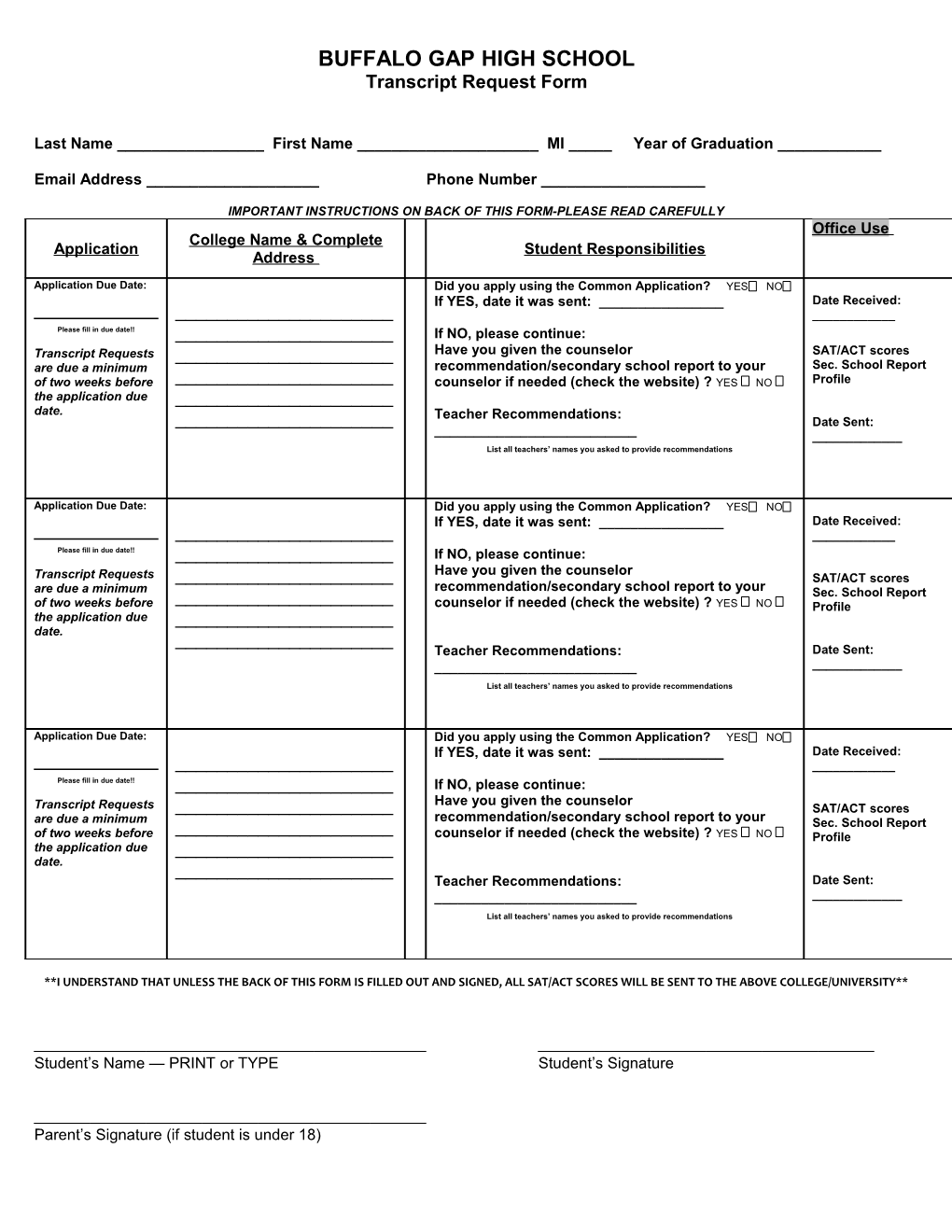
BUFFALO GAP HIGH SCHOOL Transcript Request Form
Last Name ______First Name ______MI _____ Year of Graduation ______
Email Address ______Phone Number ______
IMPORTANT INSTRUCTIONS ON BACK OF THIS FORM-PLEASE READ CAREFULLY Office Use College Name & Complete Application Student Responsibilities Address
Application Due Date: Did you apply using the Common Application? YES NO If YES, date it was sent: ______Date Received: ______Please fill in due date!! ______If NO, please continue: Transcript Requests ______Have you given the counselor SAT/ACT scores are due a minimum recommendation/secondary school report to your Sec. School Report of two weeks before ______counselor if needed (check the website) ? YES NO Profile the application due ______date. Teacher Recommendations: ______Date Sent: ______List all teachers’ names you asked to provide recommendations
Application Due Date: Did you apply using the Common Application? YES NO If YES, date it was sent: ______Date Received: ______Please fill in due date!! ______If NO, please continue: Have you given the counselor Transcript Requests ______SAT/ACT scores recommendation/secondary school report to your are due a minimum ______Sec. School Report of two weeks before counselor if needed (check the website) ? YES NO Profile the application due ______date. ______Teacher Recommendations: Date Sent: ______List all teachers’ names you asked to provide recommendations
Application Due Date: Did you apply using the Common Application? YES NO If YES, date it was sent: ______Date Received: ______Please fill in due date!! ______If NO, please continue: Have you given the counselor Transcript Requests ______SAT/ACT scores recommendation/secondary school report to your are due a minimum ______Sec. School Report of two weeks before counselor if needed (check the website) ? YES NO Profile the application due ______date. ______Teacher Recommendations: Date Sent: ______List all teachers’ names you asked to provide recommendations
**I UNDERSTAND THAT UNLESS THE BACK OF THIS FORM IS FILLED OUT AND SIGNED, ALL SAT/ACT SCORES WILL BE SENT TO THE ABOVE COLLEGE/UNIVERSITY**
Student’s Name — PRINT or TYPE Student’s Signature
Parent’s Signature (if student is under 18) HOLD ALL SCORES I do not want the BGHS Guidance Department to send my SAT and ACT scores to any colleges/ universities. I understand that I will be responsible for having The CollegeBoard (or ACT) send my scores directly to any colleges/universities that I may apply to.
Student Name: ______Signature: ______Date: ______