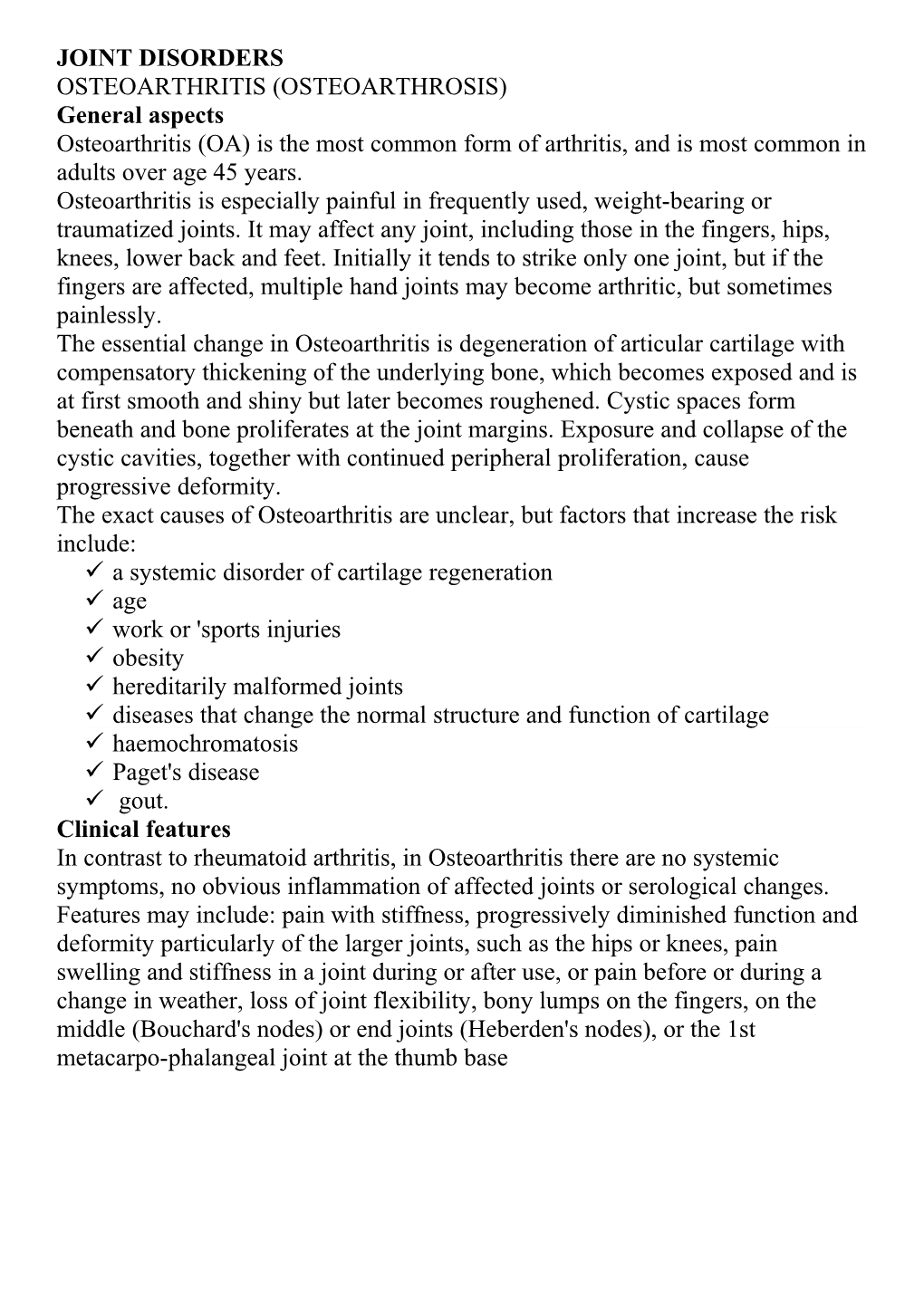
JOINT DISORDERS OSTEOARTHRITIS (OSTEOARTHROSIS) General aspects Osteoarthritis (OA) is the most common form of arthritis, and is most common in adults over age 45 years. Osteoarthritis is especially painful in frequently used, weight-bearing or traumatized joints. It may affect any joint, including those in the fingers, hips, knees, lower back and feet. Initially it tends to strike only one joint, but if the fingers are affected, multiple hand joints may become arthritic, but sometimes painlessly. The essential change in Osteoarthritis is degeneration of articular cartilage with compensatory thickening of the underlying bone, which becomes exposed and is at first smooth and shiny but later becomes roughened. Cystic spaces form beneath and bone proliferates at the joint margins. Exposure and collapse of the cystic cavities, together with continued peripheral proliferation, cause progressive deformity. The exact causes of Osteoarthritis are unclear, but factors that increase the risk include: a systemic disorder of cartilage regeneration age work or 'sports injuries obesity hereditarily malformed joints diseases that change the normal structure and function of cartilage haemochromatosis Paget's disease gout. Clinical features In contrast to rheumatoid arthritis, in Osteoarthritis there are no systemic symptoms, no obvious inflammation of affected joints or serological changes. Features may include: pain with stiffness, progressively diminished function and deformity particularly of the larger joints, such as the hips or knees, pain swelling and stiffness in a joint during or after use, or pain before or during a change in weather, loss of joint flexibility, bony lumps on the fingers, on the middle (Bouchard's nodes) or end joints (Heberden's nodes), or the 1st metacarpo-phalangeal joint at the thumb base Fig. 1: - Comparison of osteoarthritis and rheumatoid arthritis
General management The diagnosis is usually on clinical grounds, supported by imaging. The characteristic radiographic features include: 1. narrowing of the joint space 2. marginal osteophyte formation (lipping) 3. subchondral bone sclerosis 4. bone 'cysts' (rounded areas of radiolucency just beneath the joint surface) 5. deformity. Physical methods of treatment include: 1) regular exercise - to help maintain joint mobility 2) weight control - to minimize stress on joints 3) appropriate footwear if there is arthritis in weight-bearing joints or back 4) a walking stick to ease the load on a damaged joint 5) heat application to ease pain, relax tense, painful muscles and increase the regional flow of blood 6) cold application for occasional flare-ups. Medical methods of treatment include: topical pain relievers (trolamine salicylate, counterirritant medications such as methyl salicylate, menthol and camphor, or capsaicin), which may relieve pain in joints close to the skin surface, such as fingers, knees and elbows. non-steroidal anti-inflammatory drugs (NSAIDs) or licofelone, or COX-2 inhibitors such as celecoxib. Glucosamine as a food supplement, which is said to provide moderate pain relief comparable to that from NSAIDs. Antidepressants which, independent of their antidepressant properties can help lessen chronic pain. Intra-articular injections with a corticosteroid or hyaluronate which can give pain relief for a time. Surgical methods of treatment include: joint replacement surgery the most important surgical treatment for arthritis. The damaged joint is removed and replaced with a plastic or metal prosthesis. The hip joint is most commonly replaced, but implants are available for knee, shoulder, elbow, finger or ankle joints. Completely normal function is usually restored Arthroscopy can be used to remove loose fragments of bone or cartilage that may cause pain or cause mechanical symptoms such as 'locking'. However, there is no significant improvement in pain relief or function 2 years afterwards. Surgery can reposition bones to help correct deformities and can permanently fuse bones in a joint to improve stability and reduce pain. Dental aspects Age and immobility may influence access to dental care. Infections of prosthetic joints are usually due to non-oral organisms such as staphylococci and only exceptionally rarely to oral bacteria. Even where viridans streptococci have been found in infected joints, they could have come from non-oral sources, or simply have come from a bacteraemia associated with chewing. The same arguments as for endocarditis as to the risk: benefit of antimicrobial prophylaxis. Antibiotic prophylaxis is therefore not indicated for dental surgery on most patients with bone pins, plates and screws or with total joint replacements. However, antibiotic prophylaxis, 1-1.5 h before dental treatment likely to initiate a bacteraemia may be considered where dental at-risk procedures are to be carried out: in patients who have recent new joints (within 2 years) in haemophiliacs where the joint has previously been infected where the patient is immunocompromised, such as those with diabetes or rheumatoid disease. Antibiotic regimens are: Prophylactic antibiotics in patients with prosthetic joints: based on AAOS/ADA guidelines Comments Dental at-risk procedure Tooth removal Oral or periodontal surgery or raising mucogingival flaps for any other purpose (including implants) Subgingiva! procedures including probing, scaling, root planning, subgingival fibre placement or any form of periodontal surgery Intraligamentary injections Reimplantation of avulsed teeth Endodontic manipulation beyond the root apex Orthodontic banding Joint at risk Joint placed within previous 2 years Joint with history of previous infection Joint in patient with haemophilia Joint in patient with type 1 diabetes Joint in patient with rheumatoid arthritis Joint in patient on immunosuppressive therapy Antibiotic prophylaxis Cefalexin 2 g OR regimens Clindamycin 600 mg OR Azithromycin 500 mg OR Clarithromycin 500 mg OR Amoxicillin 2 g *Modified from 1997 American Association of Orthopedic Surgeons & American Dental Association cefradine 1 g orally or intravenously is a further choice. Although the evidence may be questionable, medicolegal and other considerations suggest that one should act on the side of caution and fully inform and discuss with the patient, take medical advice in any case of doubt give antibiotic prophylaxis for at-risk procedures in patients at high risk for infection. Dental management may be complicated by a bleeding tendency if the patient is anticoagulated or takes high doses of aspirin. Osteoarthritis affects the temporomandibular joints in some elderly patients but typically painlessly. Those with Osteoarthritis of other joints also do not appear to have significantly more involvement of the temporomandibular joints than controls. The radiographic severity of TMJ Osteoarthritis does not correlate with symptoms and it is frequently only a post-mortem finding. Since TMJ Osteoarthritis is rarely clinically significant, patients should not be made unnecessarily anxious. A syndrome of dry mouth and Osteoarthritis has been described (sialoadenitis, Osteoarthritis, xerostomia - SOX) but needs confirmation. Celecoxib may cause taste disturbance: rofecoxib may cause oral ulceration. RHEUMATOID ARTHRITIS Rheumatoid arthritis (RA) affects about 2% of the population in the West, Women are affected approximately three times as frequently as men, typically between the ages of 30 and 40 years. Rheumatoid arthritis is a multi-system immunologically mediated disease, but predominantly causes chronic symmetrical polyarthritis mainly of small joints.
Features of rheumatoid arthritis RA is associated with HLA-DR4. An autoantibody (rheumatoid factor, RF) is an IgM antibody directed against abnormal IgG formed in the joint tissues. It is postulated that immune complex (antigen-antibody complex) formation may then lead to the activation of complement, inflammation and synovial damage. Clinical features The onset of RA is often insidious, with increasing stiffness of the hands or feet, worse in the morning. In the acute stage there is aching, swelling, redness, tenderness and limitation of movement of small joints of the wrists, hands and feet, which are typically affected first. There is sometimes also fever and malaise. The metacarpophalangeal and interphalangeal joints typically become spindle-shaped as a result of joint swelling with muscle wasting on either side. Ulnar deviation of the fingers may develop later. Eventually, also, the wrists, elbows, ankles and knees may be involved and the patients becomes disabled. Other common manifestations are tenosynovitis or subcutaneous nodules. The cervical spine is involved in 30% and there may be atlanto-axial subluxation. Clinically apparent effects on other systems are less common, but can include: Sjogren's syndrome normochromic anaemia (anaemia of chronic disease) sensory neuropathy pleural and pericardial disease eye disease; episcleritis and scleritis. General management The diagnosis of RA is made if at least four of the features shown in Table above are present. Rheumatoid factor (RF), present in about 70%, is usually IgM and a sensitive marker of RA but is not specific. In so-called seronegative cases the RF may be IgG, and therefore not detected by the routine agglutination tests (Latex and SCAT), which detect only IgM RF. RIA and ELISA detect any class of RF. Antinuclear antibodies are also often found but are usually in low titre. Rheumatoid arthritis: features and complications Joints Arthritis Tenosynovitis Laxity of ligaments Subluxation Spinal nerve root compression Non-specific features Fever Malaise Fatigue Dermal, oral and para-oral Palmar erythema Various rashes Subcutaneous nodules Sjogren's syndrome Temporomandibular arthritis Oral drug lesions Muscular Weakness Wasting Osseous Osteoporosis Ocular Sjogren's syndrome Episcleritis, scleritis or scleromalacia Cardiovascular Pericarditis Myocarditis Valvulitis Vasculitis Haematological Anaemia Leucopenia Thrombocytopenia Respiratory Pleurisy and pleural effusion Nodules in lung Fibrosis Bronchiolitis Neurological Various neuropathies Carpal tunnel syndrome Glove and stocking anaesthesia Benign trigeminal neuropathy Renal Various nephropathies Amyloidosis Hepatic Abnormal liver function Table 22.5 Laboratory findings in rheumatoid arthritis
Typical findings Test
Normocytic anaemia Full blood count Mild leucocytosis (or leucopenia) Mild thrombocytopenia Raised Erythrocyte sedimentation rate Hypergammaglobulinaemia Protein electrophoresis Positive usually Rheumatoid factor - latex agglutination Positive in 20-60% Antinuclear antibodies The ESR and C reactive protein are typically high. Radiographic features are soft-tissue swelling, juxta-articular osteoporosis and widening of the joint space due to accumulation of fluid in the early stages. Later there is narrowing of the joint spaces, cyst-like spaces in the bone, and subluxation. Ultimately there may be severe bone destruction and deformity, but ankylosis does not follow. Factors associated with a poor prognosis include: positive RF extra-articular disease HLA DR4 early erosions severe disability at presentation. The main aspects of treatment are: rest in acute phases, but between these episodes maintenance of mobility of affected joints drugs, which include: symptom-modifying drugs such as NSAIDs, or COX- 2 inhibitors if NSAIDS cannot be tolerated, biological-response modifiers. Anakinra - a direct and selective blocker of interleukin-1 (IL-1) receptor, and Etanercept and infliximab, which act against tumour necrosis factor (TNF) alpha, may be given for severe active disease, but can cause severe toxic effects. Aprosorba column a blood-filtering technique used weekly to remove autoantibodies is sometimes available. disease-modifying antirheumatic drugs (DMARDs), which may relieve painful, swollen joints and slow joint damage: mainly sulfasalazine, but others such as gold, penicillamine, minocycline or antimalarials may also be used. Methotrexate in low dose may be helpful for more severe arthritis. Corticosteroids, azathioprine, ciclosporin, cyclophos-phamide and leflunomide are reserved for severe arthritis, in view of their adverse effects. Hyaluronic acid viscosupple-mentation products such as Hyaluronan may improve joint mobility. joint replacement occasionally needed. Dental aspects In some patients dislocation of the atlanto-axial joint or fracture of the odontoid peg can readily follow sudden jerking extension of the neck, as a result of weakness of the ligaments. Disastrous accidents of this sort have been known to follow adjustment of the head-rest of older types of dental chair, or sudden extension of the neck during the induction of general anaesthesia. Patients with joint prostheses because of rheumatoid disease may possibly require antibiotic cover before surgical procedures since those with rheumatoid disease are regarded as mildly immunocompromised. A few patients are treated with corticosteroids. Some treatments induce neutropenia, thrombocytopenia or a bleeding tendency. Patients may also have severely restricted manual dexterity and consequent difficulty maintaining adequate oral hygiene. Toothbrushes may need specially adapted handles, e.g. by adding a plastic or rubber ball to help the patient grip the brush, or an electric brush may solve this problem. Sjogren's syndrome is the main oral complication. There is a predilection of RA for small joints, including the TMJ, but though there may be limitation of opening or stiffness these are often painless. Radiographic changes are common in the TMJ and consist of erosions, flattening of the joint surfaces and marginal proliferation. Even when the disease is severe, pain from the TMJ appears to trouble only a minority. Occasionally an anterior open bite or even sleep apnoea may result.
Rheumatoid arthritis of the tempromandibular joint The drugs used in rheumatoid arthritis can be a cause of oral side effects such as ulcers and lichenoid reactions. NSAIDs, gold and low-dose methotrexate may cause ulceration.
Oral side effects of the drugs in rheumatoid arthritis GOUT In gout, uric acid crystals are deposited in joints, and phagocytosis by polymorphs, and result in release of lysosomal enzymes - causing acute inflammation. Primary gout is an inborn error of metabolism that causes raised serum levels of uric acid (hyperuricaemia). Hyperuricaemia is common, but usually symptomless. Gout mainly affects adult men, in whom food rich in purines (such as fish roe), or an alcoholic 'binge' especially with beer, can precipitate an attack in those with the underlying metabolic disorder. Ethanol favours conversion of pyruvate to lactate, which impairs renal excretion of urate. Some forms are inherited in an autosomal dominant manner, while in others there is evidence of polygenic inheritance. Lesch-Nyhan syndrome, deficiency of hypoxanthine-guanine phosphoribosyltransferase (HGPRT), is a rare cause of gout. Secondary gout is usually caused by drug treatment or radiotherapy of myeloproliferative diseases releasing large amounts of purines into the blood. Gout of either type is aggravated or can be caused by diuretics (thiazides and loop diuretics), which impair renal excretion of uric acid. Women are not significantly at risk from gout until after the menopause. Clinical features Gouty tophi are masses of urate crystals which, in joints, interfere mechanically with function and also destroy bone and cartilage to cause a severe, deforming arthritis. An acute attack of gout causes sudden and intensely severe joint pain, usually in the big toe, associated with fever, leucocytosis and raised serum uric acid levels. Many gouty patients are obese, and there is a high incidence of hyperlipidaemia, hypertension, diabetes mellitus and atherosclerosis. Chronic tophaceous gout is often associated with renal disease (gouty nephropa- thy), which, unless treated, leads to fatal renal failure in up to 25%. Extra- articular tophi typically form in the helix of the ear as conspicuous, almost white, hard, subcutaneous nodules. General management Blood chemistry shows raised uric acid levels. Secondary gout should be investigated for the underlying disorder. Colchicine and indometacin relieve an acute attack but can cause severe side effects. Anti-inflammatory analgesics are therefore used. Aspirin, which interferes with uricosuric agents, should not be given. Allopurinol reduces the frequency of acute gouty attacks. It inhibits xanthine oxidase and the conversion of xanthine to uric acid and also inhibits total synthesis of purines In severe cases, uricosuric agents, such as probenecid or sulfinpyrazone, can be used to increase uric acid excretion. In a few patients (<1%) with diminished HGPRT activity, allopurinol does not operate and the drug can, rarely, cause xanthine renal stones to form. Activation of 6-mercaptopurine and azathioprine, both purine antimetabolites, depends on HGPRT. Consequently, the therapeutic effects of these drugs are not attained in patients with Lesch-Nyhan syndrome. Dental aspects Hypertension, ischaemic heart disease, cerebrovascular disease, diabetes mellitus and renal disease may affect dental management. Aspirin is contraindicated as it interferes with uricosuric drugs. The incidence of rashes with ampicillin, but not other penicillin allergies, is greater in patients on allopurinol. Drugs used for the treatment of gout, particularly allopurinol, can occasionally cause oral ulceration. Gout affects the temporomandibular joint only rarely. Lesch-Nyhan syndrome is a rare inborn error of metabolism, in which hyperuricaemia is associated with learning disability, choreoathetosis and compulsive self-mutilation. The lips are chewed and self-inflicted injuries especially to the face and head, despite the pain it obviously causes, are typical. Calcium pyrophosphate deposition disease (CPDD) involves deposition of calcium pyrophosphate in and around joints in conditions of high plasma calcium, low phosphate or low magnesium. It appears similarly to gout and is treated by correction of the metabolic disturbance, and NSAIDs. ANKYLOSING SPONDYLITIS General aspects Ankylosing spondylitis is a seronegative spondyloarthropathy (predominantly affects the spine), seen mainly in young males. The inflammation involves the insertions of ligaments and tendons and is followed by ossification, forming bony bridges that fuse adjacent vertebral bodies or other joints. Ankylosing spondylitis is partly genetically determined; the family history may be positive and over 90% are HLA-B27. Clinical features The onset is usually insidious, with low-back pain (spondylitis) and stiffness followed by worsening pain and tenderness in the sacro-iliac region due to sacro- iliitis. Hip joints may also be involved. Over the course of years the back becomes fixed, usually in extreme flexion, and chest expansion becomes limited and respiration impaired. About 25% develop eye lesions (uveitis or iridocyclitis), About 10% develop cardiac disease (aortic incompetence or conduction defects). General management The ESR is raised, HLA-B27 is often positive and there is a mild anaemia, but no other significant laboratory findings and no autoantibodies. Radiography shows progressive squaring-off of vertebrae (which become rectangular), intervertebral ossification ('bamboo spine'), calcification of tendon/ligament insertions and obliteration of the sacro-iliac joints. Treatment consists of: physiotherapy and exercises, anti-inflammatory analgesics to control pain and allow the back to be kept as mobile as possible. Phenylbutazone or indometacin may be used. Radiotherapy to the spine occasionally given, but carries the risk of leukaemia. Dental aspects General anaesthesia can be hazardous because of severely restricted opening of the mouth, impaired respiratory exchange associated with severe spinal deformity, or cardiac disease (aortic insufficiency). Ankylosing spondylitis can affect the temporomandibular joints in about 10%, especially those over 40 years of age with widespread disease, but symptoms are usually mild. Antibiotic prophylaxis may be indicated for at-risk dental procedures if there is aortic incompetence.