high specificity, false positive results can occur and are most likely in populations where the prevalence of SARS-CoV-2 infection is low. People with COVID-19 disease tend to shed greater amounts of virus in the first several days of symptoms and shedding is generally higher among symptomatic compared to asymptomatic persons. -

INDICAID COVID-19 Rapid Antigen Test
FACT SHEET FOR PATIENTS Coronavirus PHASE Scientific International, Ltd. July 28, 2021 Disease 2019 INDICAID™ COVID-19 Rapid Antigen Test (COVID-19) You are being given this Fact Sheet because your in direct anterior nasal swabs. The presence of viral sample(s) was tested for the Coronavirus Disease 2019 proteins indicate you may have been infected with the (COVID-19) using the INDICAID™ COVID-19 Rapid virus and are likely to be contagious. Antigen Test. Why was my sample tested? This Fact Sheet contains information to help you You were tested because your healthcare provider understand the risks and benefits of using this test for believes you may have been exposed to the virus that the diagnosis of COVID-19. After reading this Fact causes COVID-19 based on your signs and symptoms Sheet, if you have questions or would like to discuss the (e.g., fever, cough, difficulty breathing), and you are information provided, please talk to your healthcare within the first five (5) days of symptom onset. provider. What are the known and potential risks and benefits of the test? For the most up to date information on COVID-19 Potential risks include: • please visit the CDC Coronavirus Disease 2019 Possible discomfort or other complications that can happen during sample collection. (COVID-19) webpage: • Possible incorrect test result (see below for more https://www.cdc.gov/COVID19 information). Potential benefits include: What is COVID-19? • The results, along with other information, can help COVID-19 is caused by the SARS-CoV-2 virus which is your healthcare provider make informed a new virus in humans causing a contagious respiratory recommendations about your care.