Comparison on intracochlea disturbances between drilling a manual and robotic cochleostomy Zoka Assadi M, Du X, Dalton J Henshaw S, Coulson CJ, Reid AP, Proops DW, Brett PN , [email protected] 1. Brunel Institute for Bioengineering, Brunel University, Uxbridge, UB8 3PH, U.K. 2. Cochlear Ltd. Australia. 3. ENT department, Queen Elizabeth Hospital, Birmingham, U.K.
Abstract: In hearing preservation cochlear implantation (HPCI), it is considered that minimizing disturbances in hearing organ are likely to reduce trauma and protection of the underlying endosteal membrane of the cochlea is an important factor in cochleostomy formation. The robotic micro-drill system tested in this paper is the first example of an autonomous surgical drill successfully producing a cochleostomy, which keeps the underlying endosteal membrane intact. This study compares induced vibrations within the cochlea during formation of the cochleostomy between using the robotic micro-drill and conventional manual drilling. The vibration of the endosteal membrane is measured using a Microscope Scanning Vibrometer (MSV) at a third window, produced in the cochlea. Results show that the highest velocity amplitude measured was associated with the manual drilling. The robotic micro-drill produced only about 1% of the peak velocity amplitude seen in manual drilling and exhibited much more uniform behaviour, while keeping the underlying membrane intact. The technique applied when using the robotic drill could be a major step in reducing the trauma to the cochlea, by reducing disturbance levels.
Key Words: Robotic micro-drill, Cochleostomy, Vibration, Microscope Scanning Vibrometer
1. Introduction
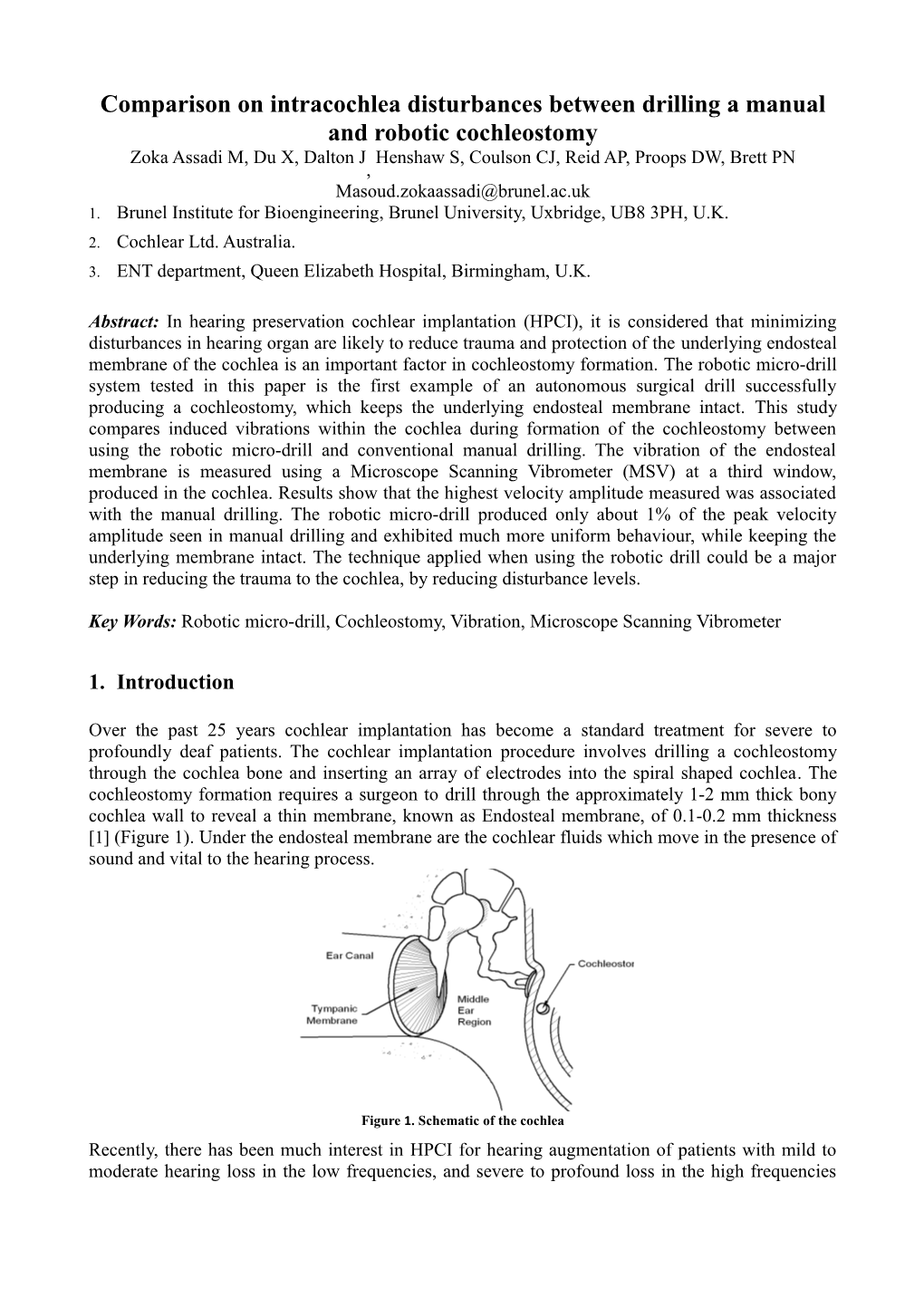
Over the past 25 years cochlear implantation has become a standard treatment for severe to profoundly deaf patients. The cochlear implantation procedure involves drilling a cochleostomy through the cochlea bone and inserting an array of electrodes into the spiral shaped cochlea. The cochleostomy formation requires a surgeon to drill through the approximately 1-2 mm thick bony cochlea wall to reveal a thin membrane, known as Endosteal membrane, of 0.1-0.2 mm thickness [1] (Figure 1). Under the endosteal membrane are the cochlear fluids which move in the presence of sound and vital to the hearing process.
Figure 1. Schematic of the cochlea Recently, there has been much interest in HPCI for hearing augmentation of patients with mild to moderate hearing loss in the low frequencies, and severe to profound loss in the high frequencies [2]. The sensitivity to pressure disturbances within the fluid endosteal lumen of the cochlea during cochleostomy is considered an important factor in hearing preservation [3]. There are two main factors which can lead to further loss of hearing of the patient during the formation of a cochleostomy: First is the mechanical and noise induced trauma during the drilling process [4, 5]; Second is the rupturing of the endosteal membrane by the running burr that can cause serious damage by inducing large pressure disturbances, and destroy hair cells. Currently cochleostomy formation is performed by hand, with the endosteal membrane being perforated by the drill in over 60% of cases [6]. Lenhardt suggests the ideal way to minimize trauma during cochleostomy formation is to preserve the underlying endosteal membrane, which is subsequently opened with a pick rather than a running burr. This method avoids introducing a running burr into the cochlear space [7].
The robotic micro-drill system tested in this paper is the first autonomous surgical robot applied successfully in the operating room for preparing cochleostomies [8]. The system allows information about the state of the drilling process to be derived from force and torque data from the tool point. The system allows force and torque transient of the drilling process to be derived using data from the tool point. This information can be used to effectively predict drill breakthrough and to implement a control strategy to minimise drill penetration beyond the far surface [9]. This unique breakthrough detection feature is significant to produce consistent third windows onto the bony wall of the cochlea.
The definition of the term dynamic disturbance in this paper is the movement of the cochlear endosteal membrane viewed through a third window, made in the cochlea. This movement is presented as velocity amplitude, and is a direct representation of cochlea fluid pressure. High velocity of membrane displacement reflects greater pressure changes within the perilymph, located in the scala tympani and hence a greater potential trauma. However it should be stated that whilst the technique shows the contrasting disturbance transients induced during the cochleostomy formation procedure, it does not provide an absolute measurement of pressure amplitude.
2. Methods and measurements
To contrast pressure disturbances in manual and robotic drilling of a cochleostomy, the investigation focused on a porcine system, as there are physical similarities in size [10]. The drilling process of the robotic micro-drill produces a consistent membrane window onto the fluid as a third window (TW) that was then used to form an assessment of disturbance amplitude. A schematic configuration of the equipment used in the experimental measurement is shown in Figure 2. Figure 2. Schematic diagram of the experimental configuration for measurement. The vibrations of the endosteal membrane at the TW is measured using a Microscope Scanning Vibrometer (MSV) in conjunction with a microscope. The location of the TW is represented with respect to round window (RW). 2.1 Experimental setup For each trial the porcine head was dissected into two halves and the brain was removed. The cochlea is located within the temporal bone underneath the dura mater. The dura was elevated using a surgical knife and Adson forceps, revealing the cochlea, which was extracted from the temporal bone with the stapes still attached and intact. The cochlea was subsequently fixed into a custom built test bed capable of fitting on the microscope. Then using two screws on the sides, the cochlea remained stationary during the experiment. A third window of 0.8 mm diameter was created at the far anterior aspect of the basal turn of the cochlea, approximately 9 mm directly anterior from the anterior lip of the round window niche (Figure 3). To respect the closed fluid structure of the cochlea and provide an accurate measurement of membrane deflection during the drilling process, the endosteal membrane in the TW was visually inspected and palpated and found to be intact after bone removal.
Figure 3. Third window (TW) created at 9 mm anterior from the anterior lip of the round window (RW). The underlying endosteal membrane is intact. The actual surface of the cochlea is hemespherical, however due to the angle and magnification of the camera the cochlea surface appears planar. As the reflection coefficient of the endosteal membrane is extremely low, approximately 0.0039_0.033% [11], 0.01mL of silver metallic paint was applied onto the endosteal membrane to be focused on by the Laser Vibrometer. Paint was applied immediately prior to measurement to avoid any chemical interaction with the properties of the membrane. The test bed was then mounted on the microscope with that the third window oriented at the top of the cochlea test bed and facing the lens of the microscope. The laser spot of the Laser Vibrometer (MSV-400) was focused onto surface of the metallic paint at the measurement point, through the Zeiss 10x/0.3 NA lens of the microscope as shown in Figure 2. 2.2 Manual and robotic drilling procedure Drilling was performed anterior inferior to the round window, in the typical position for a cochleostomy during the cochlear implant procedure. Six cochleostomies were performed on separate porcine cochleas, 3 in the manual group and 3 in the robotic group. The manual cochleostomies were performed by a skilled ENT surgeon, using a 1 mm diamond paste burr at a speed of 10,000 revs/min. At completion of cochleostomy, to assess the disturbances caused by introducing a running burr into the scala tympani, no attempt was made to preserve the underlying endosteal membrane. The surgeon applied a similar force of drilling to that used during human cochlear implantation, although this force was not specifically assessed at this stage. The surgeon was wearing a pair of surgical loupes (SurgiTel EV250) in this process to inspect the correct position of drilling. Figure 4 represents the experimental setup of the manual cochleostomy drilling. The hand of the surgeon was supported by a robust arm rest to avoid undesired hand movement.
Figure 4. Drilling manually on the cochlea while it is in the holder plate under a microscope The robotic cochleostomy was performed using the robotic micro-drill, attached to a snake arm. The arm was locked to the microscope table. Cochleostomies were created with preservation of the endosteal membrane, inherent with the use of this robotic drill. The same drill burr as in the manual tests was used (1 mm diamond); at a drilling speed of 700 rev/min. Figure 5 demonstrates the position of the drill burr with respect to the cochlea. As can be observed in the figure, the robotic drill is being supported by a snake arm. The robotic drilling arm was manoeuvred into the precise location for cochleostomy drilling by the surgeon. The setup time for the robotic drill was approximately 2 minutes. The direction and angle of drilling achieved through the posterior tympanotomy was similar to that of a conventional cochleostomy formation, with an adequate view of the drilling site. The axial drill force was limited to 2 N to ensure that the underlying membrane was not perforated when the burr drilled through the cochlear bone. Irrigation was used throughout all drilling procedures. Figure 5. Robotic drilling of the cochlea while it is in the holder plate under a microscope
3. Result
During the experimental investigations, membrane velocity measured by the MSV was logged with the settings of mm/sv, lines (Time) and 1.28 kHz sample frequency. This data was processed using the Signal Possessing Toolbox of Matlab. The contrasting response caused by manual and robotic cochleostomies, can be seen using plots of velocity transients of the endosteal membrane. Figure 6 shows velocity amplitudes of the third window membrane caused by the manual drilling. The maximum velocity during the manual drilling is approximately 1 m/s. The membrane Breakthrough (BT) point, when the drill burr breaks through the membrane is indicated on the graph. The stationary periods indicated by periods of zero velocity correspond with the surgeon to removing the drill to irrigate the drilling area.
Figure 6. Disturbance of the endosteal membrane, while creating a manual cochleostomy. Breakthrough (BT) point in indicated For robotic cochleostomies, velocity amplitude transients of the third window membrane were recorded over 250 seconds and are shown in Figure 7. The period for the three separate trials shown are 200secs, 170secs and 140secs respectively. The time taken to drill each cochlea to detection of the tissue interface varied according to cochlea thickness. In all three trials the robotic drilling process preserved the endosteal membrane. This was detected by visual inspection during palpation.
Figure 7. Disturbance of the endosteal membrane, while creating a robotic cochleostomy To contrast disturbance amplitude induced within the cochlea by manual and robotic approaches to drilling, three typical series of transients are plotted in figure 8 at the same scale for velocity amplitude. The time axis is shorter for manual drilling as the process is completed in this shorter period. It will be noted that there is significantly lower peak amplitude of disturbance in robotic drilling, approximately 1% of that induced during manual drilling. It will be observed that transients shown for manual drilling are not as uniform as the case of robotic drilling, as there is impact with each sweep of the drill in the manual technique.
Figure 8. Comparison of disturbance of the endosteal membrane at robotic (right) and manual (left) cochleostomy formation
4. Discussion This study compares endosteal membrane disturbance during manual and robotic cochleostomy formation. This study is, to the authors’ knowledge, the first measurement of endosteal membrane movement using Microscope Laser Vibrometer during the drilling of a cochleostomy. Whilst there was an expectation for the robotic micro-drill to cause lower disturbance level to the cochlea, the magnitude of the contrast was not expected. As can be observed from Figure 9, the mean membrane velocity during robotic drilling is 4% of the velocity when drilled manually. Furthermore, peak membrane velocity during the robotic cochleostomy is 1% of that observed during manual drilling.
Figure 9. The mean value of the disturbance for manual and robotic cochleostomies The results of the statistical t-test demonstrated that the two-tailed P value is less than 0.0001, between the responses at the robotic and manual drilling and by conventional criteria this difference is considered to be extremely statistically significant. It is concluded that by controlling the force in robotic drilling it is possible to produce significantly lower disturbances. To support the hypothesis of the effect of drilling speed and force on disturbance velocity amplitude, trials of drilling with three different feed forces of 0.5, 1 and 5 N with a constant speed of 10000 rev/min was performed manually on a cochlea. Figure 10 shows two graphs to illustrate the relationship of the drilling force applied and corresponding disturbance amplitude. The top graph shows disturbance velocity as a function of time and the lower graph shows the corresponding drilling force as a function of time. As can be observed, the highest disturbance occurs when drilling was performed with an applied force of 5 N, with amplitude response at approximately 0.8 m/s. The graph indicated that pressure disturbances created in the cochlea increase with applied feed force.
Figure 10. The relation of the applied drilling force (below) and corresponding disturbance (above) It can be inferred that controlling interactive force is key to reducing disturbance amplitude during the cochleostomy formation process. The robotic micro-drill is able to ensure that a constant feed force is applied from the burr to the bone at all times. This is achieved by controlling linear displacement of the robot where the drill advances or withdraws in response to the feedback depending on drilling characteristics. Manual drilling usually involves impact between the drill burr and the tissue, one with each sweep of the bone surface. On each sweep, the burr will move away from the bone, but will also rebound, leading to an increase in the force applied into the bone. As bone is removed, the forces continually change and these forces are out of the range of the human operator to sense and control. Figure 11 shows the drilling angle in manual and robotic drilling. In manual drilling, the burr is held at a slight angle so that the surgeon has a view of the target area to avoid inadvertent penetration of the underlying membrane. Irrigation is constantly performed through to the tip of the burr and often, the surgeon must remove the burr to allow the liquid to be suctioned out and the drilling site to be inspected. The inspection assesses the integrity endosteal membrane. The sweep of the drill burr and the impact of the tip after each inspection are the major factors leading to spikes in the force delivered to the cochlea during manual drilling. However in the robotic drilling, the burr is held perpendicular to the drilling site. The burr is constantly irrigated with no need of the burr to be moved from the target area.
Figure 11. Drilling angle in manual and robotic drilling. In the robotic drilling, the burr is held perpendicular, however in the manual drilling the burr is held at a slight angle to the cochlear bone The most important aspect of the robotic cochleostomy is breakthrough detection. This feature controls bone drilling to stop just before the endosteal membrane is reached, resulting in the preservation of the membrane. Lenhardt [7] recommends the ideal way to minimize trauma during cochleostomy formation is to perform a bony cochleostomy preserving the underlying endosteal membrane. In this method the membrane is subsequently opened with a pick rather than a running burr as used in the manual drilling method. This method avoids introducing a running burr into the scala tympani. A previous study by Pau has shown that the highest sound pressure level within the cochlea occurs when a running burr touches the endosteal membrane [4]. Prevention of this condition is an achievement with potentially benefit for patients.
5. Conclusion Drilling a cochleostomy in cochlear implantation may cause disturbances of the endosteal membrane that can lead to permanent damage of residual cochlear function. In the current practice of manual drilling, the cochlea may be subject to trauma due to rupturing the endosteal membrane by the running burr. The use of the robotic micro-drill system proposed in this paper will minimise the disturbance to the cochlea by controlling the state of the process of tissue interaction to decrease applied drilling force. As a result the perforation of the endosteal membrane to preserve residual hearing will be prevented.
Reference 1. Doden, E. and R. Halves, On the functional morphology of the human petrous bone. American Journal of Anatomy, 1984. 169(4): p. 451-462. 2. Roland, P.S., W. Gstöttner, and O. Adunka, Method for hearing preservation in cochlear implant surgery. Operative Techniques in Otolaryngology-Head and Neck Surgery, 2005. 16(2): p. 93-100. 3. Zoka Assadi, M., X. Du., P.N. Brett, D. Proops, A. Reid and C. Coulson, Contrasting disturbance levels within a cochlea., in Southern Region Engineering Conference. 2010, University of Southern Queenland: Toowoomba, Australia. 4. Pau, H., T. Just, M. Bornitz, N. Lasurashvilli, and T. Zahnert, Noise exposure of the inner ear during drilling a cochleostomy for cochlear implantation. The Laryngoscope, 2007. 117(3): p. 535-540. 5. Zou, J., P. Bretlau, I. Pyykkö, J. Starck, and E. Toppila, Sensorineural hearing loss after vibration: an animal model for evaluating prevention and treatment of inner ear hearing loss. Acta oto-laryngologica, 2001. 121(2): p. 143-148. 6. Coulson, C., Reid, D.W. Proops and P.N. Brett, ENT challenges at the small scale. The International Journal of Medical Robotics and Computer Assisted Surgery, 2007. 3(2): p. 91- 96. 7. Lehnhardt, E., Intracochlear placement of cochlear implant electrodes in soft surgery technique. Hno, 1993. 41(7): p. 356. 8. Brett, P., R.P. Taylor, X. Du, D. Proops, M.W. Griffiths and C. Coulson, A Smart Generic Micro-drilling Tool Applied In Cochleostomy. 2009: Springer. 9. Coulson, C., R.P. Taylor, A.P. Reid, M.W. Griffiths, D.W. Proops and P.N. Brett, An autonomous surgical robot for drilling a cochleostomy: preliminary porcine trial. Clin Otolaryngol, 2008. 33(4): p. 343-347. 10. Pracy, J.P., A. White, Y. Mustafa, D. Smith and M.E. Perry, The comparative anatomy of the pig middle ear cavity: a model for middle ear inflammation in the human? Journal of Anatomy, 1998. 192(03): p. 359-368. 11. Khanna, S.M., J.F. Willemin, and M. Ulfendahl, Measurement of optical reflectivity in cells of the inner ear. Acta oto-laryngologica. Supplementum, 1989(467): p. 69-75.