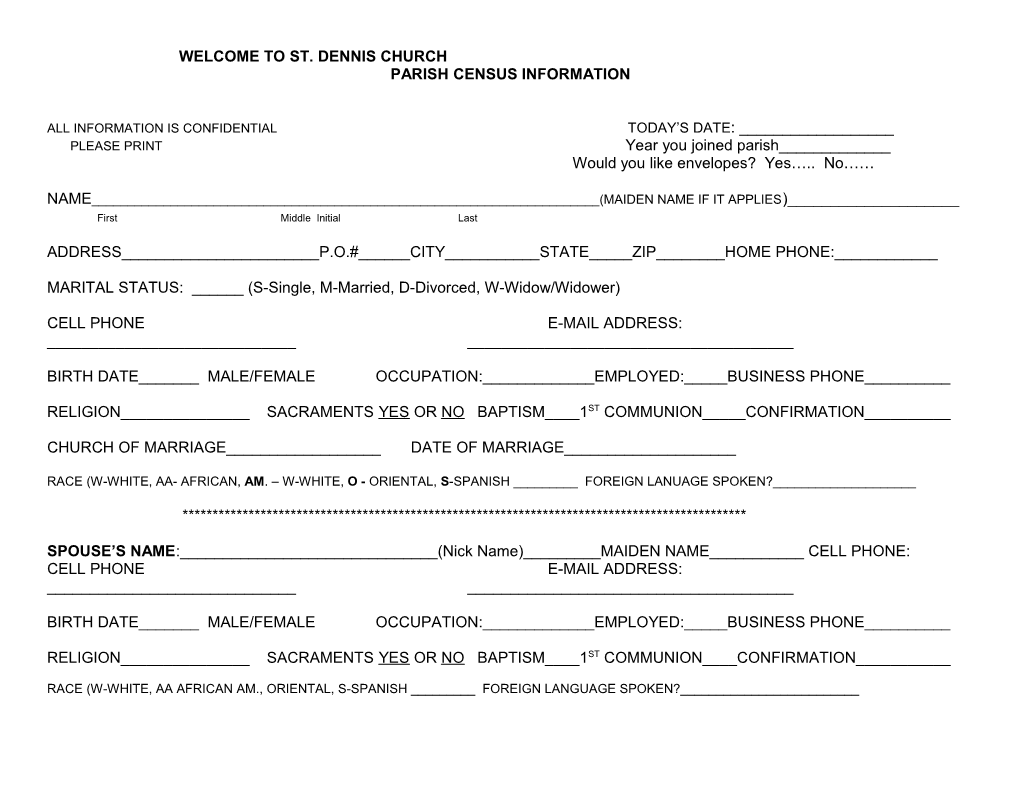
WELCOME TO ST. DENNIS CHURCH PARISH CENSUS INFORMATION
ALL INFORMATION IS CONFIDENTIAL TODAY’S DATE: ______PLEASE PRINT Year you joined parish______Would you like envelopes? Yes….. No……
NAME______(MAIDEN NAME IF IT APPLIES)______First Middle Initial Last
ADDRESS______P.O.#______CITY______STATE_____ZIP______HOME PHONE:______
MARITAL STATUS: ______(S-Single, M-Married, D-Divorced, W-Widow/Widower)
CELL PHONE E-MAIL ADDRESS: ______
BIRTH DATE______MALE/FEMALE OCCUPATION:______EMPLOYED:_____BUSINESS PHONE______
RELIGION______SACRAMENTS YES OR NO BAPTISM____1ST COMMUNION_____CONFIRMATION______
CHURCH OF MARRIAGE______DATE OF MARRIAGE______
RACE (W-WHITE, AA- AFRICAN, AM. – W-WHITE, O - ORIENTAL, S-SPANISH ______FOREIGN LANUAGE SPOKEN?______
**********************************************************************************************
SPOUSE’S NAME:______(Nick Name)______MAIDEN NAME______CELL PHONE: CELL PHONE E-MAIL ADDRESS: ______
BIRTH DATE______MALE/FEMALE OCCUPATION:______EMPLOYED:_____BUSINESS PHONE______
RELIGION______SACRAMENTS YES OR NO BAPTISM____1ST COMMUNION____CONFIRMATION______
RACE (W-WHITE, AA AFRICAN AM., ORIENTAL, S-SPANISH ______FOREIGN LANGUAGE SPOKEN?______CHILDREN LIVING AT SAME ADDRESS
CHILD’S NAME______BIRTHDATE:______MALE OR FEMALE? Religious Education: Grade_____ Sacraments: Baptism Date______Church______1st Communion Date :______Church______Confirmation Date______Church______
CHILD’S NAME______BIRTHDATE:______MALE OR FEMALE? Religious Education: Grade______Sacraments: Baptism Date:______Church______1st Communion Date :______Church______Confirmation Date______Church______
CHILD’S NAME______BIRTHDATE:______MALE OR FEMALE? Religious Education: Grade______Sacraments: Baptism Date:______Church______1st Communion Date :______Church______Confirmation Date______Church______
CHILD’S NAME______BIRTHDATE:______MALE OR FEMALE? Religious Education: Grade______Sacraments: Baptism Date:______Church______1st Communion Date ______Church______Confirmation Date______Church______
Please use another sheet of paper if needed
OTHER ADULTS LIVING AT SAME ADDRESS (PARENTS/IN-LAWS/SIBLINGS) NAME:______BIRTHDATE______HOW RELATED______SPECIAL NEEDS (if any)______
How can we help you? Do you have any particular needs at this time, ie., Home-bound visits, nursing home visits, etc.
Would you like to share your talents/time with us? List of Ministries, please check what you are interested in or what you are currently doing: Catechist____Catechist Aid,___ RCIA,___ Altar Server-youth___, Church Choir___, Lector___, Eucharistic Minister___, or call the church and let us know how you would like to volunteer.
ST.DENNIS CHURCH P.O. BOX 249 GALENA, MD 21635 410-648-5145 e-mail: [email protected] web site: stdennischurch.org