Implementation Strategies and Associated Concerns HS 490-CHAPTER 12
A great deal of work goes into developing a program before it is ready for implementation. The process used to implement a program may have much to say about its success. This chapter presents two models for program implementation. The first, a modification of the Parkinson and Associates (1982) model, includes three commonly used strategies: piloting, phasing in , and total implementation. The second, Borg and Gall’s (1989) research and development cycle, can be modified to provide a thorough implementation strategy. Also presented in this chapter are matters that need to be considered and planned for prior to implementation.
Implementation Implementation consists of initiating the activity, providing assistance to it and to its participants, problem-solving issues that may arise, and reporting on progress.
Strategies for Implementation: Implementation – is the 1st phase of converting planning, goals, and objectives into action. Adoption and sustainability are the last two phases. Sustainability is the maintenance and institutionalization of a program or its outcomes for an extended time period. First Implementation Model- Parkinson and Associates (1982) Second Implementation Model- Borg and Gall (1989) SUSTAINABILITY – is the maintenance and institutionalization of a program or its outcomes for an extended period of time.
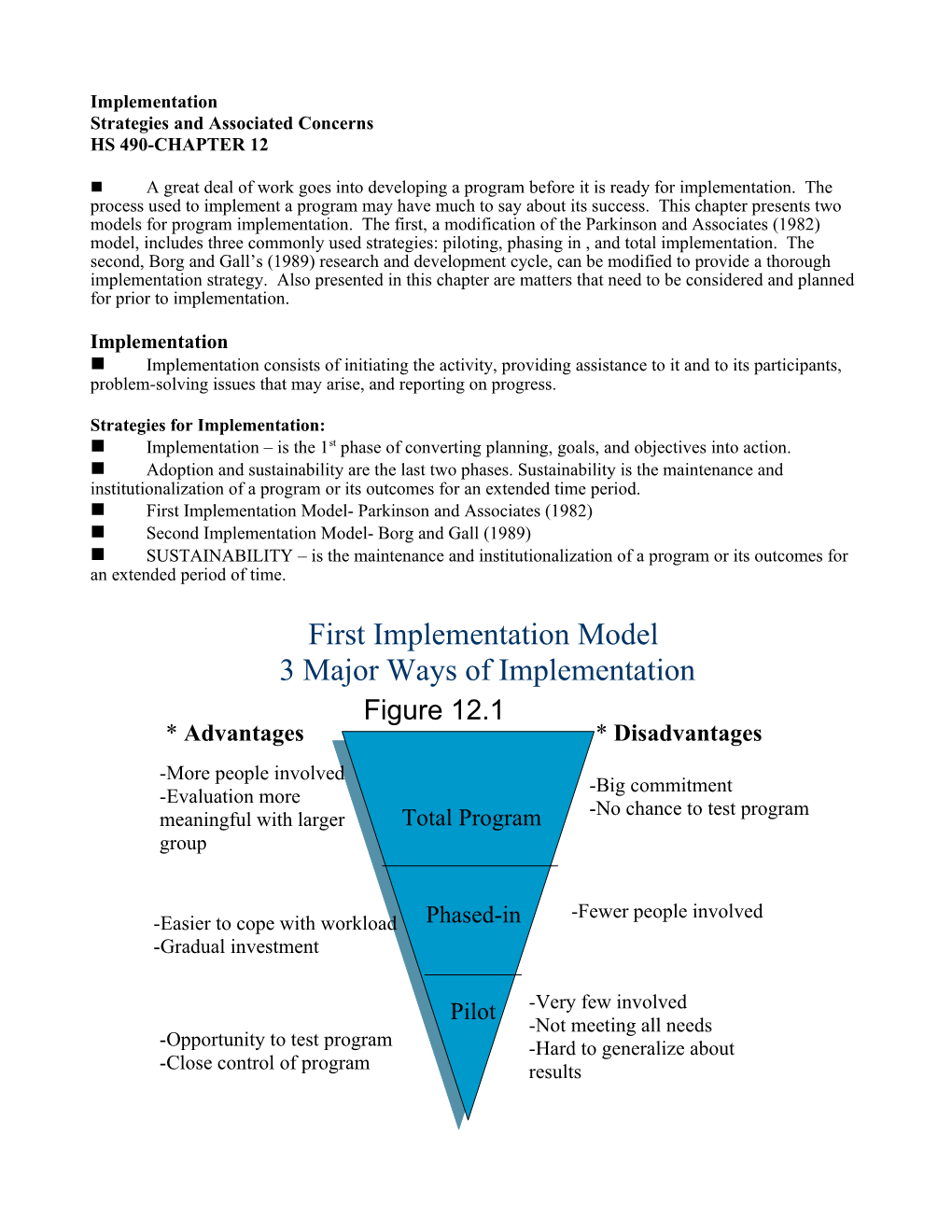
First Implementation Model 3 Major Ways of Implementation Figure 12.1 * Advantages * Disadvantages -More people involved -Big commitment -Evaluation more -No chance to test program meaningful with larger Total Program group
-Fewer people involved -Easier to cope with workload Phased-in -Gradual investment
Pilot -Very few involved -Not meeting all needs -Opportunity to test program -Hard to generalize about -Close control of program results
1. Pilot Testing Pilot testing (or piloting or field testing) the program is a crucial step. Pilot testing allows planners to work out any bugs before the program is offered to a larger segment of the target population, and also to validate the work that has been completed up to this point. As part of the piloting program, planners should check on the following: The intervention activities work as planned. Adequate program logistics have been worked out. The program participants are asked to evaluate the program.
2. Phasing In (Adoption of the Program) Once a program has been piloted and revised, the program should be phased in rather than implemented in its entirety. Phasing in allows the planners to have more control over the program and helps to protect planners and facilitators from getting in over their heads. There are several ways in which to phase in a program: By different program offerings. By a limit on the number of participants. By choice of location. By participant ability.
A program planned for a college town might be offered first on campus, then off campus to the general public.
Identifying and Prioritizing the Task to be Completed: Many of these tasks are often referred to as program LOGISTICS, which is defined as the procurement, maintenance, and transportation of materials, facilities, and personnel. Planning timetables that are commonly used include: 1. Key Activity Chart may be the simplest of the tools. It includes three components, a listing of all the key activities or tasks to the carried out, an estimate of the dates when the activities will take place, and the time allocated to complete the activities. 2. Task Development Time Line identifies the tasks that need to be completed and the time frame in which the tasks will be completed. (See Figure 12.1 pg. 275) 3. Gant Chart does the same plus provides an indication of the progress made toward completing the task by using different size lines to distinguish between the projected time frame for a task and the progress toward completing the task. (See Figure 12.2 Pg. 276)
PERT is an acronym for Program Evaluation and Review Technique. PERT charts are more complex than Gant charts and thus have been less frequently used with health promotion programs. (For more information refer to business management text books)
Critical Path Method (CPM) charts are similar to PERT charts and are sometimes known as PERT/CPM
Establishing a system of Management: Management has been defined as “the process of achieving results through controlling human, financial, and technical resources.” 3. Total Implementation Implementing the total program all at once would be a mistake. Rather, planners should work toward total implementation through the piloting and phasing-in processes. The only exceptions to this might be “one-shot” programs, such as programs designed around a single lecture, and possibly screening programs, but even then piloting would probably help.
Second Implementation Model (Borg and Gall) Figure 12.2 Major Steps of Borg and Gall’s Research and Development Cycle Applied to Creating a Health Promotion Program (The following three slides are from Figure 12.2)
Research and information collecting: Includes needs assessment, review of the literature, small-scale research studies, and preparation of report on the state of the art. Planning: Includes defining skills to be learned, stating and sequencing the objectives, identifying learning activities, and small-scale feasibility testing. Development of preliminary form of program: Includes preparation of instructional materials, procedures, and evaluation instruments.
Preliminary field testing: Program given to just a few individuals from the target population. Interview, observational, and questionnaire data collected and analyzed. Main program revision: Based on results of preliminary field test. Main field testing: Program given to approximately twice as many as in preliminary field test. Pre-and post program quantitative data on participants collected; results examined with respect to program objectives and compared to control/comparison group, when possible.
Operational program revision: Based on results of the main field test. Operational field testing: Program given to approximately twice as many as in main field test. Interview, observational, and questionnaire data collected and analyzed. Final program revision: Based on results of the operational field test. Dissemination and implementation: Program shared with others and implemented where appropriate.
First Day of Implementation (Program launch or Program rollout) No matter what implementation model or strategy the planners choose, there will be a “first day” for the program. The first day of the program is just an extension of the fourth P (see chapter 11). 1. Product; 2. Price; 3. Placement; 4. Promotion The focus of promotion is on creating and sustaining demand for the product.
Dealing with Problems: Even if a program has been piloted, problems can still arise. The problems that could be encountered can range from petty concerns to matters of life and death. Problems might involve logistics (room size, meeting time, or room temperature), participant dissatisfaction, or a personal or medical emergency. NEWS HOOK: Because many health promotion programs are not newsworthy in their own right, it might be necessary to use NEWS HOOK to interest the media in the Program, which is defined as something that would make the media want to cover the launch.
Reporting and Documenting Planners must keep others informed about the progress of the program for several reasons, including 1) accountability, 2) public relations 3) motivation of present participants, and 4) recruitment of new participants. The exact nature of the reporting or documenting will vary, but it is important for planners to keep all stakeholders informed.
Implementation Timetable To provide some guidance in implementing a program, it is helpful to compile a tentative timetable for implementation. It might even be useful to include the entire planning process. Figure 12.3 presents an example of a planning and implementation timetable using a Gantt Chart. Sample Planning and Implementation Timetable
Tasks Months Year 1 J F M A M J J A S O N D Develop program rationale Conduct needs assessment Develop goals and objectives Create intervention Conduct formative evaluation Assemble necessary resources Market program Pilot test program Refine program Phase in intervention #1 Phase in intervention #2 Phase in intervention #3 Figure 12.3 Charts: see pages 275 and 276 Key activity chart Task Development Time Line Gantt Chart PERT-is an acronym for Program Evaluation and Review Technique CPM- is an acronym for Critical Path Method Management- is defined as “the process of achieving results through controlling human financial, and technical resources.” Program Launch or Program Rollout- is an extension of The fourth (P) discussed in Chapter 11 – (Promotion) it is the initiation of the program being implemented. News Hook- Something that would make the media want to cover the launch.
Sample Planning and Implementation Timetable
Tasks Months Year 2 J F M A M J J A S O N D Phase in intervention #4 Total Implementation Collect and analyze data for evaluation Prepare evaluation report Distribure report Continue with follow-up for long-term evaluation
Figure 12.3
Concerns Associated with Implementation: Legal Concerns Liability is on the mind of many professionals today because of the concern over lawsuits. With this in mind, all personnel connected with the planned health promotion program, no matter how small the risk of injury to the participants (physical or mental), should make sure that they are adequately covered by liability insurance. In addition, program personnel should have an understanding of informed consent, negligence, and approval of appropriate professional groups.
Legal Concerns Informed consent- As a part of the process of obtaining informed consent from participants, program facilitators should: – Explain the nature and purpose(s) of the program. – Inform program participants of any inherent risks or dangers associated with participation and any possible discomfort they may experience. – Explain the expected benefits of participation. – Inform participants of alternative programs (procedures) that will accomplish the same thing. – Indicate to the participants that they are free to discontinue participation at any time. Informed consent forms must be signed by participants before they enter the program.
Legal Concerns Negligence- Negligence is failing to act in a prudent (reasonable) manner. Negligence can arise from two types of acts: - Omission - Commission - The act of omission is not doing something when you should, such as failing to warn program participants of the inherent danger in participation. An act of commission is doing something you should not be doing, such as leading an aerobic dance program when you are not trained to do so. - Negligence is failing to act as a prudent and reasonable individual. Prudent acting in a reasonable person, with the same training and under the same circumstances.
Reducing the Risk of Liability The real key to avoiding liability is to reduce your risk by planning ahead. Tips for reducing the risk of liability: Be aware of legal liabilities. Select certified instructors [in the activity and emergency care procedures] to lead classes and supervise exercise equipment [and for that matter all types of equipment]. Use good judgment in setting up programs and provide written guidelines for medical emergency procedures.
Tips for reducing the risk of liability: Inform participants about the risks and danger of exercise [or other activities] and require written informed consent. Require that participants obtain medical clearance before entering an exercise program [or other strenuous programs]. Instruct staff not to “practice medicine,” but instead to limit their advice to their own area of expertise. Provide a safe environment by following building codes and regular maintenance schedule for equipment. Purchase adequate liability insurance for all staff. It is recommended that “a million dollar per claim liability policy for all employees” be obtained.
Medical Concerns Does the program put the participants at any special medial risk so that they would need medical clearance.
Program Safety Providing a safe environment includes finding a safe program location (example: low-crime area), ensuring that classrooms and laboratories are free of hazards, providing qualified facilitators, supplying first-aid equipment, and developing an emergency care plan.
A checklist of items that should be considered when creating an appropriate emergency care plan include: (Figure 12.4) __ 1. Duties of program staff in an emergency situation are defined. __ 2. Program staff are trained (CPR and first aid) to handle emergencies. __ 3. Program participants are instructed what to do in an emergency situation (e.g., medical, natural disaster). __ 4. Participants with high-risk health problems are known to program staff. __ 5. Emergency care supplies and equipment are available. A checklist of items that should be considered when creating an appropriate emergency care plan include: (Figure 12.4) __ 6. Program staff has access to a telephone. __ 7. Standing orders are available for common emergency problems. __ 8. There is a plan for notifying those needed in an emergency situation. __ 9. Responsibility for transportation of ill/injured is defined. __ 10. Accident report form procedures are defined. A checklist of items that should be considered when creating an appropriate emergency care plan include: (Figure 12.4) __ 11. Universal precautions are outlined and followed. __ 12. Responsibility for financial charges incurred in the emergency care process are defined. __ 13. The emergency care plan has been approved by the appropriate personnel. __ 14. The emergency care plan is reviewed and updated on a regular basis. __ 15. HIPAA- Health Insurance Portability and Accountability Act __ 16. Anonymity- exists when no one, including the planners can relate to a participants identity to any information pertaining to the process. __ 17. Confidentiality- exists when planners are aware of the participants’ identities and have promised not to reveal those identities to others.
Program Registration and Fee Collection If the program you are planning requires people to sing up and/or pay fees, you will need to establish registration procedures. e.g., 1-pre-registration, 2-by mail, 3-in person, 4-via an indirect method like payroll deduction, 5-at the first session. Planners should also give thought to the type of payment that will be accepted (cash, credit card, or check). Procedures for Record keeping 1. Medical information 2. Participant progress 3. Evaluations In addition, planners must decide whether participant files will be kept in a traditional way, with paper and pencil, or using a computer software program. 4. The importance of privacy for those planners working in health care settings was further emphasized in April 2003 with enactment of the Standards for Privacy Individually Identifiable Health Information Section (The Privacy Rule) of the Health Insurance Portability and Accountability Act of 1996 (officially known as Public Law 104-191 and referred to as HIPAA).
Before implementation, program planners need to make sure that arrangements are made for a number of small but important program details.
The two techniques that are used to protect the privacy of participants are anonymity and confidentiality. Anonymity exists when no one, including the planners, can relate a participant’s identity to any information pertaining to the program (Dane, 1990). Thus information associated with a participant may be considered anonymous when such information cannot be linked to the participant who provided it. In applying this concept, planners need to ensure that collected data had no identifying information attached to them such as the participant’s name, social security number, or any other less common information. Confidentiality exists when planners are aware of the participants’ identities and have promised not to reveal those identities to others (Dane, 1990). When handling confidential data, planners need to take every precaution to protect the participants’ information. Often this means keeping the information “under lock and key” while participants are active in a program, then destroying (i.e., shredding) the information when it is no longer needed.
Logistics Logistics are defined as the procurement, maintenance, and transportation of materials, facilities, and personnel. Reserving space where the program is to be held, making sure audiovisual equipment is available when requested, ordering the correct number of participant education packets, and arranging for interpreters when working with a multicultural population are examples of program logistics that are important to the success of the program. Take care of the small things (details) and the rest will fall into place.
Moral and Ethical Concerns There are times when certain behavior is legal but not moral or ethical. Program planning and evaluation provide the health educator with almost daily opportunities to make decisions that affect other people. Some of these decisions are easy to make; others raise the question of what is the right or wrong decision. In other words, because of the nature of health promotion, program planners are confronted with many moral and ethical decisions. Who is to judge what is right and wrong? Most often, these decisions are compared to a standard of practice that has been defined by other professionals in the same field.
Figure 12.5 Hierarchy of Autonomy 1. Facilitation: Assist in achieving objectives set by a target group. Examples: putting safety belts in cars or teaching people the skills necessary to perform CPR. 2. Persuasion: Argue and reason. Examples: tell people about the importance of wearing safety belts or taking blood pressure medicine. 3. Manipulation: Modify the environment around a person or the psychic disposition of the person. Example: automatic safety belts. 4. Coercion: Treat of deprivation. Example: safety belt or motorcycle helmet laws and fine.
Nonmaleficence Nonmaleficence means to not cause harm or not doing evil. For example, is it permissible to use an aversive behavior technique to get someone to stop smoking? Which is worse, smoking cigarettes or receiving some physical punishment for doing so? Primum non nocre: First do no harm.
Beneficence Beneficence is bringing about or doing good- can also be related to ethical issues. Can there be any question whether it is right to do good? If the good comes at the expense of another, then it raises ethical concerns.
Procedural Manual and/or Participant’s Manual Depending on the complexity of a program, there may be a need to develop manuals or to purchase them from a vendor. Developing a manual in-house is a major task; therefore, adequate resources and time need to be given to developing manuals.
Training for Facilitators If a program that is being planned needs a specially qualifies person (certified or licensed) to facilitate it, every effort should be made to secure such a person.