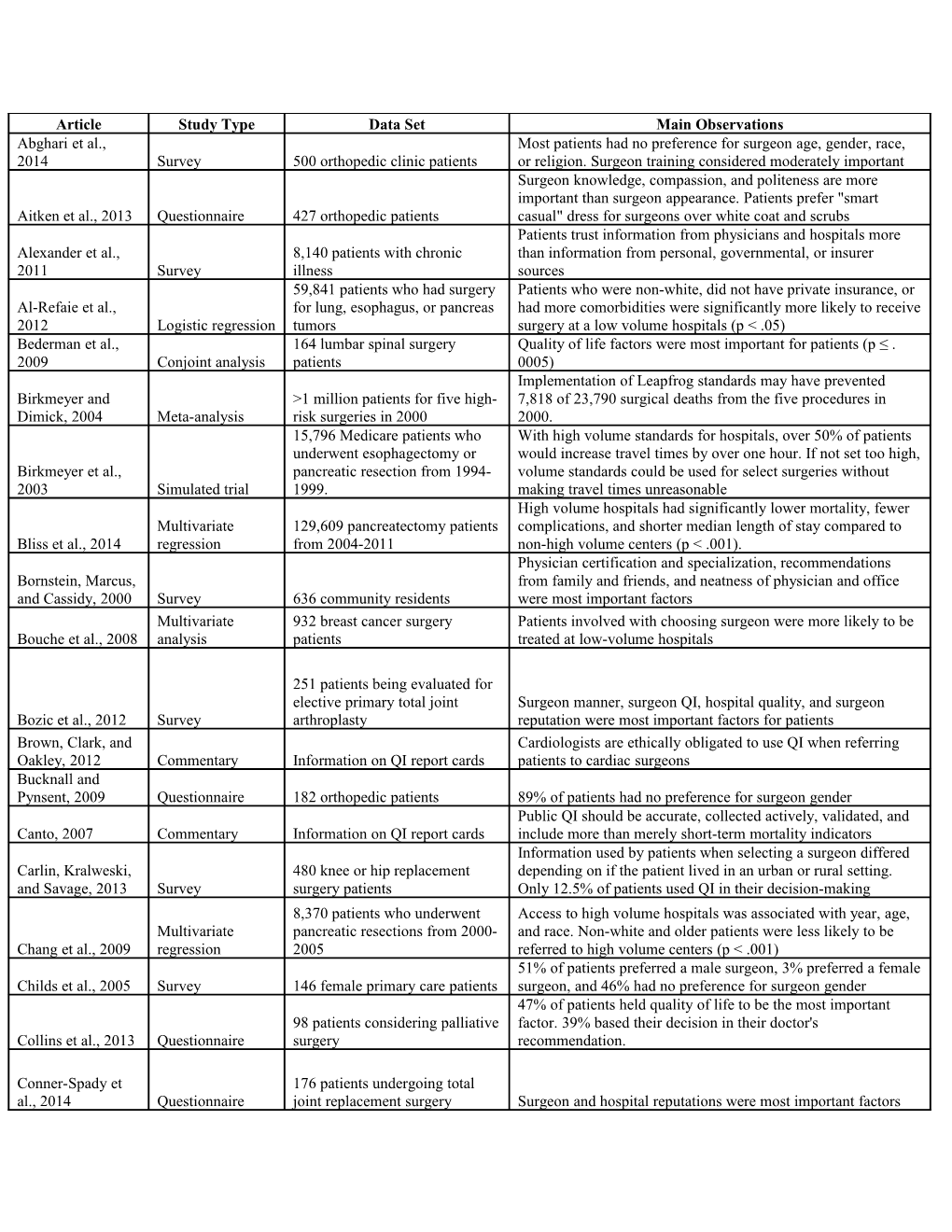
Article Study Type Data Set Main Observations Abghari et al., Most patients had no preference for surgeon age, gender, race, 2014 Survey 500 orthopedic clinic patients or religion. Surgeon training considered moderately important Surgeon knowledge, compassion, and politeness are more important than surgeon appearance. Patients prefer "smart Aitken et al., 2013 Questionnaire 427 orthopedic patients casual" dress for surgeons over white coat and scrubs Patients trust information from physicians and hospitals more Alexander et al., 8,140 patients with chronic than information from personal, governmental, or insurer 2011 Survey illness sources 59,841 patients who had surgery Patients who were non-white, did not have private insurance, or Al-Refaie et al., for lung, esophagus, or pancreas had more comorbidities were significantly more likely to receive 2012 Logistic regression tumors surgery at a low volume hospitals (p < .05) Bederman et al., 164 lumbar spinal surgery Quality of life factors were most important for patients (p ≤ . 2009 Conjoint analysis patients 0005) Implementation of Leapfrog standards may have prevented Birkmeyer and >1 million patients for five high- 7,818 of 23,790 surgical deaths from the five procedures in Dimick, 2004 Meta-analysis risk surgeries in 2000 2000. 15,796 Medicare patients who With high volume standards for hospitals, over 50% of patients underwent esophagectomy or would increase travel times by over one hour. If not set too high, Birkmeyer et al., pancreatic resection from 1994- volume standards could be used for select surgeries without 2003 Simulated trial 1999. making travel times unreasonable High volume hospitals had significantly lower mortality, fewer Multivariate 129,609 pancreatectomy patients complications, and shorter median length of stay compared to Bliss et al., 2014 regression from 2004-2011 non-high volume centers (p < .001). Physician certification and specialization, recommendations Bornstein, Marcus, from family and friends, and neatness of physician and office and Cassidy, 2000 Survey 636 community residents were most important factors Multivariate 932 breast cancer surgery Patients involved with choosing surgeon were more likely to be Bouche et al., 2008 analysis patients treated at low-volume hospitals
251 patients being evaluated for elective primary total joint Surgeon manner, surgeon QI, hospital quality, and surgeon Bozic et al., 2012 Survey arthroplasty reputation were most important factors for patients Brown, Clark, and Cardiologists are ethically obligated to use QI when referring Oakley, 2012 Commentary Information on QI report cards patients to cardiac surgeons Bucknall and Pynsent, 2009 Questionnaire 182 orthopedic patients 89% of patients had no preference for surgeon gender Public QI should be accurate, collected actively, validated, and Canto, 2007 Commentary Information on QI report cards include more than merely short-term mortality indicators Information used by patients when selecting a surgeon differed Carlin, Kralweski, 480 knee or hip replacement depending on if the patient lived in an urban or rural setting. and Savage, 2013 Survey surgery patients Only 12.5% of patients used QI in their decision-making 8,370 patients who underwent Access to high volume hospitals was associated with year, age, Multivariate pancreatic resections from 2000- and race. Non-white and older patients were less likely to be Chang et al., 2009 regression 2005 referred to high volume centers (p < .001) 51% of patients preferred a male surgeon, 3% preferred a female Childs et al., 2005 Survey 146 female primary care patients surgeon, and 46% had no preference for surgeon gender 47% of patients held quality of life to be the most important 98 patients considering palliative factor. 39% based their decision in their doctor's Collins et al., 2013 Questionnaire surgery recommendation.
Conner-Spady et 176 patients undergoing total al., 2014 Questionnaire joint replacement surgery Surgeon and hospital reputations were most important factors Dammen et al., Discrete-choice 1,303 cataract and total knee For both surgeries, the most significant factors for patients were 2012 experiment replacement patients distance, waiting times, and complication concerns (p = .000) de Groot et al., Patients use own experiences and experiences of others more 2011 Questionnaire 337 new surgical patients than public information when choosing hospitals for surgery Hospital reputation and hospital atmosphere were the most 2,122 patients who underwent 1 important factors in choosing hospital for surgical care. Patients Djis-Elsinga et al., of 6 elective surgeries from will use more information for future choices than they used for 2010 Questionnaire 2005-2006 past choices 82% of respondents indicated QI would be very useful in choosing a surgeon. Only 6.4% of patients were always able to Donelan et al., 337 individuals from general find the surgeon with the lowest risk mortality when presented 2011 Questionnaire population with four different QI displays Patients did not show significant preference for a particular Dusch, O'Sullivan, surgeon gender. Preferred surgeon demeanor may vary by type and Ascher, 2014 Survey 436 general medicine patients of surgery Patients, especially Medicare recipients, need more objective Edgman-Levitan Review and Available medical literature and information to assist them in making educated healthcare and Cleary, 1996 interviews health plan managers decisions 214 cancer patients seeking Best-worst scaling surgery at Johns Hopkins Surgeon caseload, training, and experience and hospital Ejaz et al., 2014 survey Hospital reputation were the most important factors Information on performance data Distribution of QI alone will not have an effect. QI must be Epstein, 2000 Commentary use composed of easily understood quality indicators Faber et al., 2009 Review Available medical literature Patients value and use QI to choose better healthcare plans Information on the Internet is of poor quality. Physicians should Cross-sectional Web-based pediatric urology be able to guide patients to more credible sources of information Fast et al., 2012 study information to be used in decision-making Patients value empathy, compassion, and communication in surgeons and may use these attributes to infer about a surgeon's Fiala, 2012 Review Available medical literature technical competence Finks, Osborne, >3.2 million patients for eight Operative mortality fell for all procedures from 8%-36%. Higher and Birkmeyer, Chi-squared and high-risk surgeries between hospital volume explained much of this decline for three of the 2009 regressions 1999-2008 eight surgeries All else equal, patients prefer local care. If local hospitals offered twice the mortality rate of regional hospitals, 45% of Finlayson et al., 100 patients awaiting elective patients would still opt for local surgery. 18% of patients would 1999 Questionnaire surgery prefer local care even if the local mortality rate were 18% 65% of patients used the Internet to research their condition. 36% of patients used the Internet to research their surgeon. More Fraval et al., 2012 Survey 400 patients from surgical clinics credible Internet information is needed 96 individuals chosen from Surgeon reputation and certification were most important of 8 Galanis et al., 2013 Questionnaire nonsurgical clinics factors. Surgeon training only moderately important The mean quality of web information was "poor" and over 50% Goslin and DISCERN Web-based ear, nose, and throat of websites were rated "poor" or "very poor." Only 13% of Elhassan, 2013 evaluation surgery information websites were rated "good" or "excellent" Time trade-off 50 outpatient patients and 16 Patients were significantly less likely than surgeons to trade off Gu et al., 2009 method orthopedic surgeons years of life for a reduction in "constant severe pain" (p < .05) 59% of people consider physician rating websites to be very important or somewhat important. 65% of patients were aware of such rating sites. 43% of the patients who have not sought out Hanauer et al., 2,137 individuals from general physician rating sites expressed not trusting the information on 2014 Survey public those sites Hansrani et al., Questionnaire 581 patients at an elective Almost 50% of patients chose to delay surgery due to work 2014 orthopedic center commitments. Nearly 16% of patients could not accept an operation within 6 weeks of consultation Patients are willing to increase restrictions on healthcare access in exchange for higher quality healthcare. Consumers also Harris, 2002 Survey 206 adults in West Lost Angeles would benefit from QI sources 1,541 adults from general Patients are often passive healthcare consumers. Improvements Harris, 2003 Survey population in QI could help patients make better choices Hibbard, Sofaer, Survey and focus and Jewett, 1996 groups 72 randomly selected adults General healthcare consumers find QI to be relevant and useful Hibbard et al., Easily understood QI and cost data could help patients make 2012 Survey 1,421 healthcare consumers better-informed healthcare decisions 92% of patients were willing to travel >1 hour beyond the nearest hospital to access a surgeon with a 5% lower mortality 258 patients screened for rate, 2% lower amputation or stroke rate, a higher caseload, or Holt et al., 2010 Questionnaire abdominal aortic aneurysms routine use of endovascular repair Most patients referred to surgeon by another physician. Surgeon 1,844 women who had reputation was most commonly used factor for patients who Katz et al., 2007 Survey undergone breast cancer surgery selected their surgeon 41% of patients used the Internet to research their condition. 37% researched their surgery, 32% researched their surgeon, Kurup et al., 2012 Survey 877 surgical patients and 19% researched the hospital All else equal, patients prefer local care. If mortality risks were 67 abdominal aortic aneurysm increased at the local hospital, 9% still would prefer local Landau et al., 2013 Survey patients surgery Patients who were non-white, on Medicaid, or uninsured were less likely to have surgery at a high volume hospital and more Multivariate 719,608 patients who received 1 likely to have surgery at a low volume hospital (p < .05). There Liu et al., 2006 analysis of 10 surgeries from 2000-2004 are disparities in patients treated at high volume centers 57% of patients initially chose to delay surgery for 6 months to Llewelly-Thomas Time trade-off 124 patients waiting for hip or access a surgeon with a 1% mortality risk. Maximal wait times et al., 1998 method knee replacement surgery ranged from 1-26 months with a median of 7 months. 932 Medicare patients who Surgeon reputation was most frequently cited factor for underwent a total knee choosing location for surgery. Patients with lack of choice of Losina et al., 2005 Survey replacement surgeon more likely to be dissatisfied with care Patients may act as irrational consumers of medical care. Clearer Lubalin and Harris- and more informative health information can assist consumers in Kojetin Review Available medical literature making better choices 39,645 patients who underwent 1 Multivariate of 7 surgeries in 1983 in For 5 of 7 surgeries, hospitals with poorer outcomes saw fewer Luft et al., 1990 analysis California admissions Luft, Hunt, and Simultaneous >1 million patients for 17 Multiple possible explanations are possible for the lower Maerki, 1987 equation model different surgeries in 1972 mortality associated with higher-volume hospitals Patients who had in-hospital adverse outcomes were more likely Marang-van de 2,122 elective aorta to use information on mortality, complications, and hospital stay Mheen, et al., 2010 Questionnaire reconstruction patients if choosing a hospital for a subsequent surgery Marang-van de Surgery-specific and quality of care information are the most Mheen, et al., 2011 Questionnaire 665 former surgical patients important to patients when choosing between hospitals More QI may not necessarily lead patients towards viewing Marshall and healthcare as anything but a commodity. QI may not directly McLoughlin, 2010 Commentary Information on QI use lead to healthcare improvements QI is an important aspect of quality improvement, yet there is Marshall et al., uncertainty about its merits and risks. QI disclosure should be 2000 Review Available medical literature developed to minimize risks and maximize benefits 1,059 patients visiting OB/GYN Surgeon interpersonal skills, compassion, and expertise were Mavis et al., 2005 Questionnaire clinic most important factors McGlone, Butler, and McGlone, 222 individuals, mostly from Physician professional attributes were most important factors for 2002 Survey physician offices choosing a primary care physician Mennemeyer, The effect of the Health Care Morrisey, and Multivariate Financing Administration QI HCFA QI had essentially no effect on hospital discharges. QI Howard, 1997 regression released from 1986-1992 measures must be easily understood by the public to be effective Lower income and living alone were negative indicators of 384 patients undergoing surgical willingness to get surgery (p ≤ .015). Greater optimism of consults for shoulder or elbow success and competency in English were positive predictors of Modi et al., 2013 Questionnaire conditions willingness to get surgery (p ≤ .002) Interviews and focus group 18 patients who had undergone a Patient decision-making based on variable interplay of physician Moser et al., 2010 meetings hip or knee replacement and hospital attributes Consumers could understand QI, but often had problems 18 hip or knee replacement incorporating it into their decision-making. Information from Moser et al., 2010 Interview patients peers is considered very important in surgical planning Hospitals and physicians with better outcomes saw increased Mukamel and Multivariate Information from New York market shares. This correlation varied geographically and Mushlin, 1998 analysis State Cardiac Surgery Reports declined over time Close others have a large influence on surgical patients. Close Cross-sectional 91 patients receiving surgery for other influence was associated with a greater likelihood of Rini et al., 2011 study inflammatory bowel disease surgery (OR=1.97) Patients admitted to hospitals Romano and Zhou, Time-series classified as outliers for cardiac In New York, low-mortality outlier hospitals transiently 2004 analysis surgery morbidity and mortality experienced a significant increase in case volume Surgeon training, surgeon communication, and type of hospital Discrete-choice 103 patients who had undergone were important, statistically significant factors as determined by Salkeld et al., 2005 questionnaire surgery for colorectal cancer logistic regression (p<.001) Pennsylvania's QI Consumer Guide was known by 82% of physicians. Only 10% viewed the Guide as important in Schneider and 612 cardiologists and 85 cardiac assessing a cardiothoracic surgeon. The Guide held limited sway Epstein, 1996 Survey surgeons in Pennsylvania among cardiovascular specialists. Only 12% of patients knew about Pennsylvania's QI consumer guide before choosing a surgeon, and less than 1% knew the correct rating of their surgeon or hospital. 58% of patients would Schneider and 474 cardiac surgery patients in have changed surgeons if the guide had indicated poor Epstein, 1998 Survey Pennsylvania performance results for that physician. Consumers may not use public QI. Nevertheless, QI should Schneider and remain public in order to force healthcare institutions towards Liberman, 2001 Review Available medical literature higher quality care Schwartz, 510 Medicare patients who had Hospital reputation was second most important of 6 factors, Woloshin, and Telephone one of five elective, high risk nearly equally important as the number one factor (surgeon Birkmeyer, 2005 interview surgeries reputation) Patients strongly preferred local treatment for vascular surgery. They were willing to wait between 4 and 5.4 months for Shackley, Slack, treatment and incur a 2.7-4.4% increase in mortality risk to be and Michaels, 2001 Conjoint analysis 125 vascular patients treated locally Shah and Hospital cleanliness and reputation and urologist reputation Dickinson, 2009 Questionnaire 199 urology outpatients were the most important factors Cost and quality information awareness is low among patients. Sick and Abraham, Information found on the Internet is usually based on anecdotes 2011 Review Available medical literature and is produced by private companies 153 people who had recently Physician communication skills, hospital staff communication Survey and focus been hospitalized or had a loved and responsiveness and hospital cleanliness were most important Sofaer et al., 2005 groups one hospitalized factors High volume centers yield better results for some surgeries, yet those centers are often in urban areas. A balance should be Stewart, Long, and struck so that rural patients can access quality care without Tulloh, 2006 Viewpoint Information on travel times unreasonable travel burdens 81 patients who had undergone Thrumurthy et al., Discrete-choice oesophagogastric cancer Quality of life, cure rate, surgeon reputation, and morbidity were 2011 questionnaire resection most important factors Patients mostly use advice of friends or relatives when selecting 5,800 adults from general primary care physicians, but mainly use referrals from Tu and Lauer, 2008 Survey population physicians to choose specialists and facilities for care Both kinds of patients are less likely to bypass the nearest hospital when travel time to the next closest hospital increases, Varkevisser and though the coefficient is lower for neurosurgery patients. 38% of van der Geest, Multivariate 58,475 orthopedic and orthopedic patients and 54% of neurosurgery patients bypassed 2007 analysis neurosurgery patients their nearest hospital in 2003 Patient choice is based on a complex mix of patient and provider attributes, and patients may not make rational decisions about Victoor et al., 2012 Review Available medical literature their healthcare Vonberg, Sander, and Gastmeier, Telephone General cleanliness, low infection rate, and friendly staff were 2008 interview 1000 German households the most important factors for choosing a hospital Waltzman, Scholz, Surgeon board certification and method of referral were most and Evans, 2011 Conjoint analysis 111 plastic surgery patients important factors for patients The quality of online information is variable and often incomplete. Patients cannot make well-informed decisions Wasserman et al., Cross-sectional Web-based colorectal cancer regarding colorectal cancer surgery based on Internet 2014 study surgery information information alone 3% of websites were rated "excellent," while 50% received a DISCERN Web-based cervical spine rating of "poor" or "very poor." The search for useful medical Weil et al., 2014 evaluation surgery information information on the Internet is difficult and often fruitless 500 Medicare patients who had Wilson, Woloshin, Telephone one of five elective, high risk 73% of patients either decided on a location for surgery with and Schwartz, 2007 interview surgeries their surgeon or deferred the decision to the surgeon alone 37% of websites were deemed "good" or "excellent." The Yeung and DISCERN Web-based diverticular disease quality of information on the Internet was questionable and Mortensen, 2012 evaluation surgery information websites sponsored by private companies may be biased 14 patients with end-stage ankle Surgeons are key sources of information for patients. Trust in Zaidi et al., 2013 Interview osteoarthritis surgeon was major factor for patients' choices
Supplemental Table 1: the 86 studies included in the review