DW_002_1210_FALLS PREVENTION COM
Good morning everybody, we will be starting here in the next few minutes. I have everybody unmuted, so we can hear everything that is going on, so if you have any talking in the background or any background noise if you could please mute, that will be great unless you have a question and unlike I said we will be starting here shortly.
Okay we will be getting started here shortly, so we went to rehab you on them. We are trying to get our presenter on and it will just take a couple of minutes here. She is on the webinar, but she is not on so she can speak, so I would think it should just take a couple of minutes. Ashley is going to go ahead and give her a call. So, if anybody have any good news as far as their falls program and what they have implemented so far from this community practice.
Okay, there is anybody have anything else this year on what, may be what there working on for quality improvement right now and you all will probably depute the quality lead or if you are not the quality lead and if you are interested then we are starting INR greater than five program and so we did send out as survey on that. Thus we just collect some data and then also to Falls prevention 2 move forward on how this is going to look and I can get the 7:38
INAUDIBLE, but it will be four webinars with coaching for ten hospitals that are interested to follow the webinar, and so if you are interested in that and you are the quality lead, please ask your quality lead about that survey that was sent out, but what we would like to happen is collect some data over the next couple of weeks, respond to the survey and then Brian Isetts our pharmacist will be conducting webinars with some coaching to go along. So that only will you be involved in this, but also one who will be native pharmacist will be involved in the webinars and then we will measure performance after that is finished, that will be very exciting to do that and to get started with that, I know that we had talked about that in August and finally we are getting it off the ground with Dr. Isetts and kind of going in the direction that he would want to go. Once again if he just go get on, we are waiting for Steve Ann whose is presenter to be able to get audio which she can present.
Hello, this is Sue Ann.
Hi Sue Ann, thanks for joining.
Is this Jennifer.
Yes, I am right here, Sue Ann, thank you so much for coming on. Falls prevention 3
Of course, I am sorry for that mix up, I have no idea what was going on, I have actually added different site, I am not in my office, I am on the road, so that might be one of the challenges. Now, are you hearing me clearly or not, how is the audio for you.
Yes, can everybody hear Sue Ann well?
Perfect, well Sue Ann you can see the screen and then you would like me to go to the next screen just to let me know.
Okay fantastic and I have one question quickly, when is your stop time.
Our stop time is 1 o’clock but our webinar usually goes from
11:30 until 12:30.
Okay, so 11:30 to 12:30 and do we want to do questions as I go or questions at the end, what is the preference?
Anybody in the group like to answer that would you like to ask
Sue Ann questions as she goes, would you like her to have a little break and she can ask or would you like that to be at the Falls prevention 4 end. I personally think as you go would probably be a little bit better.
Okay what I can do is just stop as I go on to say are there any questions and we can proceed that way.
That would be wonderful, thank you so much.
Okay, alright, we will get started, lets advance to the first slide, second slide is objective, lets roll over to the third slide. And the third slide essentially is giving a brief background to how it is that I change to doing this webinar today. I work for consortium in Minnesota, 24 skilled nursing facilities. This consortium came together 15 years ago and we are quality improvement organization. We do quality improvement programs based on the research that we do, then we apply that research to program and in 2008, we were given, we were awarded a Federal and State Grant from the Department of Human Services to investigate why resident fall in nursing homes and that was the key. Ultimately 16 skilled nursing homes were given this grant, my largest nursing home is a 486 bed facility and my smallest one is a 55 bed facility and these facilities are all located in Minnesota, and we do skilled independent living as well as assisted living, but the grant was specifically slated Falls prevention 5 for our skilled nursing homes. The goal of the grant again was to determine why residents fall in nursing homes, and so we hire
Dr. Dan Sheridan, who was a national nurse forensic pathologist to taught us how to do an investigation of a fall, what clues are there, essentially what is the evidence that is present at the time of resident falls.
So, he taught us root cause analysis and root cause analysis really is a process to find out what happened, why it happened and to determine what can be done to prevent it from happening again, and it really was the eye opening for us that we now since this program have applied root cause analysis to so many other clinical areas but nevertheless one of the things that he taught us in root cause analysis is that when a resident falls it is considered to be a crime and it is a crime scene and to protect that crime scene for all the clues and the evidence that are there.
And one other thing that he said was that in any crime scene the way he approaches is to first look at what are the environmental extrinsic conditions that resulted in that resident’s falling and as he taught us residents fall because everything was set up perfectly for that fall to occur and he said the environmental conditions were just perfect for that fall to occur, and then he Falls prevention 6 said the internal conditions, internal meaning what is going on inside the resident, what is their diagnoses, what were their vital signs just before they fell, all their needs that set them into motion and those needs obviously were not met because they were moving on those needs. Other internal conditions would be medications what they are on, what is the condition of their internal chemistry so lab results, all of that was examined post fall and then the last one which he said would ultimately be the most important one was operational condition meaning what are the policies and procedures that are in place, how are we running our nursing homes that the result is this exorbitant and tremendous amount of falls that seem to continue to occur in the skilled nursing home, and he said operationally we are set up for that fall to occur. So he really changed the way we looked at falls. He changed a paradigm. I wonder as nursing Jo Smith who said to me every time the resident falls, the first thing I say to myself is what did we do that cause this, how is that their falls now has occurred and it did not occur yesterday at this time, so for instance here we are and it is Tuesday and it is 11:30 in the morning, why did not they fall yesterday on
Monday at 11:30 in the morning, what was going on specific to today and that is really a result of Dan Sheridan saying something was going on today that was not going on yesterday.
There was either more staff, less staff, temporary staff that Falls prevention 7 would be all operational or there was a noisy picnic today and there was not yesterday, so operationally what was going on and then we looked at all of those conditions, what was going on environmentally internally yesterday or internally yesterday they did not take a pain medication and analgesic at breakfast but today they did and so he said every single fall has an underlying determinant. However of course that every fall can be prevented but certainly an investigation of every fall can be done.
And so from the many post fall investigations this is what occurred, a resident would fall, we would do a post fall investigation, report, that report was completed and electronically sent to Empira and we designed a software program that aggregated, collated and summarized all the falls that cause all of our facilities as well as specific to each facility and so our software program very shortly began to determine what were the most popular external conditions at the time resident fall, what was the most popular internal or prevalent internal condition and systematically operationally what was going on in our facilities that was causing a fall. Our software program could breakout this information specific to each facility as well as across the board for all of our facilities and now we have 24 facilities on-board doing this. Here with the results Falls prevention 8 of that program. The results were externally, the most popular conditions externally at the time of resident fell with noise and that one we did not expect or see coming. Ultimately we put sound meters around our buildings and we were able to correlate that high noise times resulted in high fall times, low noise times resulted in low fall times and we were able to correlate that noise was also the condition of busy activity, so if you look at busy activity and noise that is when resident fall and when are the busiest times and activities, well that is systemic conditions of shift change and great time we found to be the most popular fall times. The other external conditions that we identified were a lack of environmental contrast and specifically we looked at doorways, thresholds and toilet seat.
We found that most of our facilities had white or light toilet seats against the white or light floor. Once we put in to our toilet seats we were able to reduce some amount of falls in bathrooms. Thresholds, doorways. We contrasted the molding around the door as well as the door. We contrasted that and so it facilitated easier entrance and exits into rooms. The lack of the placement of resident furniture equipment and personal items now were the resident expects them to be identified. For instance, we were not as diligent as we also have been on asking a resident where would you like your eye glasses, where would you like your bible, where do you usually put your cane when you Falls prevention 9 go to bed at night, your walker when you go to sleep and so we got more diligent in placing things where residents expected them to be, and most importantly what side of the bed do you usually get out at home, do you usually get out of the right side of your bed or the left side and we saw many of our residents would answer, “well, I got out of the left side and we were looking at a resident now in our facility who if they got out of the left side of their bed they would walk into the privacy curtain between them in the bed next to them, and so we really did a lot of work in that area. Internal conditions at the time of fall a resident has a poor balance and we really wanted to know why do they have a poor balance and here was something that startled us and has since changed the entire culture of how we run and operate our nursing homes. We are identified that sleep deprivation or more correctly sleep fragmentation was the underlying systemic cause of almost all of the problems our residents faced. Their poor balance was due to the fact that they were so sleep fragmented they did not have a good steady balance. The other condition causing poor balance medications and the side effects of medications specifically orthostatic blood pressure, a sudden drop in the blood pressure upon rising is a frequent side effect many of the medications our residents take causing poor balance and then endurance in strength again they are so tired, they are so sleep fragmented Falls prevention 10 and deprived, they have no strength or endurance in order to continue to walk or move and so they fall down. The primary systemic cause of the falls are the policy and procedures that we have in place that actually contribute directly to falls, specific some other problems, some other policies and procedures would be interrupting sleep at night, restocking rooms at night, disrupting residents routine during the day because we need to
“run a nursing home” and so the running of the nursing home by interrupting them when they would like to have quiet time so it is one that we identified. We looked at shift changed time, break times. We did identify that some facilities have very specific days of the week that residents fall more often then other days of the week. We did not find a consistent days through all our facilities but rather consistent days within the facility, so some our facilities weekend for a fall times, yet other facilities weekends were pretty good, they did not fall as often. Some facilities identified Mondays and Fridays to be high fall days and yet other facilities Tuesday, Wednesdays were and then once again we did root cause to dwell into why, what are the conditions that are different on a weekend where falls are less or what are the conditions on a weekend that falls occur more. We looked at locations of falls we found that most of the falls occur within the residents room second to that a hallway and then third a 23:13 INAUDIBLE areas. The types of Falls prevention 11 falls, number one are transfers, number two is reaching and stretching to get something. We looked at routine staff assignments and staffing levels. We did not necessarily find that more staff resulted in the less falls but rather which staff were employed and what were they doing at the time of the falls and we also identified that we employed a lot of staff when we really did not need them or let me put that in a better wording, when the residents did need them. We were hiring and employing housekeeping, maintenance before 8 a.m. in the morning and we really do not need them. I know they think they are needed before then because as we heard from maintenance and housekeeping all I have to clean 24:01 INAUDIBLE areas. Yeah, but we really need to hear at 4-5 in the afternoon one more fall are occurring. We looked at activities and social service and said we really do not need them before 10 a.m. in the morning and so we shifted staffing levels, we split staffing levels.
So those were the causes and just so ever briefly some of the outcomes that we did. The biggest take away from our fall program was the external lesson learned and that was if we stop the noise we can reduce the fall. Next slide please and then the most prevalent internal lesson that we learned is that if we can just stop disturbing their sleep then we can reduce falls. Falls prevention 12
So those were big takeaways, the single biggest takeaways from our fall program was the generic systemic way in which we run nursing homes that contributed to falls and here is how we really came to that conclusion. We notice on the MVS the section the mood status change was getting worse and worse as resident stayed in our facilities longer and longer. In another words, their moods worsened, their cognitive changes declined and we were attributing those that declination in their cognitive status to their diagnosis of dementia and we said we will of course that we decline because we do not have a cure for dementia and so it would be understanding that they would decline. We were in high side, a little bit too glue and little bit to dismissive of those conditions being a reason for their cognitive changes. We notice that they napped more, the more that they were in our facilities and they became more agitated, meaning more behavior identified problem, they developed
“behaviors” that then get documented on the MDS and more falls, so all of that we ultimately identified those all had an underlying cause of sleep disturbance and sleep fragmentation and so what we need to say to ourselves is if all of us had our nightly sleep disturbed every two hours how would we appear in six months, two years or even six weeks and I there say our mood status would decline, our cognitive status would be greatly impaired. We would be taking a heck of lot more naps and talk Falls prevention 13 about being very angry and agitated and yes we would be uncoordinated and falling down more, so we went back to the government and we said to the government we have identified the primary systemic cause of falls and internal cause of falls, but we cannot do anything about it because it is the way we run our nursing home. We turn and reposition every two hours, we are doing these assessments that result in disturbing residents sleep at night, we get residents in from the hospital and they are unstable until we are doing vital signs all through the night and so you all know the many reasons on why we disturbing sleep at night to restock incontinent products, to restock personal hygiene products. We disturbed residents at night to draw a blood. The phlebotomist coming into our routine blood at
4-5 a.m. We have contracted vendors that come in and do carpet extraction at night. We have maintenance doing linoleum stripping at night and so we really looked at what is disturbing our residents sleep at night and we thought it is the way we run on nursing home that is why their sleep is disturbed at night and so we went back to the government and said while we have identified a primary operational condition for why residents fall that is sleep disturbance, there is little or nothing that we can do about it, unless you give us another three year grant and so the Fall Prevention Grant ended actually on September 30,
2011 and on October 1, 2011, the very next day we were awarded Falls prevention 14 another three year grant. The goal being to specifically stop disturbing sleep at night, so the goal for the new grant and it was a three year Federal State Grant was to have undisturbed sleep at night that was our number one goal and next slide please and our second goal was to have residents more fully awake and engage during the day. We defended this program to the government by saying that CMS and long-term care providers have never considered sleep as an integral part of the plan of care and services provided to residents. We never and I have now this year I am celebrating my 40th anniversary as a registered nurse and 32 of those years are in the long-term care profession, I have never written a care plan where I said the residents sleep is so poor. I never even knew haw to do a sleep assessment and so part of my professional career reflects a disregard for resident sleep at night as well as CMS and so we went back to CMS the department of human services and we said we need to change that culture, we need to protect sleep at night and so this program is a combination of nationally recognize evidenced based sleep hygiene scientific research study, and the application of the most cutting edge practices to enhance resident sleep.
This program is a combination of nationally recognized evidence-based sleep hygiene scientific research studies and the application of the most cutting edge practices to enhance Falls prevention 15 residents’ sleep. We really educated ourselves on sleep, sleep science, and sleep hygiene and we are challenging some of the standards of practice, operational procedures, and regulatory requirement. We are challenging the way our regulations do not protect our residents’ sleep at night in nursing home. The first thing we have to do we have to learn sleep. We knew little or nothing about sleep. We did not understand the etiology of sleep, and so we at Empira became very astute and much more skilled in sleep wake science. Next slide please.
The biggest thing is that we identified our own sleep deficit or knowledge deficit I should say. We did not know what is the etiology of sleep, how did human beings wake up and go to sleep.
Next slide please. We learn from the international study that sleep has been studied intensively for about the last two decades. It has become much more sophisticated science in the measurement of sleep. I know there are some people listening who have probably gone to sleep labs where you go for an overnight 12-hour study and electrodes are put on the skull to measure brain wave activity, on the eyes to measure eye movement activity. Vital signs are taken throughout the night and then a monitoring device for muscle tonicity how tight a cuff is actually put on the subject’s thigh or upper arm where the measurement of muscle tonicity, how tight is the muscle, how relaxed is the muscle, and all of that information goes into a Falls prevention 16 software program, next slide please, where scientist could actually measure the different stages and cycles of sleep.
Another brand new development is the actogram or the Actiwatch.
The Actiwatch now has been commercially made into a product called FitBit. The FitBit is not anyway near sophisticated as the Actiwatch, but the Actiwatch was designed about seven to eight years ago and it is device worn on the wrist 24/7 and it really helps to identify if you will, the next slide please. It really identifies all of the parameters of sleep. So what happens is our residents we purchase these Actiwatches put them on residents. They were on resident anywhere from four to seven days 24/7, we then took the Actiwatch off, put in on a port on a computer and what was downloaded was a full sleep wake assessment report. For the first time ever, all of our residents had a much more comprehensive sleep wake assessment.
Very briefly what I am showing you there is just a one day 24- hour cycle, a printed cycle of a resident’s activity-inactivity wake sleep program and I really don’t have more time than that to simply save you, to give you an example that we were able to do a very intense sleep wake assessment of all of our residents.
Next slide please. What we were actually looking at measuring it was what time did they go to sleep, what time did they get up, how much time did they actually spend in bed, and when they were in bed, what was their sleep efficiency meaning how much Falls prevention 17 time did they actually sleep while they were in bed. So if they were in bed for 10 hours at night but they only slept 6 hours then they would have had a 60% sleep efficiency. We also started learning about sleep science, sleep latency, how long were they in bed before they actually fell asleep. Many of you probably are aware of the fact that if you go to sleep at night, you are fully exhausted physically. You close your eyes and suddenly your brain turns on and you can’t fall asleep, and so that is a scientific condition called sleep latency or are you one of those people who you can drop off to sleep. That’s not a problem, you fall asleep, but in the middle of the night you wake up and you can’t go back to sleep. It is actually again well identified and documented as WASO (wake after sleep onset).
We were able to measure a light threshold, how much light did they get during the day, how little at night. We measured the frequency and duration of naps and there we are at the last most important one, how often at night is this sleep being disturbed, if you will. Next slide please. What we learn is that all human beings have a circadian rhythm that is an inborn, internal, 24-hour cycle of change and fluctuation within the physiological, behavioral, and emotional functions of the human body. What we actually learned is that we have going on inside our body, next slide please, different changes for which we have little or no control and when you have more time, I would really Falls prevention 18 encourage you to look at the average human biological clock because things go on in our body based on the time of the day.
Because it is 10 o’clock in the morning, I am most alert.
Because it is 9 a.m. in the morning, men are making the highest amount of testosterone they will make in the 24-hour period or because it is 11 o’clock at night, our body stops making a hormone called serotonin and starts making a hormone called melatonin and so none of us got up this morning and said okay its 7 a.m. I better start making some serotonin, we did not do that, but it was being done, but for being done because that would be time of the day.
Can somebody put a sign board, can you please hang up; otherwise just mute that INAUDIBLE 36:44 see if I can figure it out.
I think at another time I would encourage all of you to really take a look at human biological clock of circadian rhythm changes and this is probably 100s of the changes that occur in our body, fluctuations of change that we have little or no control over, but the change is occurring because it is that time of the day, if you will next slide please. We really began to work and investigate the effect of sleep deprivation on the human body and sleep fragmentation on the human body and so that is what this next slide will show you is all of the scientific research that has been done in sleep deprivation and in actually Falls prevention 19 identifying the causation of sleep deprivation on the body. Can
I have the slide changed please, ya, there we go. So that is the scientific investigation into deprivation of sleep on the human body just a few of the effects. Next slide please. One of the things that we also learned is that human beings have a very renowned narrow healthy time window of sleep. All human beings ought to sleep 7 to 8 hours, that would be an ideal healthy system of sleep. I know that many of us sleep only 5 to
6 hours at night and we do function the next day, but all the scientific research reveals that we won’t function as well had we slept 7 to 8 hours. We also for people who sleep less than 6 hours or consistently more than 10 hours of sleep at night will all suffer from a deprivation in longevity. People who consistently sleep for short hours, I need to be so blunt, die sooner. People who have a consistent sleep patterns of less than 6 hours or less will suffer from cardiovascular condition, diabetic, endocrine disease is more often. We also sleep, next slide please, in very specific and this is where all of the research has been focusing on more recently. Next slide please, and that is that we sleep in cycles. We sleep in 4 to 5 cycles at night and each cycle is 2 hours long and this is key to why our residents are really falling because they are not getting these cycles of sleep. Ideal every night, people should sleep in four 2 hours cycles and each cycle has within them stages of Falls prevention 20 sleeps stage 1, 2, 3, and REM or stage IV. 1, 2, 3, REM, 1, 2,
3, REM and we wake up in the morning. Each of those stages has been identified scientifically as producing very specific results in the human body. Stage 1, stage 1 sleep is a transition from wake to sleep. Stage 1 generally lasts 5 to 15 minutes, brain waves begin to flatten, eyes begin to move more slowly, muscles begin to relax every once in a while we will have the sudden twitch or feeling of falling and we twitch awake and that literally is that the muscles have relaxed too quickly releasing too many minerals and enzymes into the surrounding area so we suddenly have a twitch, but we should be falling asleep within 5 to 15 minutes. Our vital signs begin to drop.
We begin to breathe more deeply and more slowly. Our core body temperature begins to drop, pulse and respirations begin to go slower. Stage 2, the brain wave activity is getting even flatter, the eyes are moving less, the muscle tonicity is beginning to relax, the muscle is not as tight, it is beginning to relax, peristaltic activity slows down, brain waves slows down, and ever so briefly we begin to do a computer save file trash of the events that have happened during the day. Our brain begins to look at the back 24-hour period and say “okay wait, I will be saving for ever, filing for short term need or trashing totally. Stage 3 sleep occurs at about 90 to 100 minutes into this cycle of sleep, so about 90 minutes to almost Falls prevention 21
2 hours into sleep, the most powerful deep physiological healing occurs. The greatest amount of healing occurs at stage 3 because the brain waves are almost flat, the muscles are completely flaccid and relaxed, the heart muscle is at its slowest, the pulse, respirations, core body temperature, blood pressure is at its flattest and lowest. When all of these is at its greatest point of relaxation, the greatest amount of healing occurs at this stage due to the greatest amount of white blood cell formation, T4 cancer fight cell formation, and red blood cells re-oxygenation, cellular molecular repair and regeneration occurs at stage 3 sleep and we found when we put our Actiwatches on our residents, fewer than 20% of our residents ever entered stage 3 sleep, they just did not enter this stage of sleep because we were interrupting them at 90 to 2 hour intervals.
Next slide please. If we allowed ourselves to continue to stay asleep for 2 hours ever so briefly, we would enter REM sleep.
Initially, early in the night, REM sleep only lasts for just a moment or two. As the night progresses each cycle we get deeper and deeper REM sleep. REM sleep is when we have a sudden burst of brain wave activity and eye movement and we begin to have and create long episodic story dream. They only may be 30 to 40 seconds in length at the early part at the evening, but later into the night, they can be 20 to 30 minutes in length and this period, this specific stage of sleep, this stage of sleep is Falls prevention 22 rapid eye movement sleep is where we see the deepest emotional, mental and psychological healing of the human body. These long episodic story dreams are created to alleviate us of fear, anger, stress, and sadness, and it also cements memories. This is one of the most powerful healing processes of the human body and it is mental-psychological healing. Next slide please. The next slide shows you the result of what we found with our residents. Our residents are only experiencing stage 1, 2, 1,
2, 1, 2, and a little bit of REM sleep at the end of the night and why is that because we are interrupting their sleep and every time you interrupt sleep, you have to start that cycle all over again so when we interrupt the sleep start again 1, 2, start again and so they never get the benefit of stage 3, stage
4 sleep. Next slide please. What we did is we learned how human beings fall asleep and wake up and the key, the physiological key to sleep and wake is light and darkness. If you will, next slide please. Light enters the human eye and that light wave travels down the human eye to the back of the eye where it is picked up by your nerve, the suprachiasmatic nerve, so that wave length from that light hits that nerve and that wave length travels down that nerve that light wave if you will, is changed into an electronic impulse and it travels down to the center of the brain and here is the key of our whole program. In the center of the brain is your pineal gland and Falls prevention 23 the pineal gland produces two hormones, the first hormone serotonin. Serotonin is produced with a light wave, the electrical impulses from that light wave hits the pineal gland.
The pineal gland gets a message, it is light outside and when it gets that message, it starts to produce a chemical, a hormone called serotonin and when serotonin is released into the bloodstream it explodes absolutely the brain wave activity.
Brain waves begin to increase eye wave, eye movement increases.
Serotonin crosses over into the heart muscle and the heart muscle starts to contract more rapidly so we see an increase in the pulse, blood pressure. Serotonin enters the lungs and we breathe more rapidly. Serotonin enters every single organ in the body and it literally wakes up that organ and it produces more activity within that organ, so all endocrine gland secretions increase in the presence of serotonin. Serotonin increases peristaltic activity, it enters our mouth and we become more hungry. It enters every single muscle and ligament and we can actually move more rapidly. We can constrict our muscles more tightly. Serotonin in essence is the wake-up hormone and it is produced because light travels to the back of the eyes, convert it into an electrical impulse that travels to the pineal gland and serotonin is made, manufactured, and distributed to the body. The inverse of that happens when it is dark, the darkness enters the eyeball, the lack of white Falls prevention 24 stimulation or the lack of a white wave or darkness travels down to the pineal gland and the pineal gland gets a reading, it is dark outside, stop making serotonin, start making another chemical melatonin and melatonin does just the opposite of what serotonin does. If you will, the next slide please.
Melatonin is a powerful chemical. Melatonin is made in the presence of darkness. When melatonin is released into the bloodstream, brainwave activity stops, eyes stop moving, we begin to breathe deeply, our heart slows down, our brainwaves become less and less active and our muscles begin to become totally relaxed to the point INAUDIBLE 50:31 we cannot move, we are paralyzed when we get enough melatonin, and in essence, we fall asleep.
The next slide relatively tells you serotonin and I have already mentioned that.
And so, what we have discovered is that light is the key to waking people up, darkness is the key to putting people to sleep but only about 8-10 years ago, Rensselaer Polytechnic Institute in New York identified something else. They identified that is not just how bright the light is, it is actually the color of light that puts us to sleep and wakes us up. Falls prevention 25
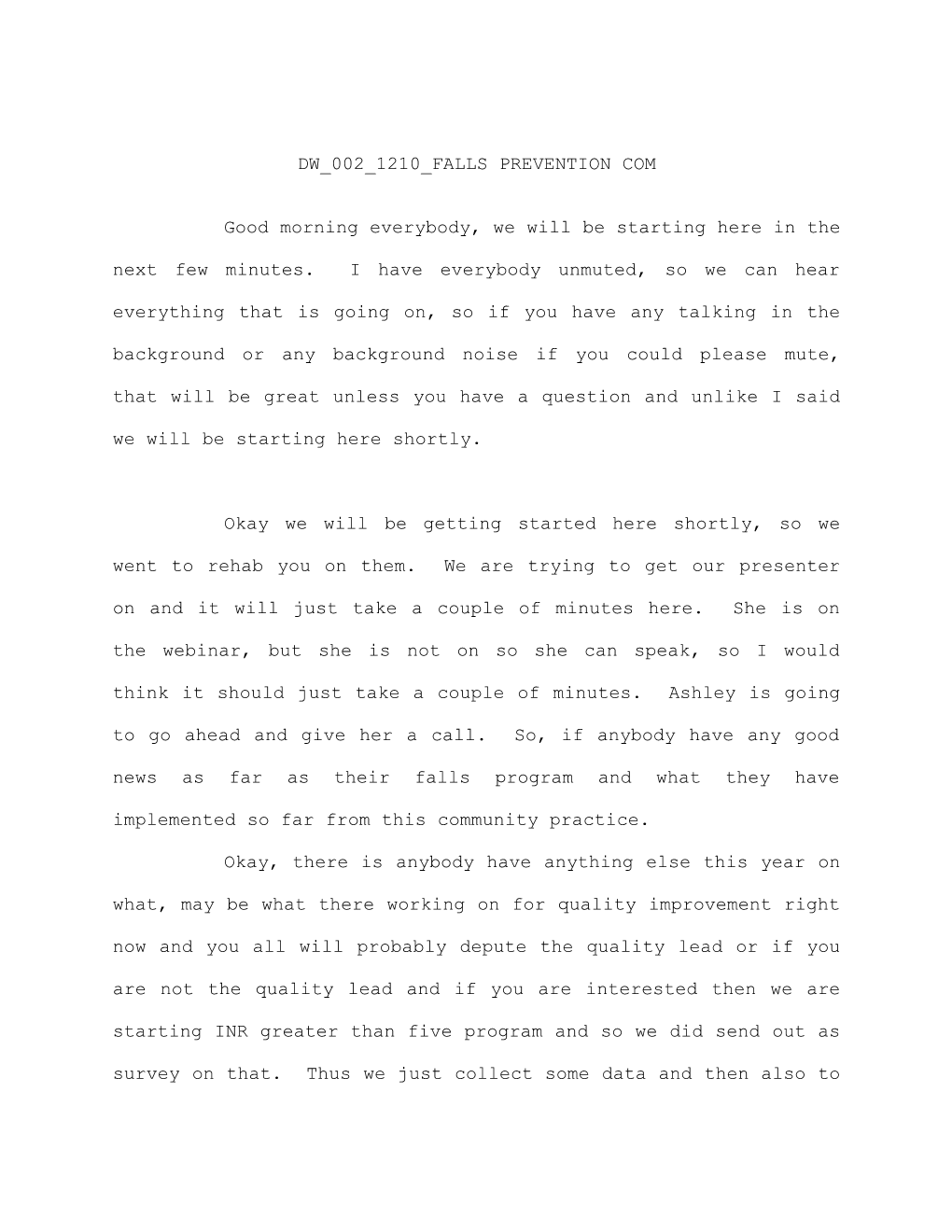
If all of you would take a look at this picture; this is a picture of an office and the office is filled with lot of light blue light. My question to everybody would be the following.
If you had to more quickly, work swiftly and have a high workout. So you got to work very quickly, very swiftly, come up with a lot of creative ideas and have a high work output. Where is that more likely to occur in this office or in the following office. We are eager to work quicker, swifter, faster, or have a higher output. This office has a lot of red, yellow, orange light.
The next pictures are of restaurant. This restaurant has a lot of light blue light, so blue, purple, white light. My question again. Where are you going to eat quickly, expect to be served quickly, eat fast and get out soon this restaurant or this restaurant, you expect to eat quick, eat fast, be served quickly and get out fast more often than not and in most situations people would say I would work faster in that light white blue office, not in that yellow, orange office. I would eat way more quickly in that light blue light than in this light. In this light, I would eat slower, I would take my time and I would leave later. Falls prevention 26
What we have discovered is that the color of the light speeds up internal activities and it actually speeds up the production of melatonin and serotonin. Violet, blue, green light is all very rapid, quick wavelength and those rapid quick wavelengths actually produce more serotonin. The pineal glands will be more awaked by producing more serotonin in blue light, but the other end of the spectrum red, orange, yellow light is a very slow wavelength, and the slow wavelength will go to the pineal gland and it will stop making serotonin and it will start making melatonin. That is in essence how we sleep. Not only the brightness of the light but the color of the light, so the rapid blue swift blue-purple wavelength keeps us awake because it makes more serotonin and the red-orange yellow light is a slow wavelength. It hits the pineal gland, it stops making serotonin and it starts making more melatonin.
Simply reinforces what I have just explained that is not the brightness of the light so much but the color of the light.
And so, research absolutely supports blue light in the morning wakes us up by producing more serotonin. Stop having blue light at night at least within two hours of sleep because that blue light is going to stop the manufacturing of melatonin. Falls prevention 27
Again, science support orange, yellow, red light should be used at night because it allows melatonin to be made.0
So taking all of this information, we looked at the lighting source in our building and this is really for your information side.
What light in our own personal environment as well as our nursing home are producing more red light, candle light, fire places are all red light. All the incandescent light bulb are more red light, but if you go down that color spectrum, you will see that cellphone, HGTV screens are moving into the blue light spectrum. Computer, laptops, halogen lights and LED lights are all blue-purple spectrum lights and we should be using those during the early morning and afternoon hours.
The other thing that we learned about sleep is the amount of activity we engage in during the day will also affect melatonin and serotonin level, and many of us already are fully aware of this.
We are like rechargeable to battery. If any of you have cellphones, I am sure you do. If you have any electronic tooth brushes, if you read the manufacturing directions on it, it will actually say to extend the life of the battery, slowly exhaust or allow the battery to run done prior to recharging and human Falls prevention 28 being is just like this. If we sit around all day and are less active, we actually get less sleep at night. We do not sleep as deeply, we do not produce as much melatonin, we do not produce as much serotonin during the day, and so when we sit around and are less active during the day, we have less deep sleep at night. The more specifically active we are during the day, we are literally burning down the battery and the batter gets a better recharge at night by running down the battery. That was something else we identified. When we put the active watch on the residents, we were measuring their activity level during the day and we were horrified to see how low their activity levels were which then contributed to shallow sleep at night.
We also looked at the scientific research into where if they are in bed for a long period of time at night is that great. Would have been beneficial for them, would be 9 hours or 10 or 11 or
12 hours in bed might be better.
And once again, our scientific research and investigation identified that no. When people consistently stay in bed for greater than nine hours every single night, here are the horrific outcomes of that on the human body and this really was the state of our residents. We found that anywhere from 35 to
40% of our residents were in bed for more than 10 hours every Falls prevention 29 single night. I mean, I know who I am speaking to and the people who are listening or people who put residents to bed or assist in getting residents to bed at 6:30 to 7:30 at night and then the residents who are not getting up until 6:30 to 7:30 morning and that is a consistent routine of how we run our nursing home that residents are in bed for greater than 10 hours at night, and the result is dehydration, progressive cardiac deconditioning, postural hypotension, reduced lung capacity.
These are all the outcomes that scientists have found from people who are in bed for more than 10 hours at night. And at another time I would let you go through and read specifically what it is. And when I look at all of these horrific outcomes from being in bed at night, I realize that these were the very items that I have spent my career putting on resident care plan.
This is in essence a resident care plan. Reduced cardiac output, skin breakdown, constipation, etc. etc.
And so we began our program. Once we learned about sleep, a science of sleep, how we sleep and how we awake and the detrimental effects on sleep, we have really been said how are we going to set up this program to prevent the disturbances of sleep and the first thing we had to identify is what disturbs sleep the most. Falls prevention 30
We looked at and wanted to do research specifically into identify what are the environmental, clinical and operational factors, what is in place in these residents lives that their sleep is being so disturbed. Environmentally, we knew light is on all night and the most incorrect color of light is on. We also know the environmental factors of noise. We have noisy staff at night, people are making rounds, opening doors, closing doors, opening drawers, closing drawers, moving equipment in and out of residents rooms, so noise. We looked at the clinical factors. The internal factors of residents’ sleep being disturbed at night. We know that internally that we were looking at medications that we were giving these residents at night. We looked at operational situations that were going on at night, again what time were shift changes occurring. What we actually doing at night in the environment that was resulting in the operations of how we ran nursing home that was disturbing all residents at night. And then we flipped and looked it during the day. How come our residents were not more awake during the day. How could we have residents say that they enjoyed more wakeful hours, environmentally why were not they enjoying wakeful hours. Well, the first environment that we identified was it was dark in our nursing homes. Are we were not opening window covering, we were not getting residents outdoors in the outside lights of the sun that would benefit Falls prevention 31 them the greatest. So, most of our residents’ environment was indoors INAUDIBLE 01:01:49 with window coverings still on. We looked at clinical factors. How come we were getting these residents more physically active during the day and how could we do that and then operationally.
How come we could not get our residents more physically active during the day. The greatest benefit to our program was actually something we discovered and that was the Harvard sleep study. Remember our program started in 2011 and it was a three- year grant, and in 2011, we essentially said okay, we are going to stop disturbing sleep at night and keep them awake during the day and the number one benefit to us was that Harvard University
Medical Center had just completed a very intense five-year study and they published their findings in 2011 and what they identified was they wanted to do research and did research to discover what were the greatest disturbances to human sleep.
And here was the result of their study. The top 10 disturbances to human sleep at night is:
1. Noise.
2. Light.
3. Sleep environment meaning your matters, your sleep surface,
your bedding, the temperature of the room; what are you
sleeping in, pajamas, nightgown and then the aroma or smells Falls prevention 32
around you. So sleep environment was the third greatest
disturbance to sleep.
4. Naps. More naps, naps lasting more than 30 minutes would
reduce deep quality sleep at night and so that has been well
documented that you do not make up for lack of sleep the night
before by taking a nap the next day. What you actually do is
start a vicious cycle of napping shallow during the day and
napping shallow at night.
5. The fifth greatest disturbance of sleep at night is
medication.
6. Continent sneeze
7. Pain.
8. Positioning the need to reposition.
9. Inactivity during the day resulting in a lack of good quality
sleep at night.
10. Then what do we eat and drink, that should exactly say,
diet/fluids during the day contributed to sleep disturbance at
night.
I am going to just stop you for a moment, Jennifer and ask because I am about to go into and cover the actual program and how we address each of these 10 disturbances in our program. I just want to stop now and ask. Are there any questions at this point regarding anything I said thus far. Is it clear on just, Falls prevention 33
I know I went through this ever so quickly. Is it clear to everyone the very simple way human beings fall asleep and awake.
And any questions up to this point of my presentation.
Does anybody need any clarification. Yeah but, what if. Could if there are not any questions, I will move on and actually explain again ever so briefly how we address each of these disturbances because the way we ran our program, how we rolled it out, what we said, this is huge. We were overwhelmed at the beginning of our program and we said how are we going to start the program and the way we are going to start it is to look at each of these individual items one by one, but we are going to start with the greatest disturbance noise and once we get noise under control then we will move to light and once we get light under control, then we will move to sleep. So we did a very specific one by one move down this program and here is what we did.
This webinar was supposed to end at 12:30, but if you have time to listen to rest of it, I think even though she is speaking about how this happens and she does this in the nursing home, it still applies to our hospitalization exactly, and I want everybody to know that if you do have to get off because I do want to respect your time. I am going to continue learning her Falls prevention 34 speak and this is being recorded. We will put it on our website and I also will share her slide on HEN-HUB but I think hopefully before people have to kind of get off, can we guess around three takeaways that you have received from her speaking today; things that maybe made you think a little bit more about how we are doing our patient care and how that is affecting all. Pick it up three takeaways before she continues. Thank you yes. I know we have all learned something. Did anybody know that there were four cycles of sleep at night or about the circadian rhythm and when melatonin kicks in and when it stops and maybe when we think about our patients that are in the hospital for a reason, it is not immobility but we are having them lay in the bed all day basically horizontal and not having them get up and be upright or letting them sleep the whole time even though they really do not need that. Can I have some better response for you to excite, make lot more people will listen to this after it is recorded so I will let you continue on, so again. Thank you.
Sure. And this is what I am doing now is just sharing the application of what I have explained in the last hour. We took the etiology of sleep and we took this Harvard Sleep Study and that is how we rolled out our program looking at the etiology of sleep and the disturbance of sleep. Falls prevention 35
Each slide now addresses the top 10 disturbances of sleep and it addresses it through interventions to prevent that disturbance from occurring. What I have really done is created 10 slides on the implementation of our program and this first slide is the implementation of the intervention to prevent noise and it shows. The first thing we did was we audited sound levels to identify what was causing the noise. We identified where the noise was, the times of day the noise was and whose specifically and which departments were causing the noise. So we did if you will a noise assessment of our environment. Once we identify the times of the day where and who was causing the noise, we can then move on to things that what will we do to eliminate the noise. What we did is we eliminated all overhead paging, audible call lights and we eliminated all personal alarms. None of our residents anymore have personal alarms attached on or near them. We still have maintained exit alarms into unsafe areas. We reduced noisy times. We reduced noisy area. We identified loud speaking staff.
And all I am doing now is rolling through the implementation of the program. This shows you specifically how we addressed the elimination of all personal alarms. Falls prevention 36
The elimination of all personal alarms and in fact in the state of Minnesota it is now at a directive from the
Department of Health Surveyors are working with us and becoming an alarm free nursing home state and just a kind of the side note, by the way, CMS had been kept abreast of all the findings of our program. So we shared with CMS and we shared with our
State Department of Health Surveyors. All of these findings from our fall program and our sleep program. And the last year
July 28, 2015, CMS has issued in draft from the following and it was sent to all of our State Surveyors your State Surveyors
INAUDIBLE 1:10:54 and I would just like to read this opening paragraph and this is the summary paragraph of a draft from CMS to all Department of Health State Surveyors, some nursing homes used various types of physician change alarms as of full prevention strategy or in response to a resident fall, evidence does not support that alarm use effectively prevents falls.
Alarms may also have adverse consequences for residents and the facility environments, the Centers for Medicare and Medicaid has revised the guidance to surveyors in appendix PP under F tag
321, 222 and 323 to discuss the appropriate role of physician change alarm and resident cares. I would encourage everyone to get a copy this draft because in the United States today we are moving towards the elimination of residents using and wearing personal alarms. Falls prevention 37
Next slide please.
And so for the next of my slides what I have done is I have summarized the implementation of intervention to stop that disturbance. Here is the lighting and shows you step by step what we did with lighting. The implementation of timers and dimmers that automatically have lights going on and off and we changed the color of lights. In dining room, we have white blue light. We used way more light blue florescent LED lights during the day and all of our lights in the buildings are turned off at night with the use of use just wall sconces or night lights that are red or blue and then our staff at night all wear hug lights and again I had encouraged all of you to just you Google hug lights and you will that this is a malleable, bendable tube of light that worn around the caregivers neck and it is a directional light and the light can also be adapted and changed, so we do not have overhead lights we actually have individual lights being worn by our staff.
Next slide please.
Sleep surfaces, we make certain that all of our sleep surfaces are pressure relieving mattresses that with a key.
Next slide please. Falls prevention 38
You will see that NPUAP National Pressure Ulcer Advisory Panel in 2014 now has a specific recommendation for the type of mattresses our residents should sleep on in order to reduce and eliminate and prevent any skin breakdown due to pressure, and so
I would encourage anyone listening to get that documentation because that’s what we use for our sleep program, we are able to reduce the amount of times we turned and repositioned our residents because they were now on supportive sleep surfaces that had a reduction in pressure points and so with pressure redistribution relieving mattresses, you do not have to turn in reposition as often.
Next slide please.
Naps: It shows exactly what we did with nap, we reduced the frequency of naps, we encouraged one nap in the middle of the day generally between the hours of 2 and 4 o’ clock not to be more than 30 to 40 minutes in length.
We then addressed medication that shows exactly what we did with medication, we did not awaken the residents to take a medication at night once they were sleep, we did not disturb their sleep, we really worked with our pharmacist and physicians to have medications that were only given in order to be given during waking hours, we looked at side-effects of meds to see which medications would cause residents to be jittery or fidgety or Falls prevention 39 what medications had side-effects what would say the blood pressure would increase or the pulse would increase and so those medications would not be given before sleep at night. We really looked at side-effects as far as they caused drowsiness or does it drops their blood pressure. Why are we giving those meds at
9 a.m. in the morning, 8 a.m. in the morning, those medications with that type of side-effects would be better given just before bed at night.
Next slide please.
We looked the pain as the contributing factor to the disturbance of sleep at night and we looked it what is causing the pain and could we address this through environmental better sleep surfaces, could they bring their own pillows. We provided many different types of pillows to enhance more comfortable sleep, feather pillows, foam pillows, crunchy foam, side pillows, back pillows to sleep. Pillows that would enhance the resident’s sleep, full body pillows, different types of sheeting that would encourage resident to be more comfortable. We ask residents are you more comfortable on cotton sheets, flannel, satin and then provided that because all of that enhance their comfort level of sleep and reduce their pain. We asked residents would you rather sleep in pajamas, what kind of pajamas, and nightgowns yeah, what kind of nightgowns and so by offering residents more Falls prevention 40 comfort at night sleeping they have less pain. We also looked at what about pain medication being given just before sleep that would be slow time relief to enhance they are sleep at night by being and less pain.
Next slide please.
Continents and repositioning were huge for us and I really cannot say much about that in such a time-constraint area opportunity, except to say that we really looked at allowing our residents to sleep for greater periods of time at night.
Next slide please.
We looked as because we are using the act2 watches we really looked at fluid intake and looking at providing opportunity for residents to have more fluid in the morning hours and taper that fluid throughout the day as many of us to know and we are all well aware for our own personal hygiene needs that if we were to drink a lot of fluids before bedtime we would need to get up in the middle of the night and so one of the things we noticed with our residents as we are pushing h.s. snacks and fluids, which was counter to a good night of sleep. We are giving medications in bulk at night four or five six meds before sleep that resulted in them having to take more fluid to swallow those pills, maybe we could have offer those pills in liquid form Falls prevention 41 thereby reducing the fluid at night and essence our incontinence program was really a hydration control program offering more fluids earlier in the day and tapering the fluid intake throughout the day to a reduction and cessation of fluid intake after the evening meal and that really shows you on the slide exactly how we did that. We also encouraged and used overnight incontinent products, the products that have polymer in the middle of the layers of the incontinent product that would allow the urine to be whisked to be way or pulled away from the skin surface, so now they have less fluid intake after the evening meal resulting an less fluid output during the night and what fluid also they do put out is whisked away from the body due to the polymer in the incontinent product.
Next slide please.
We really took a lot of time going through and looking at our act2 watches and seeing when a resident is sleeping through the night can we push them from two-hour disturbance to 3-4, 4-6, and 6-8.
Next slide please.
We could not even do this program without the knowledge and assistance of Nancy Bergstrom, I would say clearly that I would not do this program without downloading and reading intensely Falls prevention 42 and following her citation there, The Journal of American
Geriatric Society, Turning for Ulcer Reduction. She really did intense research into sleep surfaces and the ability to allow residents to sleep longer and longer periods of sleep at night and reducing their skin breakdown and so it was through her research and then the next citation there is Jerry Lundgren, her article she published in the Wound Care Advisor and her Turning
Program Hindering a good night’s sleep. Jerry Lundgren worked with us from day one to really prevent skin breakdown and allowing residents to sleep more consistently and for more hours without interruption at night without increasing skin breakdown and incontinence.
and allowing residents to sleep more consistently and for more hours without interruption at night without increasing skin breakdown and incontinence. So, for anyone doing or considering this program I really must say that Nancy Bergstrom and Jerry Lundgren were invaluable to the program and their research was.
The next couple of slides really are just a summary of
Nancy Bergstrom’s work on repositioning or reducing the need to reposition residents and allow you to read those slides on your own. Falls prevention 43
Again, this is a summation of Nancy Bergstrom’s work and Jerry Lundgren’s work.
And then we looked at lastly diet and foods. We looked at the type of food that resident ate to enhance sleep and to enhance wakefulness. We looked at the amounts of fluid that they took in.
We looked at the fluids that actually enhance and give better energizing wakeup in the morning. We looked at breakfast foods that actually wake the human body up and get us going. We changed that on menus and encouraged residents to eat more of these breakfast items. We looked at snacks in the afternoon.
And then we looked at what we called our snooze foods; those foods that have been identified of enhancing a better deeper night of sleep and so these are the foods that we encouraged after both at and after bedtime. These became our evening meal menu foods and bedtime snacks.
We knew that activity was the other part of our program that we need to enhance, in order to get better sleep at night, to reduce falls, to reduce depressions, agitation and to increase a better lifestyle for residents. We really focused on Falls prevention 44 increasing the opportunity for residents to be more active during the day.
Our sharing and caring program is the program that we set up to enhance more activity after the evening meal keeping residents more active at night after the evening meal so that they would go to bed later and go to bed having less time in bed so that they were looking at the 9, 10, 12 hours in bed at night. We knew that that was not healthy for the residents, so we wanted them to go to bed later. How do we get them to go to bed later, by offering more active program that would engage them and be of interest to them after the evening meals and offer more activities during the day that would again enhance them to stay wake during the day, and I just sort of number of falls in the next couple of slides reflects more of the activity program that residence enjoy doing during the day.
And then to just wrap up, at the every end of our program there will really, in the last couple of years, great strides made the in the science of aroma therapy. That is what we are working on right now. We are looking at aroma therapy to enhance wakefulness during the day and sleepiness at night.
Science has well documented that the essential oils that are FCC accredited and so we use those essential oils in our program Falls prevention 45 right now. I am really bringing you up-to-date with our current program and that is that we using essential oils to enhance wakefulness during the day, specifically the oils of citrus and mint during the day and that at night lavender and camomile, and we are using these because we are aware of the fact that brainwave activity can be both stimulated by scent or relaxed by scent and so that scent is yet another tool in our toolbox of enhancing wakefulness during the day and sleepiness at night.
And so to summarize, to really wrap up and summarize; did the implementation of the sleep prevention program reduce falls in the nursing home. I mean that really was the key. We knew that we had to get to the root causes of the disturbance of sleep at night, why will residents being disturbed at night. We knew that, from the get go if we did not get leadership on board; if we did not get, when I say leadership, I do not just mean the administrators and supervisors in my facilities, I mean the CEOs of the companies, but even more importantly I mean the leadership as far as our surveyors, CMS, quality improvement organizations, ombudsmen, we were educating everyone on these programs, so that all of our programs were enhanced by the leadership and the greatest leadership that we really consulted were our residents and their families, to keep them informed and to get them on board behind this program, so the leadership of Falls prevention 46 the staffs, residents, families, physicians, surveyors, and government. We really started with the easiest root and the easiest root was noise INAUDIBLE 01:25:36. Those were the easy part of the program. As we advanced down that part of our sleep study, we realized that more difficult programs were those last ones, continence, positioning, pain, and medication.
So, did we actually reduce falls through our sleep program?
That was the key question here. I am just sharing with you two of my facilities and I have got dozens and dozens of these slides. In 2012, one year into our sleep program, here is an example of the 65-bed facility, one of our facilities, 65-bed facility on average they were experiencing 17 falls a month.
One year later into the sleep program, 2013, they were experiencing nine falls a month. Essentially, a 50 percent cut in falls by the implementation of the sleep program.
The next one shows you a 102-bed facility. One year into the sleep program on average they were experiencing 25 falls a month. Two years into the sleep program, they are experiencing 13 falls a month. Again, we are seeing what the implementation of our program that allows residents to sleep Falls prevention 47 through the night. We essentially have reduced falls yet again in all of our facilities. And the only thing I would like to point out on the last slide is the very last line; I know there is a lot of information there. The very last line shows you that on average, when we started our sleep program or actogram watches identified that 99 percent or our residents were being disturbed every two hours. They were not necessarily being changed or repositioned, although most were. Many of that disturbance was because of the activities that we were doing by distributing linen, incontinent products etc, etc., but we were able to identify through our acto watches that 99 percent of our residents sleep with disturbed every two hours. One year into the program, we reduced that by 58 percent of our residents’ sleep was disturb every two hours and by 2013, it was 7 percent.
That is a significant obvious enhancement in the overall wellbeing and health of our residents and that is my conclusion of my program. I want to thank Jenniffer for the opportunity to present the program of Empira and I want to thank the Iowa
Healthcare Collaboration for the opportunity to share the work of Empira.
Thanks again Jenniffer.
Thank you so much Sue Ann. Falls prevention 48
Everybody enjoy your day and again we can discuss this on Hen Hub or via email, but I think that Sue Ann did a fabulous job for us bringing the sleep pattern to us and even though she is talking about nursing home we can implement a lot of these thinks into our hospital and just loot at what is going on. So, once again have a wonderful day and I will have this recording by the end of the week on our website and then also I will put the slides on Hen Hub.
Have a very great day.
Thank you bye-bye