Fundamentals 11-12 Scribe: Jake Nolen Monday, November 23, 2009 Proof: Hillary Carney Dr. Bartlett How Drugs are Prescribed Page 1 of 8 I. Introduction [S1]: a. We’re going to go through the FDA and some of the regulatory issues. b. We’re going to talk about prescription writing as well, so there should be a lot of practical utility from the lecture today. c. Call him with questions. II. New Drug Development and Regulatory Issues [S2] a. Some of the regulatory issues we’re going to talk about: b. This involves all of us as healthcare providers. We encounter these kinds of issues all the time. c. We’ll talk about new drug development- labeled and unlabeled uses. That’s a very impt medical-legal concept. d. We’ll talk about drug use during pregnancy and also controlled substances. e. We’ll talk about the drugs that have potential for abuse and addiction and how those are regulated f. We’ll talk about some practical issues, and give you some trade names of medications you’ll be encountering later in your career at UAB. III. How are Drugs Classified in the US? [S3] a. Let’s look at how drugs are classified first of all. b. There are two broad categories of drugs- over the counter drugs, drugs that are available without prescription. They are regulated by the FDA. On the other hand we have the legend drugs. These are the prescription drugs. They’re referred to as legend drugs because if you look at the label, the legend says caution: federal law prohibits distributing without prescription. c. That simply means that these are regulated. You have to have a prescription in order to use them or administer them or dispense them to a patient.
IV. Drugs Commercially available in the US [S4] a. 2 broad categories of drugs- over the counter and prescription. b. 2 kinds of prescription medications- non-controlled substances that are FDA regulated just like the over the counter products. We have the drugs that have potential for abuse and addiction. Those are called controlled substances. Controlled substances are those that have potential for abuse or addiction and those are regulated by the Drug Enforcement Administration (DEA). c. Those are the people that wear the baseball hats and do the drug raids. d. We’ll talk about the DEA and how those drugs are regulated in a few minutes.
V. New Drug Development [S5] a. Let’s look at new drug development. b. Whether these drugs are OTC (over the counter) or Rx (prescription), they go through a process to become available to our patients c. It’s a very long pathway to go from an idea or concept at the pre-clinical level and go all the way through the FDA and onto the patient care arenas. d. We have so called pre-clinical investigations. This would be lab or animal investigations. This investigation will reach a point where it looks fairly feasible that it could have use for us in clinical practice. e. At that point the IND application is submitted (Investigational New Drug) for approval to begin to do clinical investigation. f. This marks the point where, it’s a 30 day turn-around, they will tell you you can start human clinical studies on your product. g. At that point the drug sponsor and manufacturer are permitted to do interstate commerce – move these drugs across state lines and begin human testing which involves 3 phases: 1, 2, and 3. h. Phase 1 studies are very early studies looking at safety only. The impt question that must be answered is: Is this a safe medication? They take normal people without disease and they administer the drug. They look at pharmicokinetic issues, they look at drug metabolism and elimination: kidney function, liver enzymes. i. They’re making sure that the medicine seems to be safe. j. If it is, they move into phase 2 studies. This will be the first time the drug has actually been used in people with the disease to treat them. If it’s an antibiotic, is it going to be useful on this infection? If it’s a glaucoma product, is it going to be used successfully? So patients with glaucoma are recruited for the phase 2 study looking at safety and efficacy. k. Phase 3 pivotal studies are large scale drugs to look at safety and efficacy before the product is finally submitted to the FDA for approval. That application is called the NDA (new drug application). That’s submitted to the FDA. Once it’s approved, not every drug is approved, but once it’s approved, then some drugs will go into phase 4. That’s post-marketing testing. There may be some clinical questions, some clinical safety issues that need to be looked at in more detail, so the FDA may either request or require the company to launce some phase 4 studies even after the product is on the market. Fundamentals 11-12 Scribe: Jake Nolen Monday, November 23, 2009 Proof: Hillary Carney Dr. Bartlett How Drugs are Prescribed Page 2 of 8 l. The drug can be launched, it can be made available to the public, but phase 4 testing can be ongoing for a number of years to answer some of these questions that came up in the initial investigations. m. It takes a while to get all this through the FDA
VI. Newspaper article [S6] a. The question sometimes comes up: Why should we be interested? b. Why do we need to know phase 1, phase 2, phase 3? It’s because patients care. c. Patients can read the newspaper. In fact here’s an article from the wall street journal talking about a miracle obesity pill. They talk about 3 companies that are developing obesity pills, and they talk about the Pfizer product and the Merck product, and they actually have in the newspaper Phase 3 trials, phase 3 trials, completed phase 2 trials for the Alazeim product in the UK. Knowing where a drug is in the development can be of interest to our patients. d. They want to know: When will I have access to this new drug for my condition? e. If you know a product has finished phase 3 and it’s about to be submitted to the FDA, it should be a year-a year and a half before it’s on the market. We’ll look at a timeline in a minute.
VII. Newspaper article [S7] a. Lots of clinical trials going on, particularly here at UAB. You can pick up a newspaper and read online to see the many clinical human studies that are ongoing here. This is a lead article. The headline in the Sunday newspaper was the car at Bristol, but this is the real headline they were trying to emphasize about UAB clinical trials. b. We have lots of trial going on at phase 1, 2, and 3 levels here at UAB. Lots of phase 2 and 3 studies are ongoing.
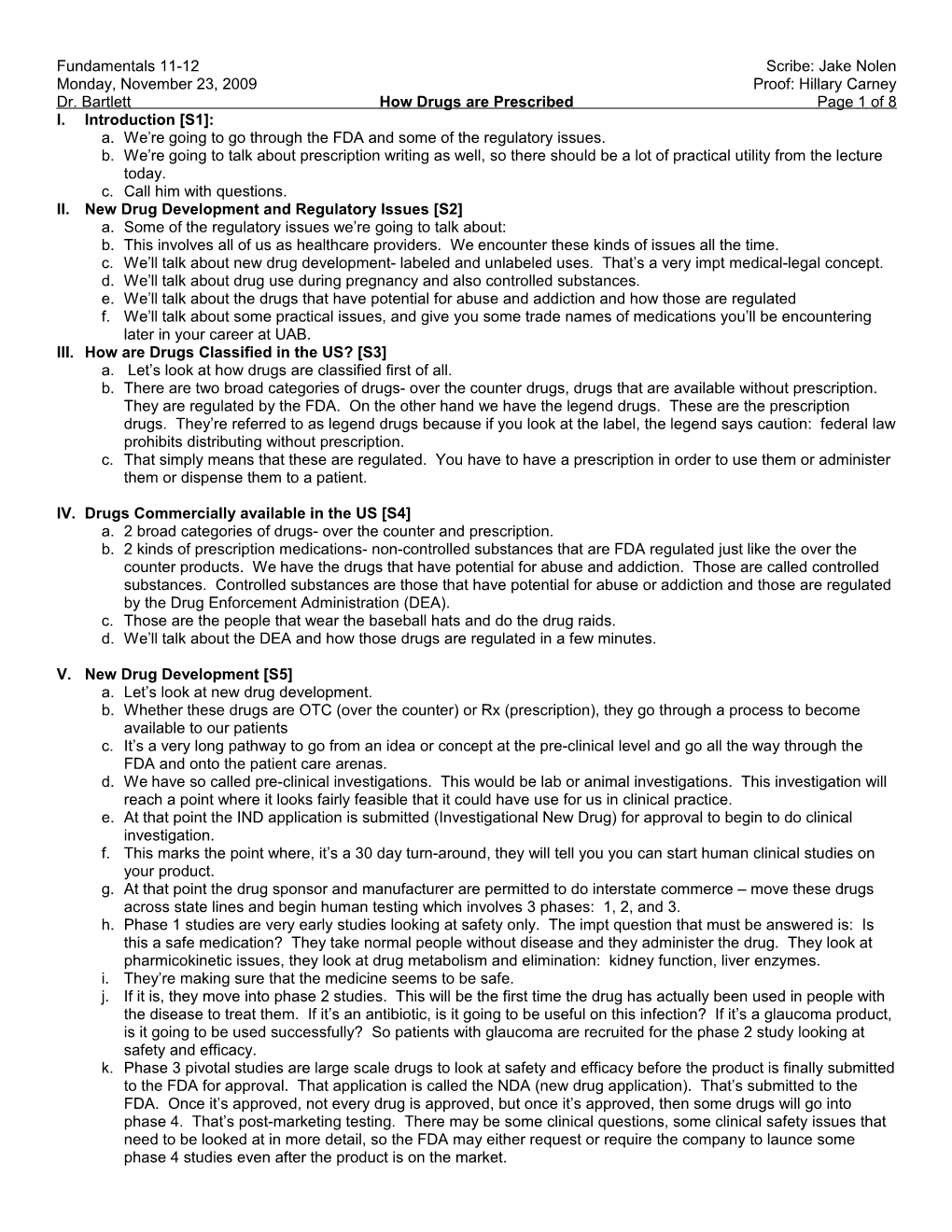
VIII. Drug Approval Timeline [S8] a. This is right out of your textbook b. This simply shows us the timeline for drug approval. c. We have the first couple of years in the lifeline of a brand new drug are the in vitro lab testing on animals and that kind of thing. d. At about the 4 year mark, the IND is submitted permitting the phase 1 testing to start. e. Phase 1: is it safe?, Phase 2: does it work?, Phase 3: does it work and is it also safe? In a double blind, mass scale kind of study. The NDA is submitted and years 8 and 9 here simply suggest that it takes about a year or two for drugs to undergo their evaluation at the FDA before they’re actually approved. f. Once the NDA is submitted to the FDA, it takes a year or two ( the average is 1 yr) for a drug to be approved by the FDA. g. Phase 4 studies can be ongoing at that point. Notice the patent will expire after 20 yrs, but 20 yrs. From what? It’s not 20 yrs from the time the FDA approves the drug. The FDA has nothing to do with patents. Patents are issued way back at the in vitro or animal testing phase. Sometimes several years before human testing actually starts. h. The clock starts to tick when the patent is issued in the animal stage or lab phase. It can be early in human testing, but usually it’s back here 20 yrs from that point not 20 yrs from the time the FDA approves it. i. Sometimes by the time the FDA gets around to approving a product the patent may expire in 6 or 8 or 10 yrs. j. Obviously, the company wants the longest patent as possible to protect its investment in the research.
IX. Standard NDA and BLA approvals [S9] a. This busy graph simply shows us that for a standard NDA, there are 2 tracks that an NDA can take at the FDA. b. Most drugs are on the standard track where the normal evaluation processes take place. The other is called a priority track. If a new drug has potentially novel advances, the drug manufacturer may pay the FDA for additional reviewers to get it through the FDA track quicker. c. There is a priority track and a standard track. The standard track graph simply shows us- these bars here indicate the time at the FDA. d. The average time for a standard review from the FDA is 12 months. He emphasized this. e. On average, it takes one year to get a product through the FDA once the NDA has been submitted. If you read the newspaper tonight or see online that an NDA is submitted, chances are in a year we should see that drug approved and on the market and available for our patients.
X. Drugs with Unlabeled Uses [S10] a. Let’s look at a different topic here: drugs with unlabeled uses. b. It’s a very important medical-legal term. It can come back to haunt you if you’re not careful as a clinician. Fundamentals 11-12 Scribe: Jake Nolen Monday, November 23, 2009 Proof: Hillary Carney Dr. Bartlett How Drugs are Prescribed Page 3 of 8 c. This means we’re taking a drug that the FDA has approved, and we’re using it in an unapproved manner. We’re using it in a way that is not suggested by the package insert. d. The label is the package insert. Off label means you’re using the drug for a condition or disease that’s not in the package insert. e. Or a dosing frequency or duration that’s not in the package insert. So you’re departing from the recommendations that have been approved in the package insert. f. The term is unlabeled or off-label, and it’s an important concept. XI. What is the Label? [S11] a. It’s the package insert b. XII. Information Provided in the Package Insert [S12] a. I would encourage you to pick up a package insert and read it, so you can see the kind of info that is there. It’s very impt info. b. It is a legal document- it’s admissible in a court of law as the rule to follow for a drug approved by the FDA. c. The plaintiff’s attorney uses them a lot to prove that a doctor has committed malpractice by not following the directions in the package insert. XIII.Information Provided in the Package Insert [S13] a. Lots of different things on there indications, contra-indications, precautions, adverse events, drug interactions.
XIV. Prozac [S14] a. Here’s an example of a drug you all know. b. This is a package insert label for Prozac. c. What would you call the big black box label? The black box warning. d. It’s the first thing you see in some package insert. Pay attention to the black box warning if you’re using a drug or prescribing it to a patient. You need to be very familiar with the content. e. In this case, it’s talking about with Prozac, and similar anti-depressants in children and adolescents, there is know suicidality involved there. Kids can develop suicidal tendencies when on this kind of anti-depressants. f. XV. Examples of Unlabeled Uses [S15] a. Here’s an example of unlabeled uses b. We’ve got Cytotec, trade name for Misoprostol which is a prostaglandin analog. c. It’s labeled and approved by the FDA to prevent NSAID (non-steroidal anti-inflammatory drugs like ibuprofen) induced gastric ulcers. They can tear down the stomach lining, and this product is designed to replenish the prostaglandins to maintain the stomach lining. This decreases gastric ulcer problems with long-term NSAID use. d. An unlabeled use: obstetricians use it to induce labor. A completely different indication but it’s a very effective medication to induce labor. e. Valium’s labeled use is a muscle relaxant medication, but it’s great for panic attacks. f. Quinine, you can see chloroquinone resistant malaria that’s the approved FDA use, but it can be used unlabeled for nocturnal leg cramps. Quinine can be very effective for nighttime leg cramps. g. You have approved indications and unapproved uses that become common in practice.
XVI. Unlabeled Uses are Legal [S16] a. It is legal to use medication for off-label purpose even though we talk about medical-legal consequences, it is legal to use medicines off label, but there need to be some caveats. b. One is, does it make sense scientifically or medically. Can you explain the pharmacological mechanism in terms of how the drug is acting. It needs to make sense. There must be an explainable mechanism of action. c. Second, is there peer-reviewed literature to support your use of the medication in this fashion. Must be good, published, solid science behind it. Not an editorial in a throw away magazine, but a good article in a peer reviewed magazine like the New England Journal of Medicine. That kind of quality where you have a placebo controlled and comparison group, doubled massed, scientifically validated study. That’s very helpful to have that going for you. d. Third, do you have the patient’s informed consent? That’s a very impt term that you’ll learn about. It’s a very important medical-legal concept. Have you told the patient you’re using a medication for them that the FDA has not approved but nevertheless has been found to be effective, and do you have the patients consent to go ahead and be treated that way? You write that down on the chart. e. If these three things apply, you’re on solid footing for using a medication off label. Sometimes, you could get a phone call from a pharmacist refusing to fill that prescription if they know you’re using it off label. If you get a call like that, be prepared to defend yourself and quote and send that literature that’s been published, and make Fundamentals 11-12 Scribe: Jake Nolen Monday, November 23, 2009 Proof: Hillary Carney Dr. Bartlett How Drugs are Prescribed Page 4 of 8 sure you can rationalize from a scientific or pharmacological point of view the mechanism of action that you’re utilizing here for this off label use.
XVII. Negative Consequences of Unlabeled Uses [S17] a. Negative consequences medical-legal and insurance.
XVIII. Newspaper Article [S18] a. This is an article also from the Wall Street Journal about a drug company called Cephalon. They have a drug called Fentora. It’s Fentanil-- it’s a narcotic analgesic approved for acute cancer pain. b. Rather than acute cancer pain, some doctors have been using this medication for migraine headaches. c. Some patients have died when receiving Fentora for migraine headaches. d. Now you have a situation where doctors use a medication off-label with adverse consequences. e. You can understand the medical legal issues that arise when these doctors are sued for medical malpractice. f. When using medications off label and there are serious side effects, it’s very difficult to defend yourself unless you fall back on the 3 caveats that we mentioned.
XIX. As Costs Rise . . . [S19] a. Another consequence is insurance denial of payment. Here’s an example of Avastin. Approved for colorectal cancer and doctors are using it for brain tumors. It’s an ulabeled use of Avastin. They submit the insurance claims and they don’t pay it because it’s an unlabeled use of the drug. The drug costs $8000 per dose every 2 weeks. We’re talking about a $300,000 a year drug where insurance claims are being denied. b. That’s one consequence of using drugs off label. You have to think about insurance problems, malpractice problems.
XX. Drugs in Pregnancy [S20] a. How about drugs in pregnancy? b. The number one rule is don’t use drugs during pregnancy. Medications may not be safe. c. We can’t do controlled clinical trials during pregnancies d. We can do animal trials. They look at birth defect potential in animals during pregnancy during the animal phase of testing. We know about mechanisms of action. We know how safe drugs should be based on that. e. We know about clinical experience, reportable problems during pregnancy. f. Based on those kinds of things, the FDA has given every drug product a rating classification based on potential risks, perceived risks to the fetus during pregnancy.
XXI. 19 yowf Presents for Second Opinion [S21] a. Here’s a picture of a 19 year old patient brought in by her mother. b. She’s 4 months pregnant.
XXII. Picture of Eye [S22] a. If we look at her left cornea, anyone can see this is not a healthy cornea. There are blood vessels growing in, the cornea is hazy when it should be clear. b. This is a patient that has a very severe form of allergy called atopic keratoconjuncitivitis. c. She needs steroids, a strong anti-inflammatory approach to treatment. d. She had been on a steroid eye drop 4 times a day for the past year. A frequent course of steroids like that can cause a lot of harm. Elevating intraocular pressure, causing cataract. Fortunately she didn’t have any of those problems, but the mother was worried because now that she’s 4 months pregnant, should she be using this cortisone eye drop during her pregnancy?
XXIII. FDA Pregnancy Categories [S23] a. If we look at these ratings, we have A, B, C, D, and X b. Which is the worst? X! c. If that’s on the test, you’ll get it right d. Absolutely avoid category X medicines. They are well known to cause birth defects. e. A is the safest. A drug in the A category is presumed to be safe. I’ll give examples in a minute. f. Then you have all these in between. Generally from a clinical point of view, category A and B drugs seen to be safe. We can prescribe a lot of drugs in category B safely during pregnancy. g. You really want to avoid category C drugs. For each individual patients you have to weigh the advantages and the disadvantages. Balance out advantages with risks. Fundamentals 11-12 Scribe: Jake Nolen Monday, November 23, 2009 Proof: Hillary Carney Dr. Bartlett How Drugs are Prescribed Page 5 of 8 h. Individual judgment with every patient. Try not to use any drugs during pregnancy, but some you have to treat. i. You have to treat hypertension during pregnancy. You have to treat thyroid disease and diabetes and lots of things that are chronic. j. Avoid category D drugs during pregnancy. They have known risks.
XXIV. Drug Use During Pregnancy [S24] a. Here’s a little summary table showing us the implications of these categories b. A is no risk, B is no evidence of risk, C risk can’t be ruled out, D there is risk. X is a definite risk. c. There are some examples on the right that are commonly used. Levothyroxin is one that is commonly used. The trade name for that is synthroid which is used for hypothyroidism. d. Vitamin B6 is very safe. 25 mg of B6 is great for morning sickness in pregnancy, so that’s category A e. Azithromycin antibiotic, erythromycin antibiotic, rimantidine for glaucoma. f. Some category 3 drugs are steroids. All steroids whether topically delivered or given intravenously or nasal steroids are all category C. We would rather avoid category 3. g. In the patient I just showed you, I switched her to a category B medicine for use during pregnancy. h. Tetracycline antibiotics, you’ll get that later, these are definitely something that can create problems with bone development, tooth discoloration. i. The trade name for isotretinoin is Acutane. Category X
XXV. Avoid Category X ! [S25] a. Acutane in category X and is a very serious risk for birth defects. It’s taken for acne.
XXVI. Caveats [S26] a. There are some caveats. Some drugs have more than one category depending on the trimester. b. In the first trimester, the ACE inhibitors for example, for blood pressure are category C but in the second and third trimester, they’re a D. The risk increases as the pregnancy goes on. Some drugs like ibuprofen which is OTC, is category B. However, there are risks of congenital heart defects with ibuprofen. The FDA has a pregnancy labeling task force to see if they can come out with anything more meaningful or more effective to get this info across. c. Currently, we have these ABCDX ratings that you’ll need to know and use all the time during clinics when you have a woman who is pregnant or may become pregnant. Think about these things before you prescribe drugs.
XXVII. Controlled Substances [S27] a. Let’s look at the controlled substances b. Again these drugs have potential for abuse and addiction c. They have a separate regulatory oversight. They are regulated by the Drug Enforcement Administration (DEA) d. When we finish here at UAB and get our license, we still can’t use the controlled substances until we register with the DEA. That’s a separate registration process. You must register directly with the DEA as a provider with an online application and renew it every three years. If you dispense medicines in more than one office, you have to register for each office. The current cost is $551 every 3 years. They’re raised it recently to fight the drug wars.
XXVIII. Controlled Substance Schedules [S28] a. The controlled drugs have 5 schedules. Some people call them classes but they’re officially known as schedules. b. They’re given roman numerals. The lower the roman numeral, the greater the risk for addiction or abuse. c. There are I, II, III, IV, and V. I has the greatest addiction and abuse potential. It’s so great that there is no accepted medical use. No provider can use or prescribe Schedule I use. d. The drugs that have the highest addiction and abuse potential that we can prescribe are schedule II. e. Schedule III is less risk, IV is less, and V have such little potential for abuse and addiction that they can be sold OTC w/o prescription. Many states have upregulated those from schedule V to schedule III. State law trumps federal law with regards to controlled drugs. f. A good example is Codein which used to be available otc as a cough syrup. Now, it’s schedule III and requires a prescription in just about every single state.
XXIX. Symbol Designation [S29] a. There’s a symbol you want to look for to designate a controlled substance: a capital C and a Roman Numeral b. It’s a roman numeral with a C around it, so this one is schedule II and has a high addiction potential. c. The other one is Schedule III. Schedule III has lower abuse potential. Fundamentals 11-12 Scribe: Jake Nolen Monday, November 23, 2009 Proof: Hillary Carney Dr. Bartlett How Drugs are Prescribed Page 6 of 8
XXX. Examples [S30] a. These are some examples here of schedule I, so no one can use those. LSD and marijuana are examples of that. b. Schedule II drugs include cocaine which we use in optometry professionally and maybe dentistry too as a local anaesthetic. It’s used in ENT surgeries as an anesthetic and in optometry to diagnose Horner’s syndrome. c. We have morphine and oxycodone (oxycontin) that are schedule II. d. Schedule III’s- codeine, combinations with aspirin or ibuprofen and acetaminophen. Lots of combos there containing codeine, hydrocodone, like Lortab for example. That’s hydrocodone. e. Lots of different commercial combinations there. f. Schedule IV prophoxyphene (that’s our Darvon, darvoced N type medicine), butorphanol, midazolam g. Schedule V like Robitussin AC. OTC codeine permitted federally, but at the state level that’s usually a prescription schedule III in most states including AL. h. When you have a few minutes, go to this website. It’ll give you all of the schedules. Every drug and every schedule. There are 100’s of drugs available commercially and you can see them all there on that website.
XXXI. Requirements for Schedule II [S31] a. There are some regulatory aspects we need to pay attention to as we write prescriptions. b. Schedule II drugs must be written prescription- you can’t call them in. c. You can call in for schedules III and IV but not schedule II. d. They must be handwritten and signed and have limited doses. They usually like to see less than 100 doses. e. They can’t be refilled.
XXXII. Requirements for Schedules III and IV [S32] a. For schedules III and IV, you can call them in. b. They can be refilled up to 5 times in 6 months. Generally, there are some restrictions for optometrists that they’ll talk about in optometric pharmacology, but generally there are no dose limitations. c. XXXIII. Schedule V [S33] a. Schedule V we talked about OTC or legend depending on the state.
XXXIV. Precautions in Prescribing Controlled Drugs [S34] a. Some good websites here. Drugs @ FDA I use at least once a week. Can see the package inserts for most medications there. b. The orange book. For years, it had an orange color. Now, it’s online with an orange background. This is the primary source for generic info, so if you’re trying to find out if a drug has a generic form, and it’s equivalent to the trade name, this is where you find that info. Drugs are rated there A, AB, B, AT. The A rated products are therapeutically equivalent. AT are therapeutically equivalent too. c. DEA is for our controlled drugs. d. ePocrates is something you should be using by tomorrow. Free, highly credible, downloadable drug database. Over 900,000 physicians in the US use this. It tells you everything about a drug. e. XXXV. Useful Websites [S35] a. Let’s look at prescription writing.
XXXVI. Prescription Writing [S36] a. Obviously, it’s a communication between the prescriber and the pharmacist. b. Indirectly, it’s a communication to the patient too. Basically we want to be sure the pharmacist fully understands exactly what our instructions will be to the patient.
XXXVII.What Is a Prescription? [S37] a. This is what I call the pharmicotherapeutic chain. Preclinical drug development, clinical trials, FDA approval. Here’s the practitioner, the pharmacist, and our patient. We’re communicating to the pharmacist for the benefit of our patient. b. If we have poor communication, then our patient can be harmed. Many patients have died through inappropriate communication to the pharmacist. c. XXXVIII. Types of Prescriptions [S38] a. Usually we write prescriptions Fundamentals 11-12 Scribe: Jake Nolen Monday, November 23, 2009 Proof: Hillary Carney Dr. Bartlett How Drugs are Prescribed Page 7 of 8 b. Sometimes we can call them in c. You can also use electronic prescribing. E-prescribing is coming into its own and will be a requirement in the next couple of years. Most of the clinics here on campus are converting to e-prescribing. XXXIX. Electronic Transmission “e-Prescribing” (S39) a. The advantages are many with e prescribing b. Fixes the problem of bad handwriting. Poor handwriting has gotten a lot of people in trouble when pharmacists can’t read the prescription. c. You have pre populated fields. You can just click on the dosage. There are lots of advantages with this.
XL. The Prescription Pad (S40) a. Here’s a well done prescription, and it proves a point. When you’re in a multi-doctor practice, you need to circle your name. The pharmacist needs to know who wrote the prescription so he can call the prescribing doctor if there is a question. Be sure you have definitive identification of who you are as a prescriber.
XLI. Prevent Forgeries (S41) a. There are prescription pads now to prevent forgeries. There is a requirement now that prescriptions for Medicaid patients have at least 3 tamper proof features on the Rx pad to eliminate forgery and drug diversion. b. One way is when you photocopy the Rx it leaves a void across the whole paper. Or if you try to erase it, the erasures are very easy to see. XLII. RX against fraud (S42) a. This is one from UAB hospital showing the void on the back when it’s copied. We’ll use these kind of Rx pads when we get to the clinics. XLIII. Format of the Written Prescription (43) a. Let’s look at the format here. Basically, we’re looking at the center here. We have the superscription, that just the symbol “Rx”. It’s an ancient latin derivative. The 1st line of the prescription. b. There are 3 lines to a well written prescription. We’re talking about out-patient prescriptions. c. The top line is the name of the medication generic or trade name. d. With combination medications like lortab- acetominophen and hydrocodone combination. It’s easier to write out the trade name. Then, sign on the line to permit a generic. It’s faster for us this way. e. We have the strength of this product also written on the top line. f. The third is the formulation, so up to 3 things on that top line: the drug name, the strength, and the formulation if it comes in multiple formulations like a drop, suspension, ointment, etc. g. That’s called the inscription- the top line. h. The middle line is called the subscription. That’s the amount to be dispensed by the pharmacist at that time. 10 mLs or 50 capsules etc. Usually we’re limited by insurance rules to no more than 30 days supply. For chronic conditions- high B.P., diabetes, glaucoma, you do 30 days at a time. i. The third line is called the signatura which is latin for label. This is the part that will be typed on the outside of the container or bottle to instruct the patient how to use the medication. Must be very clear and unambiguous. It’s historically been written in Latin, but today we are using English more and more. When in doubt, write it in English and make sure it’s readable. j. One drop in each eye bid=twice a day for glaucoma. Put the reason for the Rx there in that third line. Some Rx pads have a blank for the reason. It’s impt for the pharmacist to know the reason, so he can double check your dosages. And that way they know if it’s on label or off label.
XLIV. Dispense as Written? (S44) a. Then we have two signature lines. Dispense as written means they must use the trade name drug. b. Product selection permitted allows them to get a generic. c. If you want the patient to get the benefit of the generic, sign on the right side d. In the state of Alabama, you must by law have two prescription lines on every prescription. One for trade name and one for generic. You can write a legal prescription on something other than a Rx pad, but it still must have two prescription lines for generic or trade name. Some insurance policies require you to prescribe generics.
XLV. Example for Oral Medication (S45) a. There’s a tetracycline like medicine called doxycycline. Pregnancy category D. b. We have second line: 60 of them c. Signatura: take one capsule by mouth. It’s impt to put “PO” on medicines that are orally administered. It’s latin for per os or by mouth. You’d be surprised what patients do with medicines. Women have eaten vaginal suppositories. Contraceptive jelly on toast has happened. XLVI. Quick Handheld Resources (S46) Fundamentals 11-12 Scribe: Jake Nolen Monday, November 23, 2009 Proof: Hillary Carney Dr. Bartlett How Drugs are Prescribed Page 8 of 8 a. skipped XLVII. Tips and Pearls (S47) a. skipped XLVIII. Write Legibly! (S48) a. This is an actual prescription for the Kirklin Clinic for a patient with high B.P. It’s illegible. Don’t do this.
XLIX. Avoid Abbreviations and Decimals (S49) a. Use latin abbreviations that are proper b. Avoid trailing zeros. Don’t put zeros behind a whole number. Don’t use decimals. Instead of giving 1.0, they may give 10. c. Don’t abbreviate drug names. Avoid decimals altogether if you can. If you have to use one, put a zero in front of it. 0.X L. Abbrevs (S50) a. These are the important latin abbreviations you need to know LI. More Abbrevs (S51) a. Learn the ones you don’t know LII. More Abbrevs (S52) a. Learn the ones you don’t know. When in doubt use English. LIII.The Institute for Safe Medication Practices (ISMP) (S53) a. This is a great website looking at the potential to miscommunicate when calling in prescriptions. LIV. Drug Name/Packaging Similarities Leading to Death (S54) a. Chlorpropamide and chlorpromazine look alike. This has led to death. b. Get the pharmacist to read back the Rx to you after you give it to him if you call in a Rx LV. Eliminating Error-prone Abbreviations, Symbols, and Dose Designations (S55) a. skipped LVI. The Problem (S56) a. skipped LVII. Implement “Do Not Use” List (S57) a. skipped LVIII. Blank (S58) a. skipped LIX. Include Reason for Prescription (S59) a. include the reason for the prescription. This is a Rx pad at university hospital. The pharmacist wants to know why the medication is being prescribed so they can double check the Rx. LX. Avoid “PRN” or “UT DICT” (S60) a. Avoid prn or UT DICT. PRN means as needed. UT Dict means as directed. A lot of patients don’t remember what you’ve told them. b. If you use PRN, put something after the prescription i.e. PRN pain, or sleep, or nausea etc. LXI. Example of Bad Prescription (S61) a. Here’s an example of a bad prescription. Never write more than 1 drug per prescription blank. LXII. Perscription (S62) a. If you want to do that, you can have a special Rx that you can put up to 3 medications on, so it’s very clear. LXIII. Prescription Writing for Opioids (S63) a. For opioids, you want to write the patient’s full address. It’s a federal, legal requirement for controlled drugs. LXIV. Rx Example for Controlled Substance (S64) a. This is a prescription for Lortab. Notice the #16. Put parentheses and spell out the number so the patient can’t add zeros and get 160. LXV. Perscription (S65) a. Take one tablet by mouth every 4-6 hrs as needed for eye pain. LXVI. Reread Your Prescription for Accuracy! (S66) a. Make sure your Rx says exactly what you want before you give it to your patient.
[end 48 min]