Neonatal Intubation Simulation with Virtual Reality and Haptic Feedback
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Motion and Context Sensing Techniques for Pen Computing
Motion and Context Sensing Techniques for Pen Computing Ken Hinckley1, Xiang ‘Anthony’ Chen1,2, and Hrvoje Benko1 * Microsoft Research, Redmond, WA, USA1 and Carnegie Mellon University Dept. of Computer Science2 ABSTRACT We explore techniques for a slender and untethered stylus prototype enhanced with a full suite of inertial sensors (three-axis accelerometer, gyroscope, and magnetometer). We present a taxonomy of enhanced stylus input techniques and consider a number of novel possibilities that combine motion sensors with pen stroke and touchscreen inputs on a pen + touch slate. These Fig. 1 Our wireless prototype has accelerometer, gyro, and inertial sensors enable motion-gesture inputs, as well sensing the magnetometer sensors in a ~19 cm Χ 11.5 mm diameter stylus. context of how the user is holding or using the stylus, even when Our system employs a custom pen augmented with inertial the pen is not in contact with the tablet screen. Our initial results sensors (accelerometer, gyro, and magnetometer, each a 3-axis suggest that sensor-enhanced stylus input offers a potentially rich sensor, for nine total sensing dimensions) as well as a low-power modality to augment interaction with slate computers. radio. Our stylus prototype also thus supports fully untethered Keywords: Stylus, motion sensing, sensors, pen+touch, pen input operation in a slender profile with no protrusions (Fig. 1). This allows us to explore numerous interactive possibilities that were Index Terms: H.5.2 Information Interfaces & Presentation: Input cumbersome in previous systems: our prototype supports direct input on tablet displays, allows pen tilting and other motions far 1 INTRODUCTION from the digitizer, and uses a thin, light, and wireless stylus. -

2019 Streamlight® Tactical Catalog
CELEBRATING 45 YEARS SOLVING LIGHTING PROBLEMS. INTRODUCING NEW PRODUCTS. ® 90 IT’S WHAT WE DO. PROTAC Since 1973, Streamlight has delivered effective, efficient high-performance lighting solutions. The latest technology delivers unmatched performance, unheard of durability and incredible value. We’ve earned our reputation one customer at a time. And we’re not about to let up now. SIEGE ® X USB 2 GET MORE INFO AT: STREAMLIGHT.COM / 800-523 –7488 / 610-631-0600 TLR-8 ® G RAIL-MOUNTED LIGHT TLR-6 ® NON-LASER TLR-6 ® FOR SIG SAUER P365 PROTAC ® RAIL MOUNT HL-X LASER BANDIT ® PRO USB HEADLAMP TLR-VIR ® II SPECIALTY PRODUCT TL-RACKER ™ FOREND LIGHT 3 STREAMLIGHT TLRs THE WIDEST RANGE OF WEAPON-MOUNTED LIGHTS Streamlight produces a full line of weapon-mounted lights with the features that law enforcement, conceal & carry, and sportsmen need: high-lumen, laser, and IR. Models to fit long guns and full-size and compact pistols. LIGHT ONLY LIGHT ONLY COMPACT & FULL FRAME PISTOLS UNIVERSAL RAIL-MOUNT MODELS TLR-7® TLR-1 HL® TLR-1® TLR-3® WHITE LIGHT ILLUMINATOR WHITE LIGHT ILLUMINATOR TLR-1®s WHITE LIGHT ILLUMINATOR WHITE LIGHT ILLUMINATOR NEW SUB-COMPACT & COMPACT PISTOLS TRIGGER GUARD & TLR-6® NON-LASER TLR-7® TLR-3® RAIL-MOUNT MODELS WHITE LIGHT ILLUMINATOR WHITE LIGHT ILLUMINATOR WHITE LIGHT ILLUMINATOR NEW LONG GUN / AR SHOTGUN FOREND & RAIL-MOUNT MODELS TLR-1 HL® PROTAC® RAIL MOUNT 1 PROTAC® T L R -1 HP L® TL-RACKER™ (Long Gun Kit) PROTAC® RAIL MOUNT 2 RAIL MOUNT HL-X (Long Gun Kit) WHITE LIGHT ILLUMINATOR/FOREND WHITE LIGHT ILLUMINATOR WHITE -

KSPC (Keystrokes Per Character) As a Characteristic of Text Entry Techniques
KSPC (Keystrokes per Character) as a Characteristic of Text Entry Techniques I. Scott MacKenzie Dept. of Computer Science York University Toronto, Ontario, Canada M3J 1P3 +1 416 736 2100 WQEGOIR^MI$EGQSVK Abstract. KSPC is the number of keystrokes, on average, to generate each character of text in a given language using a given text entry technique. We systematically describe the calculation of KSPC and provide examples across a variety of text entry techniques. Values for English range from about 10 for methods using only cursor keys and a SELECT key to about 0.5 for word prediction techniques. It is demonstrated that KSPC is useful for a priori analyses, thereby supporting the characterisation and comparison of text entry methods before labour-intensive implementations and evaluations. 1 Introduction An important research area in mobile computing is the development of efficient means of text entry. Interest is fueled by trends such as text messaging on mobile phones, two-way paging, and mobile web and email access. Coincident with this is the continued call in HCI for methods and models to make systems design tractable at the design and analysis stage [5]. This paper addresses these two themes. We propose a measure to characterise text entry techniques. It is calculated a priori, using a language model and a keystroke-level description of the technique. The measure is used to characterise and compare methods at the design stage, thus facilitating analyses prior to labour-intensive implementations and evaluations. 2 Keystrokes per Character (KSPC) KSPC is an acronym for keystrokes per character. It is the number of keystrokes required, on average, to generate a character of text for a given text entry technique in a given language. -
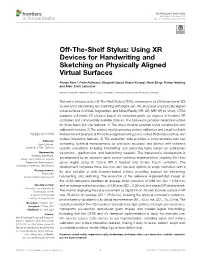
Off-The-Shelf Stylus: Using XR Devices for Handwriting and Sketching on Physically Aligned Virtual Surfaces
TECHNOLOGY AND CODE published: 04 June 2021 doi: 10.3389/frvir.2021.684498 Off-The-Shelf Stylus: Using XR Devices for Handwriting and Sketching on Physically Aligned Virtual Surfaces Florian Kern*, Peter Kullmann, Elisabeth Ganal, Kristof Korwisi, René Stingl, Florian Niebling and Marc Erich Latoschik Human-Computer Interaction (HCI) Group, Informatik, University of Würzburg, Würzburg, Germany This article introduces the Off-The-Shelf Stylus (OTSS), a framework for 2D interaction (in 3D) as well as for handwriting and sketching with digital pen, ink, and paper on physically aligned virtual surfaces in Virtual, Augmented, and Mixed Reality (VR, AR, MR: XR for short). OTSS supports self-made XR styluses based on consumer-grade six-degrees-of-freedom XR controllers and commercially available styluses. The framework provides separate modules for three basic but vital features: 1) The stylus module provides stylus construction and calibration features. 2) The surface module provides surface calibration and visual feedback features for virtual-physical 2D surface alignment using our so-called 3ViSuAl procedure, and Edited by: surface interaction features. 3) The evaluation suite provides a comprehensive test bed Daniel Zielasko, combining technical measurements for precision, accuracy, and latency with extensive University of Trier, Germany usability evaluations including handwriting and sketching tasks based on established Reviewed by: visuomotor, graphomotor, and handwriting research. The framework’s development is Wolfgang Stuerzlinger, Simon Fraser University, Canada accompanied by an extensive open source reference implementation targeting the Unity Thammathip Piumsomboon, game engine using an Oculus Rift S headset and Oculus Touch controllers. The University of Canterbury, New Zealand development compares three low-cost and low-tech options to equip controllers with a *Correspondence: tip and includes a web browser-based surface providing support for interacting, Florian Kern fl[email protected] handwriting, and sketching. -

Chapter 9. Input Devices
Table of contents 9 Input devices .................................................................................................................9-1 9.1 Keyboards ............................................................................................................. 9-4 9.2 Fixed-function keys .............................................................................................. 9-6 9.3 Pointing devices.................................................................................................... 9-7 9.3.1 General........................................................................................................... 9-7 9.3.2 Mouse ............................................................................................................ 9-9 9.3.3 Joystick and trackball .................................................................................. 9-10 9.3.3.1 General..................................................................................................9-10 9.3.3.2 Hand-operated displacement joysticks .................................................9-10 9.3.3.3 Finger-operated displacement joysticks................................................9-11 9.3.3.4 Thumb tip and fingertip-operated displacement joysticks....................9-13 9.3.3.5 Hand-operated isometric joysticks........................................................9-13 9.3.3.6 Thumb tip and fingertip-operated isometric joysticks..........................9-14 9.3.3.7 Ball controls..........................................................................................9-14 -

Virtual Reality Controllers
Evaluation of Low Cost Controllers for Mobile Based Virtual Reality Headsets By Summer Lindsey Bachelor of Arts Psychology Florida Institute of Technology May 2015 A thesis Submitted to the College of Aeronautics at Florida Institute of Technology in partial fulfillment of the requirements for the degree of Master of Science In Aviation Human Factors Melbourne, Florida April 2017 © Copyright 2017 Summer Lindsey All Rights Reserved The author grants permission to make single copies. _________________________________ The undersigned committee, having examined the attached thesis " Evaluation of Low Cost Controllers for Mobile Based Virtual Reality Headsets," by Summer Lindsey hereby indicates its unanimous approval. _________________________________ Deborah Carstens, Ph.D. Professor and Graduate Program Chair College of Aeronautics Major Advisor _________________________________ Meredith Carroll, Ph.D. Associate Professor College of Aeronautics Committee Member _________________________________ Neil Ganey, Ph.D. Human Factors Engineer Northrop Grumman Committee Member _________________________________ Christian Sonnenberg, Ph.D. Assistant Professor and Assistant Dean College of Business Committee Member _________________________________ Korhan Oyman, Ph.D. Dean and Professor College of Aeronautics Abstract Title: Evaluation of Low Cost Controllers for Mobile Based Virtual Reality Headsets Author: Summer Lindsey Major Advisor: Dr. Deborah Carstens Virtual Reality (VR) is no longer just for training purposes. The consumer VR market has become a large part of the VR world and is growing at a rapid pace. In spite of this growth, there is no standard controller for VR. This study evaluated three different controllers: a gamepad, the Leap Motion, and a touchpad as means of interacting with a virtual environment (VE). There were 23 participants that performed a matching task while wearing a Samsung Gear VR mobile based VR headset. -

Displaying Images on the SMART Sympodium
Displaying Images on the SMART Sympodium Anything you can display on your computer monitor will be projected onto the SMART Sympodium when you are connected to the system. For example, you could display: Word Documents Images Pages on the Internet PowerPoint Presentations Statistical or Design Programs Touching the SMART Sympodium screen with the pen stylus is equivalent to clicking on your computer screen using your mouse. Tap once on the Sympodium for a single mouse click; tap twice on the Sympodium for a double click. Drawing on the Sympodium Screen Use the stylus attached to the SMART Sympodium to draw on the screen. Do not write on the SMART Sympodium screen with dry-erase markers or pens. Note that the stylus pen color is changeable. It will write in the color you select by pen color selection buttons located at the top of the Sympodium screen. Also note that the pen and mouse are interchangeable. However if you lay the pen on the screen,the mouse will not function properly. Always rest the pen near the inside bottom of the screen when not in use. Note the buttons at the bottom of the Sympodium panel. These are shortcuts to some of the Sympodium tools. By default, the Floating Tools are not active. To activate them, click on the Start Menu and then "SMART Board Tools". The toolbar will fade in on the left side of the screen. To customize the appearance of your tools: Click on the "Gear" icon at the bottom of the Floating Toolbar. Drag the desired tool onto the bar; likewise, drag the undesired tool away. -

LNCS 4551, Pp
Stylus Enhancement to Enrich Interaction with Computers Yu Suzuki, Kazuo Misue, and Jiro Tanaka Department of Computer Science, University of Tsukuba 1-1-1 Tennodai, Tsukuba, Ibaraki 305-8573, Japan {suzuki,misue,jiro}@iplab.cs.tsukuba.ac.jp Abstract. We introduce a technique to enrich user interaction with a computer through a stylus. This technique allows a stylus to be manipulated in the air to operate applications in new ways. To translate the stylus manipulation into application behavior, we take an approach that we attach an accelerometer to the stylus. Such a stylus allows control through new operations like rolling and shaking, as well as through conventional operations like tapping or making strokes. An application can use these operations to switch modes or change parameters. We have implemented a number of applications, called the “Oh! Stylus Series,” that can be used with our proposed technique. Keywords: Stylus Enhancement, Interaction, Accelerometer, Behavior. 1 Introduction Computer operations based on a stylus, compared to those with a mouse, have the advantage of being direct and easy to understand. In terms of the interaction style, though, most stylus operations simply replace mouse operations, so these operations do not take advantage of all the ways a pen-shaped device can be handled. Potential interface techniques have not been realized because computers cannot detect stylus positions and movements when a conventional stylus is not touching the display. Our goal is to make pen-based applications more useful by enabling a computer to detect such manipulations of a stylus and use them to govern applications run on the computer. -
Wii U Fun Center Operations Manual
Wii U Fun Center Operations Manual 100425-E Note: Fun Centers have been rebranded as Starlight Gaming stations. Your device will still refer to “Fun Center.” Any in-person reference to “Gaming station” also refers to this product. 100425-E Do you need assistance? Visit www.starlight.org/gaming/support/contact for contact information For immediate assistance during the business hours of 6:00 AM to 4:00 PM PST Monday-Friday please call the Gaming station (Fun Center) Support Hotline at 1-877-716-8550 or email [email protected] FEDERAL COMMUNICATIONS COMMISSION (FCC) COMPLIANCE INFORMATION Note This equipment has been tested and found to comply with the limits for a Class A digital device, pursuant to Part 15 of the FCC Rules. These limits are designed to provide reasonable protection against harmful interference when the equipment is operated in a commercial environment. This equipment generates, uses, and can radiate radio frequency energy and, if not installed and used in accordance with the instruction manual, may cause harmful interference to radio communications. Operation of this equipment in a residential area is likely to cause harmful interference in which case the user will be required to correct the interference at his own expense. Any changes or modifications not expressly approved by the party responsible for compliance could void the user’s authority to operate the equipment. Starlight Fun Center unit support: Phone: 877.716.8550 Website: starlight.nintendo.com Email: [email protected] © 2014-2015, 2016 Nintendo Manufactured by Nintendo of America Inc. Headquarters are in Redmond, Washington Starlight®, Fun Center®, and the boy reaching for the star logo are registered trademarks of Starlight Children’s Foundation®. -

Chapter 3 Input Devices
CSCA0201 FUNDAMENTALS OF COMPUTING Chapter 3 Input Devices 1 Input Devices Topics: • Input Devices • Examples of Input Device • Keyboard • Pointing Devices • Graphic and Video Input Devices • Audio Input Devices 2 Input Devices Input Devices • Any peripheral (piece of computer hardware equipment) used to provide data and control signals to a computer. • Allows the user to put data into the computer. • Without any input devices, a computer would only be a display device and not allow users to interact with it. 3 Input Devices Examples of Input Device • Keyboard • Mouse • Touchscreen • Graphic tablet • Microphone • Scanner 4 Input Devices Keyboard • One of the primary input devices used with a computer. • The keyboard looks very similar to the keyboards of electric typewriters, with some additional keys. • Keyboards allow a computer user to input letters, numbers, and other symbols into a computer • Uses an arrangement of buttons or keys. • Requires pressing and holding several keys simultaneously or in sequence. 5 Input Devices Keyboard 6 Input Devices Types of Keyboard • Standard • Laptop • Gaming and Multimedia • Thumb-sized • Virtual • Foldable 7 Input Devices Types of Keyboard Standard • Desktop computer keyboards, such as the 101-key US traditional keyboards or the 104-key Windows keyboards, include alphabetic characters, punctuation symbols, numbers and a variety of function keys. 8 Input Devices Types of Keyboard Laptop Keyboard • The laptop computer keyboard is a small version of the typical QWERTY keyboard. • A typical laptop has the same keyboard type as a normal keyboard, except for the fact that most laptop keyboards condense the symbols into fewer buttons to accommodate less space. -

Music Games Rock: Rhythm Gaming's Greatest Hits of All Time
“Cementing gaming’s role in music’s evolution, Steinberg has done pop culture a laudable service.” – Nick Catucci, Rolling Stone RHYTHM GAMING’S GREATEST HITS OF ALL TIME By SCOTT STEINBERG Author of Get Rich Playing Games Feat. Martin Mathers and Nadia Oxford Foreword By ALEX RIGOPULOS Co-Creator, Guitar Hero and Rock Band Praise for Music Games Rock “Hits all the right notes—and some you don’t expect. A great account of the music game story so far!” – Mike Snider, Entertainment Reporter, USA Today “An exhaustive compendia. Chocked full of fascinating detail...” – Alex Pham, Technology Reporter, Los Angeles Times “It’ll make you want to celebrate by trashing a gaming unit the way Pete Townshend destroys a guitar.” –Jason Pettigrew, Editor-in-Chief, ALTERNATIVE PRESS “I’ve never seen such a well-collected reference... it serves an important role in letting readers consider all sides of the music and rhythm game debate.” –Masaya Matsuura, Creator, PaRappa the Rapper “A must read for the game-obsessed...” –Jermaine Hall, Editor-in-Chief, VIBE MUSIC GAMES ROCK RHYTHM GAMING’S GREATEST HITS OF ALL TIME SCOTT STEINBERG DEDICATION MUSIC GAMES ROCK: RHYTHM GAMING’S GREATEST HITS OF ALL TIME All Rights Reserved © 2011 by Scott Steinberg “Behind the Music: The Making of Sex ‘N Drugs ‘N Rock ‘N Roll” © 2009 Jon Hare No part of this book may be reproduced or transmitted in any form or by any means – graphic, electronic or mechanical – including photocopying, recording, taping or by any information storage retrieval system, without the written permission of the publisher. -

Download Full Article
Vol. 14, Issue 4, August 2019 pp. 201–223 A Comparison Study of the Smartphone Gaming Control Sang-Duck Seo Abstract Associate Professor University of Nevada, Las Digital technologies have changed human behavior, Vegas especially the characteristics of products and their Las Vegas, NV functionalities related to interface and interaction. USA Smartphone users had to accept touchscreen interfaces [email protected] without sufficient evidence of the effectiveness of these Sunghyun Kang digital interfaces over physical analog interfaces. Moreover, Professor smartphone gaming industries have introduced mobile Iowa State University games with touch-based interfaces that may or may not be Ames, IA effective for game users. This study aims to find empirical USA [email protected] evidence for the effectiveness between analog and digital interfaces for smartphone game controls through two usability tests: (a) a pilot study to compare the data values between direct and indirect input control with six participants and (b) a main study to investigate the effects of tap-only afford between digital and analog input control from the results of the pilot study. Both qualitative and quantitative research methods were used to analyze the usability test. A total of 81 participants were enrolled in the main study and divided into two large groups to compare one-handed and two-handed input controls. Nine participants in each group played smartphone games that were based on different input control tasks. This study found that direct touchscreen interaction was more effective for two-handed input control tasks and indirect physical input control was more effective for one-handed input control tasks.