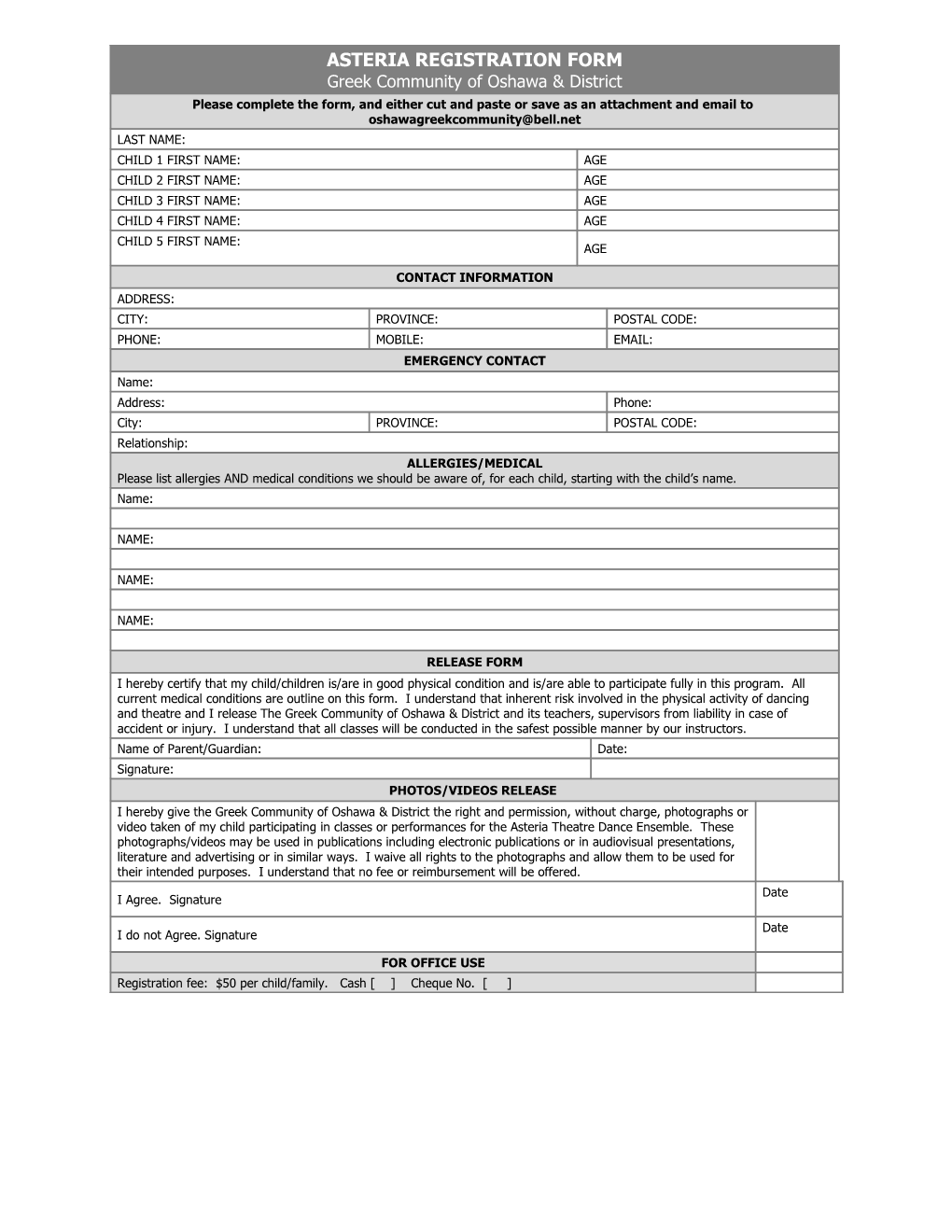
ASTERIA REGISTRATION FORM Greek Community of Oshawa & District Please complete the form, and either cut and paste or save as an attachment and email to [email protected] LAST NAME: CHILD 1 FIRST NAME: AGE CHILD 2 FIRST NAME: AGE CHILD 3 FIRST NAME: AGE CHILD 4 FIRST NAME: AGE CHILD 5 FIRST NAME: AGE
CONTACT INFORMATION ADDRESS: CITY: PROVINCE: POSTAL CODE: PHONE: MOBILE: EMAIL: EMERGENCY CONTACT Name: Address: Phone: City: PROVINCE: POSTAL CODE: Relationship: ALLERGIES/MEDICAL Please list allergies AND medical conditions we should be aware of, for each child, starting with the child’s name. Name:
NAME:
NAME:
NAME:
RELEASE FORM I hereby certify that my child/children is/are in good physical condition and is/are able to participate fully in this program. All current medical conditions are outline on this form. I understand that inherent risk involved in the physical activity of dancing and theatre and I release The Greek Community of Oshawa & District and its teachers, supervisors from liability in case of accident or injury. I understand that all classes will be conducted in the safest possible manner by our instructors. Name of Parent/Guardian: Date: Signature: PHOTOS/VIDEOS RELEASE I hereby give the Greek Community of Oshawa & District the right and permission, without charge, photographs or video taken of my child participating in classes or performances for the Asteria Theatre Dance Ensemble. These photographs/videos may be used in publications including electronic publications or in audiovisual presentations, literature and advertising or in similar ways. I waive all rights to the photographs and allow them to be used for their intended purposes. I understand that no fee or reimbursement will be offered. Date I Agree. Signature
Date I do not Agree. Signature
FOR OFFICE USE Registration fee: $50 per child/family. Cash [ ] Cheque No. [ ]