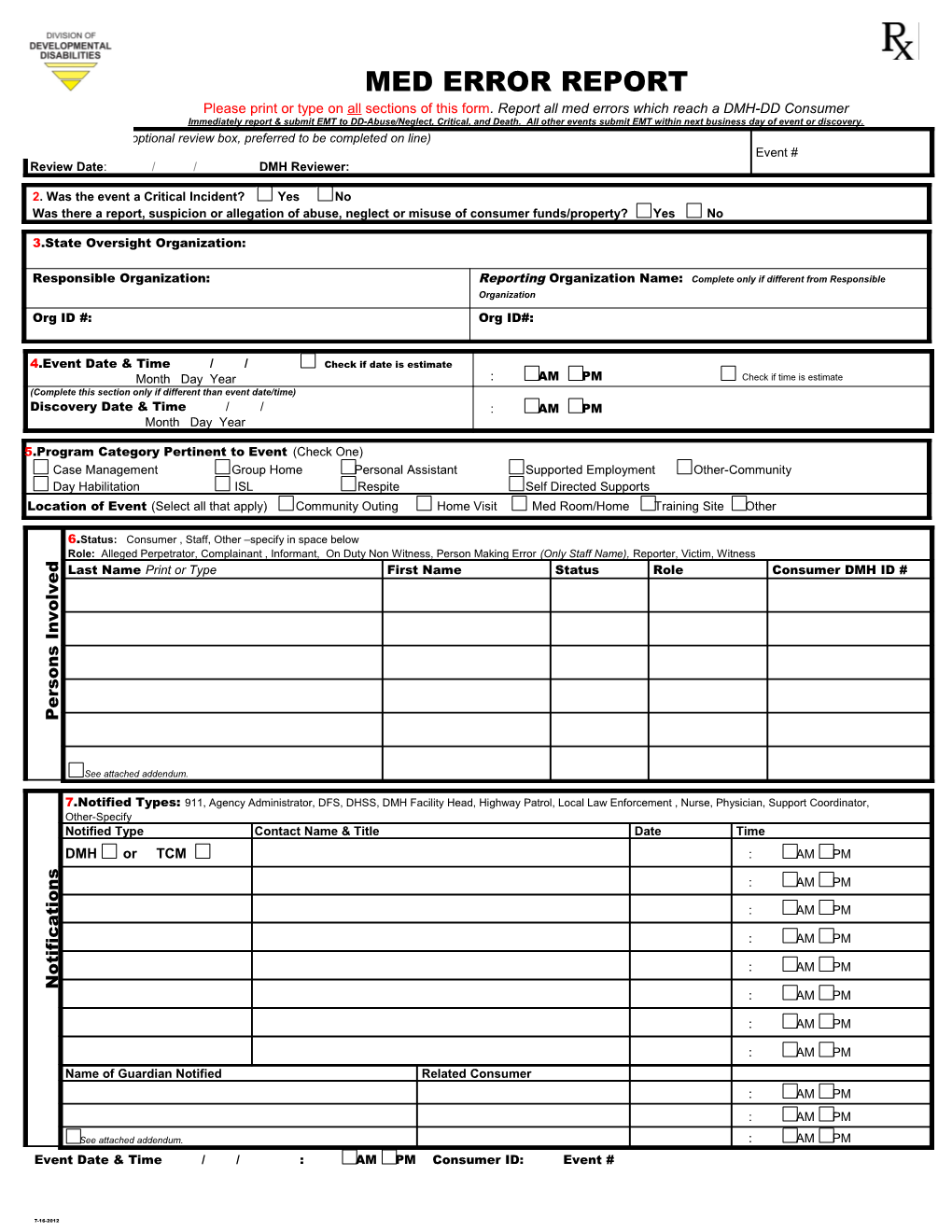
MED ERROR REPORT Please print or type on all sections of this form. Report all med errors which reach a DMH-DD Consumer Immediately report & submit EMT to DD-Abuse/Neglect, Critical, and Death. All other events submit EMT within next business day of event or discovery. 1.DMH Use Only (optional review box, preferred to be completed on line) Event # Review Date: / / DMH Reviewer:
2. Was the event a Critical Incident? Yes No Was there a report, suspicion or allegation of abuse, neglect or misuse of consumer funds/property? Yes No
3.State Oversight Organization:
Responsible Organization: Reporting Organization Name: Complete only if different from Responsible Organization Org ID #: Org ID#:
4.Event Date & Time / / Check if date is estimate Month Day Year : AM PM Check if time is estimate (Complete this section only if different than event date/time) Discovery Date & Time / / : AM PM Month Day Year
5.Program Category Pertinent to Event (Check One) Case Management Group Home Personal Assistant Supported Employment Other-Community Day Habilitation ISL Respite Self Directed Supports Location of Event (Select all that apply) Community Outing Home Visit Med Room/Home Training Site Other
6.Status: Consumer , Staff, Other –specify in space below Role: Alleged Perpetrator, Complainant , Informant, On Duty Non Witness, Person Making Error (Only Staff Name), Reporter, Victim, Witness
d Last Name Print or Type First Name Status Role Consumer DMH ID # e
v
l o
v
n I
s
n o
s r e P
See attached addendum.
7.Notified Types: 911, Agency Administrator, DFS, DHSS, DMH Facility Head, Highway Patrol, Local Law Enforcement , Nurse, Physician, Support Coordinator, Other-Specify Notified Type Contact Name & Title Date Time DMH or TCM : AM PM
s : AM PM n o i
t : AM PM a c
i : AM PM f i t : AM PM o N
: AM PM
: AM PM
: AM PM
Name of Guardian Notified Related Consumer : AM PM : AM PM
See attached addendum. : AM PM Event Date & Time / / : AM PM Consumer ID: Event #
7-16-2012 Other Other/Supervisor Reporter 10
7-16-2012
.PrintTitleName& Event Description Medication Error
Type)(Print or MedicationNamein Error Error End Date on order) appeartheyas error inmeds (Record only Written Order Physician (Select One) Error Reason (Select One) Error Severity (Select One) Error Category (Select One) Error Type 8 Up: Follow Medical 9
.Print or -Type.Print .Individual’s .Individual’s Name:
Seeaddendumattached for meds additional in error. see attached see addendum additional for description
Date: Describe med error Describemed& up action.follow
Optional- attached & Optional- see medsorder only.physician in indicate error Give to Forgot Complex Administration Serious: Moderate: Minimal: Dose Wrong Error Error in Transcription ConsumerAvailable Not AdministertoFailure Other: Other:
Prescribing Dispensing
Time: Time: -when a combination of error type occur (administration, occurdispensing, prescribing) error of type combination -when a Life threatening and/or permanent adverse consequencesadverse permanentand/or Life threatening No treatment or intervention other than monitoring intervention or monitoring than observation treatment or other No /Dosage/Form Treatment and/or interventions in addition to or monitoring to observation ininterventions and/or addition Treatment - - when there is an incorrect selection and a med is given/not given, in the wrong dosage, form, quantity, route, etc. route, form, dosage, quantity, given, isgiven/notthe med wrong ain whenis an -incorrect selection and there - Physician,- incorrectselection drug, form,of dosage, etc,quantity, orroute, for use instructionsa of are drug ordered.wrongly
Pharmacy,when incorrect drug,the dosage, form, concentration, isformulatedquantityand provided foruse. : :
AM AM Medication Not AvailableMedication Not Consumer Given Wrong to Incorrect Dose CalculatedIncorrect PM (Use only if different from Event Date andif different from Event Date Time.) only(Use Signature
Wrong MedicationWrong Form Wrong
New Order NewOverlooked Order Flagged NewNot Mislabeled wasnot individual)given to Amount given (0-if med Quantity
Wrong RouteWrong PersonWrong Date Time No Order Physician Stated AllergyStated Correctly ReadNot : : :
times error did the occur? How many Variances
Other Wrong Time Wrong AM AM AM AM consecutive
PM PM PM _