Vaginitis
The most common causes of vaginitis are Bacterial vaginosis, Candida albicans vaginitis, and Trichomonas vaginalis. Other causes include gonococcal or chlamydial cervicitis, atrophic vaginitis, or contact/irritant vaginitis. Ascertaining pH by touching pH strip to speculum after exam can be very helpful in making diagnosis. If doing both wet prep and KOH, do wet prep first. Some experts think there is no need for KOH except in doing whiff test. Scan slides first on low power then go to high power (10x vs. 40x).
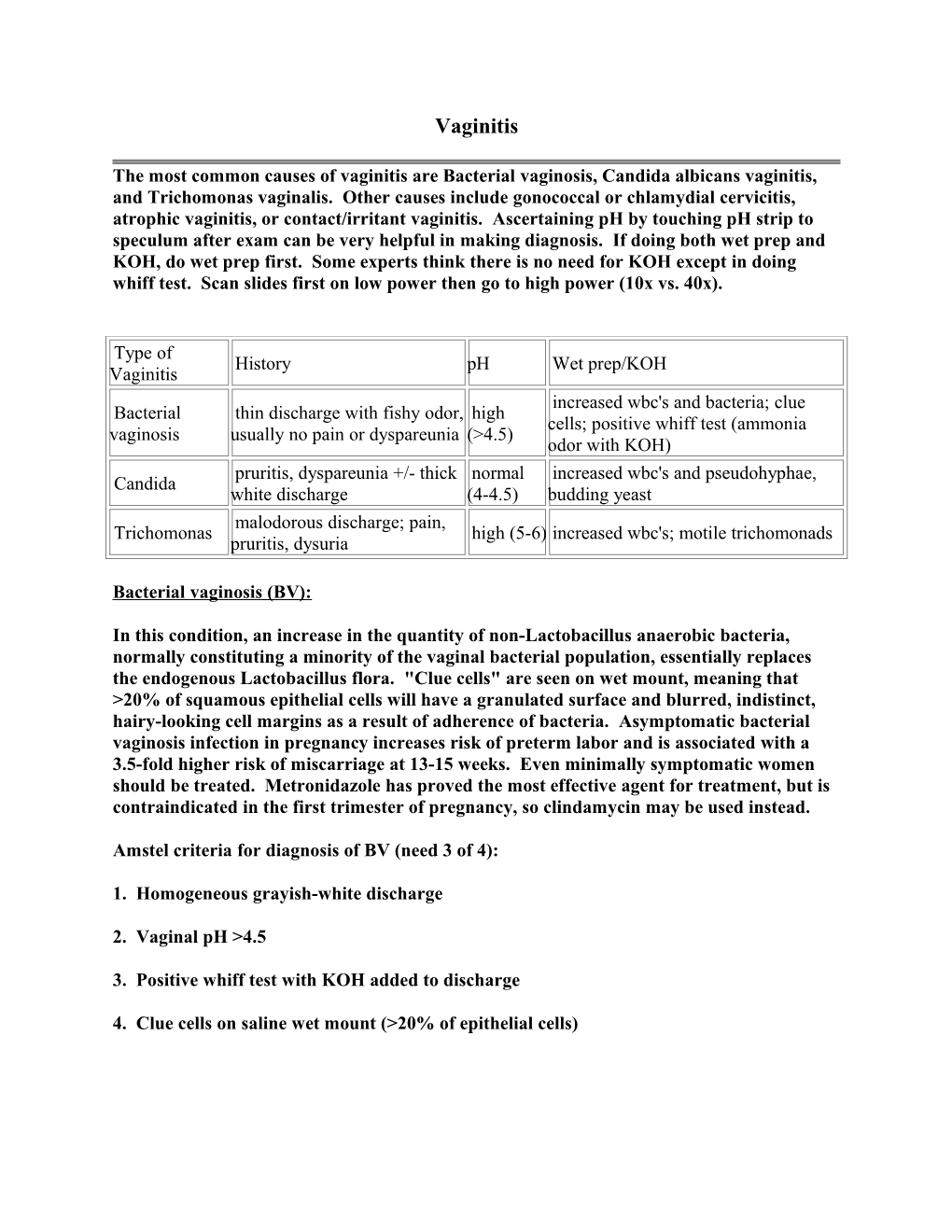
Type of History pH Wet prep/KOH Vaginitis increased wbc's and bacteria; clue Bacterial thin discharge with fishy odor, high cells; positive whiff test (ammonia vaginosis usually no pain or dyspareunia (>4.5) odor with KOH) pruritis, dyspareunia +/- thick normal increased wbc's and pseudohyphae, Candida white discharge (4-4.5) budding yeast malodorous discharge; pain, Trichomonas high (5-6) increased wbc's; motile trichomonads pruritis, dysuria
Bacterial vaginosis (BV):
In this condition, an increase in the quantity of non-Lactobacillus anaerobic bacteria, normally constituting a minority of the vaginal bacterial population, essentially replaces the endogenous Lactobacillus flora. "Clue cells" are seen on wet mount, meaning that >20% of squamous epithelial cells will have a granulated surface and blurred, indistinct, hairy-looking cell margins as a result of adherence of bacteria. Asymptomatic bacterial vaginosis infection in pregnancy increases risk of preterm labor and is associated with a 3.5-fold higher risk of miscarriage at 13-15 weeks. Even minimally symptomatic women should be treated. Metronidazole has proved the most effective agent for treatment, but is contraindicated in the first trimester of pregnancy, so clindamycin may be used instead.
Amstel criteria for diagnosis of BV (need 3 of 4):
1. Homogeneous grayish-white discharge
2. Vaginal pH >4.5
3. Positive whiff test with KOH added to discharge
4. Clue cells on saline wet mount (>20% of epithelial cells) Candida vaginitis:
Familiar predisposing factors include diabetes, AIDS, recent antibiotic use, obesity, birth control pill use, pregnancy, corticosteroids, immunosuppressants, debility, warm weather, and tight clothing. Women will often have vulvar and vaginal irritation resulting in burning, itching, dyspareunia, and dysuria. They will often have a white clumpy discharge. Women with classic vaginal itch who have a history of yeast vaginitis or are at risk (such as from recent antibiotic therapy) may reasonably treat themselves empirically without further testing, but empiric treatment should be avoided under other circumstances. Severe or recurrrent Candida infections require 7-14 day treatment with an azole agent or nystatin. Although KOH slides are often used to dissolve cells and other debris that can obscure fungal forms, yeast can be diagnosed with a plain saline slide. Some women have recurrent candida vaginitis, being plagued by more than 3 episodes per year. Patient self-diagnosis and treatment has been a strategy for this patients, along with attention to predisposing factors.
Trichomonas:
Most infected women complain of discomfort such as pruritus, dyspareunia, or dysuria. "Strawberry cervix" should suggest the diagnosis of TV. Look for motile trichomonad which will be intermediate in size between PMN's and epithelial cells. May see flagellum waving. Treatment is metronidazole. Sexual partners should be treated as well.
References:
Eckert LO. Acute Vulvovaginitis. N Engl J Med 2006;355:1244-52.