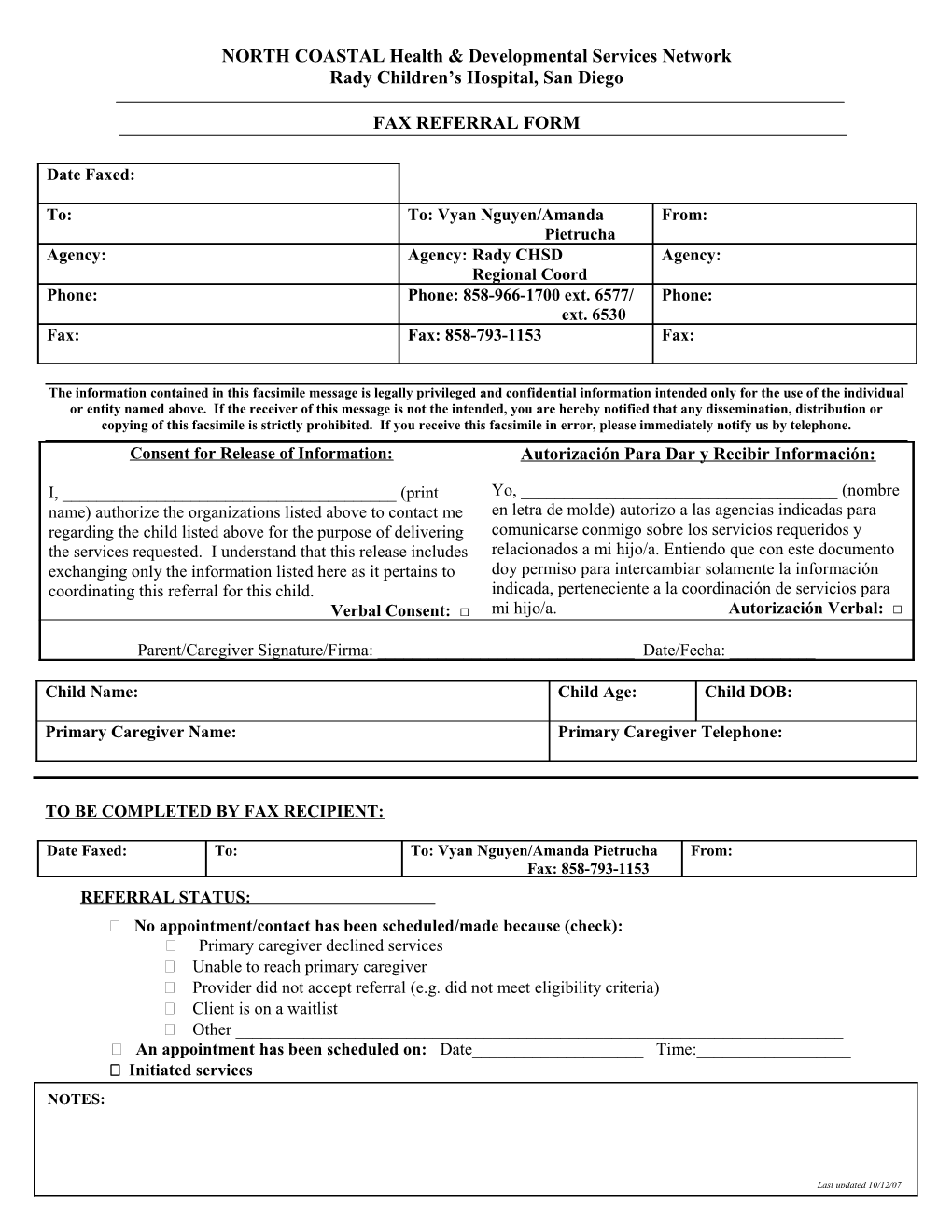
NORTH COASTAL Health & Developmental Services Network Rady Children’s Hospital, San Diego
FAX REFERRAL FORM
Date Faxed:
To: To: Vyan Nguyen/Amanda From: Pietrucha Agency: Agency: Rady CHSD Agency: Regional Coord Phone: Phone: 858-966-1700 ext. 6577/ Phone: ext. 6530 Fax: Fax: 858-793-1153 Fax:
The information contained in this facsimile message is legally privileged and confidential information intended only for the use of the individual or entity named above. If the receiver of this message is not the intended, you are hereby notified that any dissemination, distribution or copying of this facsimile is strictly prohibited. If you receive this facsimile in error, please immediately notify us by telephone. Consent for Release of Information: Autorización Para Dar y Recibir Información:
I, ______(print Yo, ______(nombre name) authorize the organizations listed above to contact me en letra de molde) autorizo a las agencias indicadas para regarding the child listed above for the purpose of delivering comunicarse conmigo sobre los servicios requeridos y the services requested. I understand that this release includes relacionados a mi hijo/a. Entiendo que con este documento exchanging only the information listed here as it pertains to doy permiso para intercambiar solamente la información coordinating this referral for this child. indicada, perteneciente a la coordinación de servicios para Verbal Consent: □ mi hijo/a. Autorización Verbal: □
Parent/Caregiver Signature/Firma: ______Date/Fecha: ______
Child Name: Child Age: Child DOB:
Primary Caregiver Name: Primary Caregiver Telephone:
TO BE COMPLETED BY FAX RECIPIENT:
Date Faxed: To: To: Vyan Nguyen/Amanda Pietrucha From: Fax: 858-793-1153 REFERRAL STATUS: No appointment/contact has been scheduled/made because (check): Primary caregiver declined services Unable to reach primary caregiver Provider did not accept referral (e.g. did not meet eligibility criteria) Client is on a waitlist Other ______ An appointment has been scheduled on: Date______Time:______ Initiated services NOTES:
Last updated 10/12/07