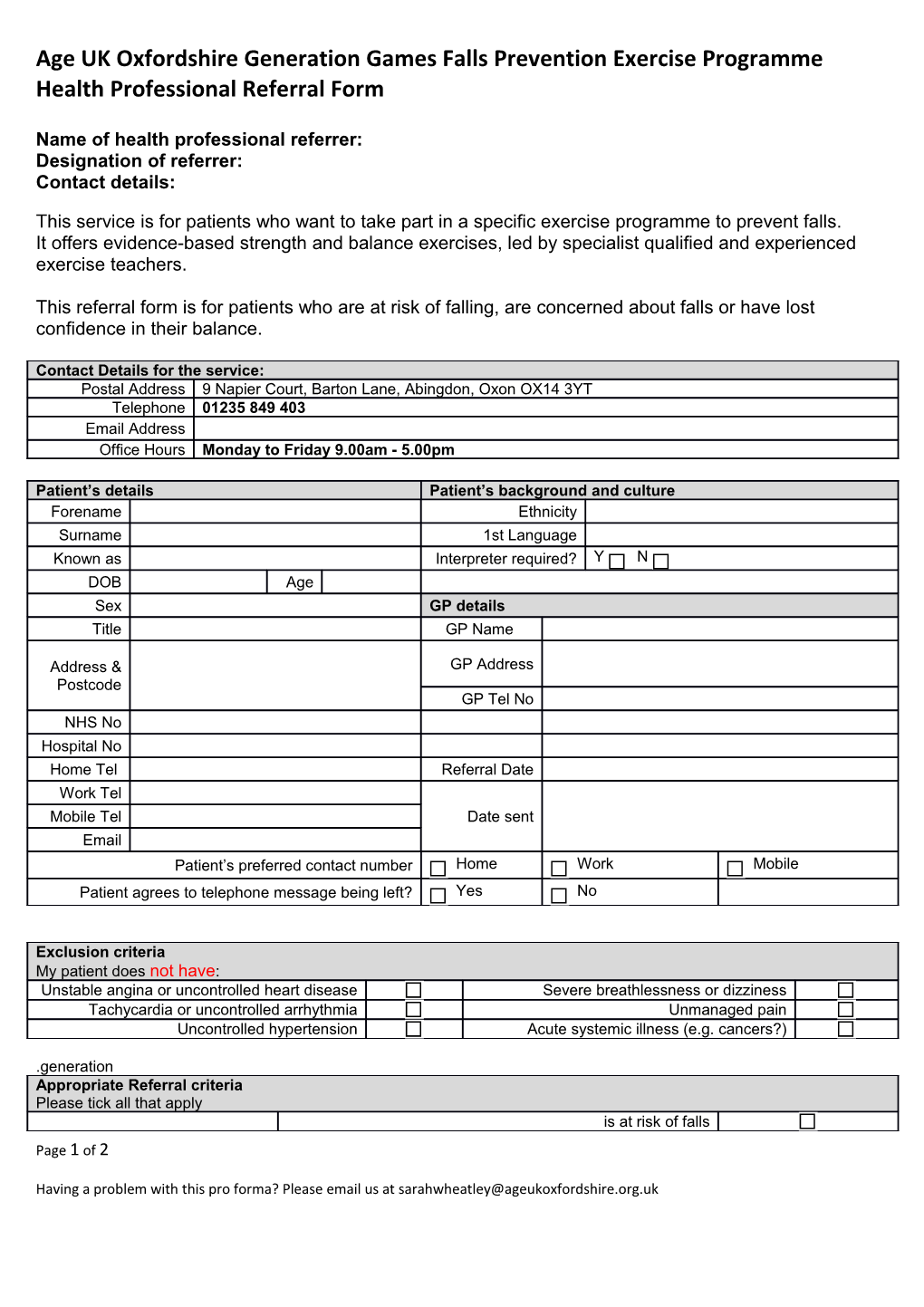
Age UK Oxfordshire Generation Games Falls Prevention Exercise Programme Health Professional Referral Form
Name of health professional referrer: Designation of referrer: Contact details:
This service is for patients who want to take part in a specific exercise programme to prevent falls. It offers evidence-based strength and balance exercises, led by specialist qualified and experienced exercise teachers.
This referral form is for patients who are at risk of falling, are concerned about falls or have lost confidence in their balance.
Contact Details for the service: Postal Address 9 Napier Court, Barton Lane, Abingdon, Oxon OX14 3YT Telephone 01235 849 403 Email Address Office Hours Monday to Friday 9.00am - 5.00pm
Patient’s details Patient’s background and culture Forename Ethnicity Surname 1st Language Known as Interpreter required? Y N DOB Age Sex GP details Title GP Name
Address & GP Address
Postcode GP Tel No NHS No Hospital No Home Tel Referral Date Work Tel Mobile Tel Date sent Email Patient’s preferred contact number Home Work Mobile Patient agrees to telephone message being left? Yes No
Exclusion criteria My patient does not have: Unstable angina or uncontrolled heart disease Severe breathlessness or dizziness Tachycardia or uncontrolled arrhythmia Unmanaged pain Uncontrolled hypertension Acute systemic illness (e.g. cancers?)
.generation Appropriate Referral criteria Please tick all that apply is at risk of falls Page 1 of 2
Having a problem with this pro forma? Please email us at [email protected] Age UK Oxfordshire Generation Games Falls Prevention Exercise Programme Health Professional Referral Form is concerned about balance The patient … has lost confidence has had one or more non-injurious falls in the last 12 months Other Please specify: The exercise programme has been discussed with the patient and they are motivated to attend
Narrative of referral letter / additional information: (please highlight any significant comorbidities and relevant investigations) Please tick here if you are sending any additional documents. The referral narrative should be typed below, not in a separate letter
Please send this referral form to [email protected] We will telephone your patient within 5 working days of receiving the form.
Page 2 of 2
Having a problem with this pro forma? Please email us at [email protected]