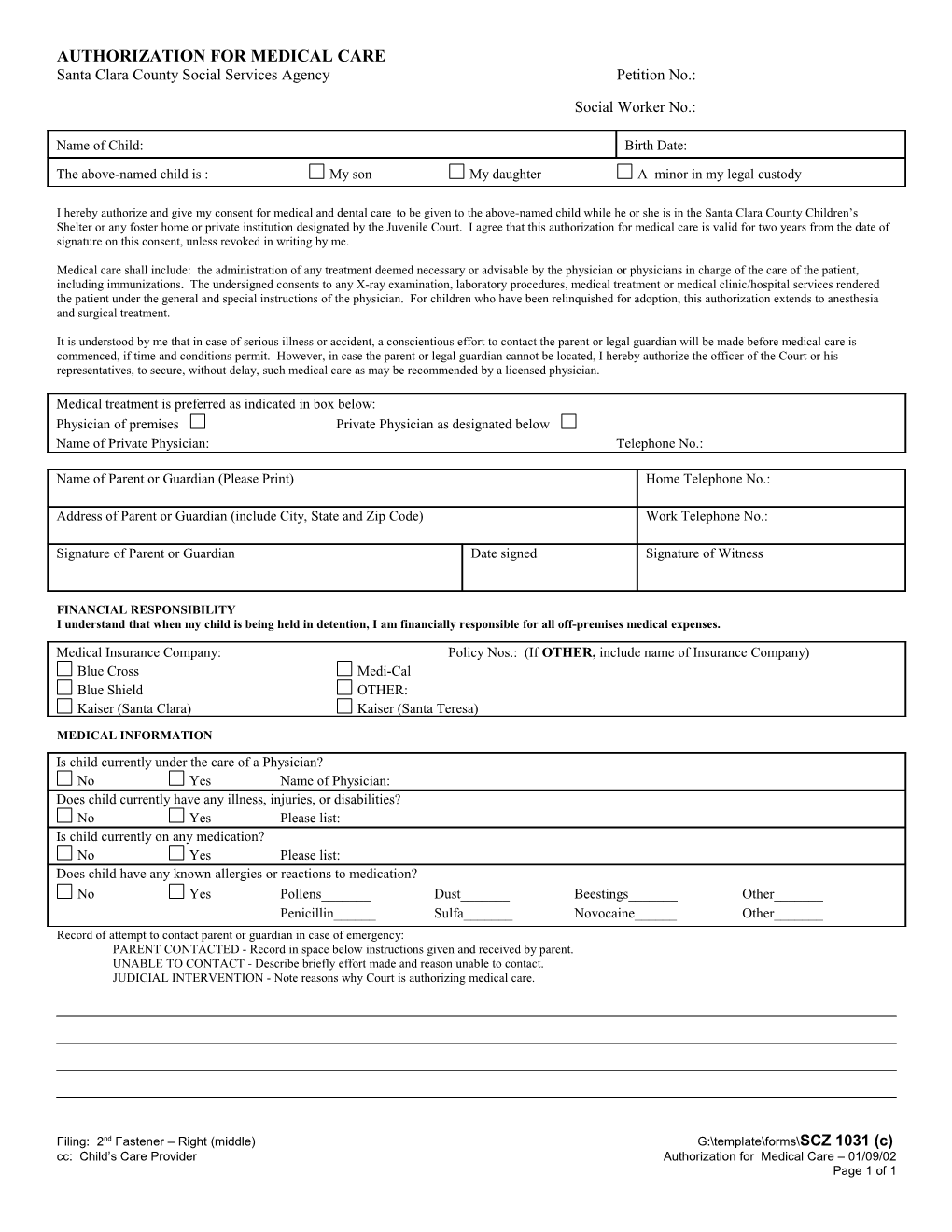
AUTHORIZATION FOR MEDICAL CARE Santa Clara County Social Services Agency Petition No.:
Social Worker No.:
Name of Child: Birth Date:
The above-named child is : My son My daughter A minor in my legal custody
I hereby authorize and give my consent for medical and dental care to be given to the above-named child while he or she is in the Santa Clara County Children’s Shelter or any foster home or private institution designated by the Juvenile Court. I agree that this authorization for medical care is valid for two years from the date of signature on this consent, unless revoked in writing by me.
Medical care shall include: the administration of any treatment deemed necessary or advisable by the physician or physicians in charge of the care of the patient, including immunizations. The undersigned consents to any X-ray examination, laboratory procedures, medical treatment or medical clinic/hospital services rendered the patient under the general and special instructions of the physician. For children who have been relinquished for adoption, this authorization extends to anesthesia and surgical treatment.
It is understood by me that in case of serious illness or accident, a conscientious effort to contact the parent or legal guardian will be made before medical care is commenced, if time and conditions permit. However, in case the parent or legal guardian cannot be located, I hereby authorize the officer of the Court or his representatives, to secure, without delay, such medical care as may be recommended by a licensed physician.
Medical treatment is preferred as indicated in box below: Physician of premises Private Physician as designated below Name of Private Physician: Telephone No.:
Name of Parent or Guardian (Please Print) Home Telephone No.:
Address of Parent or Guardian (include City, State and Zip Code) Work Telephone No.:
Signature of Parent or Guardian Date signed Signature of Witness
FINANCIAL RESPONSIBILITY I understand that when my child is being held in detention, I am financially responsible for all off-premises medical expenses.
Medical Insurance Company: Policy Nos.: (If OTHER, include name of Insurance Company) Blue Cross Medi-Cal Blue Shield OTHER: Kaiser (Santa Clara) Kaiser (Santa Teresa)
MEDICAL INFORMATION Is child currently under the care of a Physician? No Yes Name of Physician: Does child currently have any illness, injuries, or disabilities? No Yes Please list: Is child currently on any medication? No Yes Please list: Does child have any known allergies or reactions to medication? No Yes Pollens______Dust______Beestings______Other______Penicillin______Sulfa______Novocaine______Other______Record of attempt to contact parent or guardian in case of emergency: PARENT CONTACTED - Record in space below instructions given and received by parent. UNABLE TO CONTACT - Describe briefly effort made and reason unable to contact. JUDICIAL INTERVENTION - Note reasons why Court is authorizing medical care.
Filing: 2nd Fastener – Right (middle) G:\template\forms\SCZ 1031 (c) cc: Child’s Care Provider Authorization for Medical Care – 01/09/02 Page 1 of 1 DATE: NAME:
Filing: 2nd Fastener – Right (middle) G:\template\forms\SCZ 1031 (c) cc: Child’s Care Provider Authorization for Medical Care – 01/09/02 Page 2 of 1