U R Medway Only Clinicians:- Band TI 5 6 7 Triage:LBP/Non LBP Non triage FR OR LTC LX TX CX LL UL Initial Self Referral Form – Adult Musculoskeletal Physiotherapy PhysioPhysiotherapyFor Official Use Only
Patient Details: GP Details: Title: Mr/Mrs/Ms/Miss Name: First Name: GP Practice Address: Surname:
Address:
Information: Postcode: Do you require an interpreter? Yes/No Contact Tel. No: (Home) (Work) If yes, which language? (Mobile) NHS Number if known: Can we leave a message on any of these numbers? Date of referral: Occupation:
Date of Birth:
Please give a brief description as to why you would like a Physiotherapy assessment:
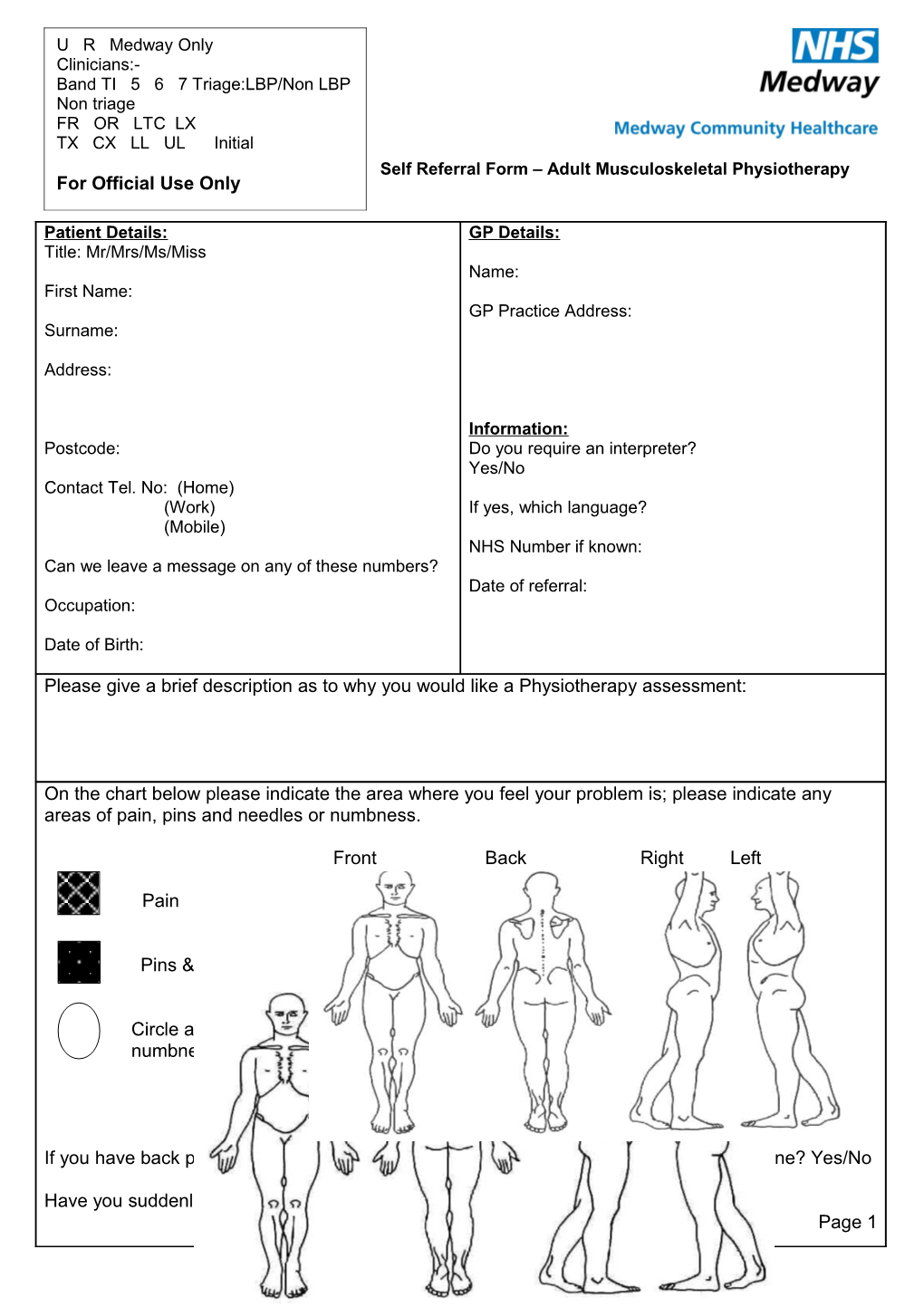
On the chart below please indicate the area where you feel your problem is; please indicate any areas of pain, pins and needles or numbness.
Front Back Right Left
Pain
Pins & Needles
Circle area for numbness
If you have back pain with leg pain have you had any difficulties passing or controlling urine? Yes/No
Have you suddenly lost weight without trying? Yes / No Page 1 If any of the following is relevant to your pain please speak to your GP first.
Trauma i.e. fall from height, road accident Constant increasing pain Previous cancer history Drug usage – HIV Sudden unplanned weight loss Steroid use Generally unwell Difficulties with urine/bowel problems
Please list any medication you are taking or attach copy of medication list
Symptom History: Please tick as appropriate.
When did this problem start? Less than 2 weeks / 2-8 weeks / 8-12 weeks / more than 12 weeks?
Is the problem:
New □ Ongoing □ Flare up of an old problem □
Getting better □ Getting worse □ Staying the same □
Does it wake you at night? Yes □ No □
Are you off work/unable to care for a dependent Yes □ No □ because of this problem?
Is the problem stopping you from doing things? Yes □ No □
Please specify:
Pain
If you have pain, please indicate how severe your pain is on this scale of 0 - 10
0 1 2 3 4 5 6 7 8 9 10
No pain at all Mild Moderate Severe Worst pain possible Page 2 Medical History - Please tick as appropriate.
Have you consulted your GP about this problem? Yes □ No □
Have you tried anything to help with your problem? Yes □ No □ (e.g. pain killers, exercise, other treatment)
Please specify:
Have you had Physiotherapy for the same problem in the last 6 months? Yes □ No □
If so, where did you have your Physiotherapy?
Are you suffering from any of the following:
MRSA □ C.diff □ diarrhoea & vomiting □ scabies □
Impetigo □ undiagnosed skin rash □
IMPORTANT. Adult Physiotherapy is for patients aged 16 and above, patients with problems affecting muscle joints etc, including back pain, neck pain and shoulder pain.
Take , send or fax your completed referral to the Physiotherapy Department at: Adult Musculoskeletal Physiotherapy Department Medway Maritime Hospital Windmill Road Gillingham Kent ME7 5NY
Contact Tel: 01634 833959 Fax: 01634 402877 Email: [email protected]
A physiotherapist will look at your form and prioritise based on the information you have supplied. We will contact you regarding an appointment in due course.
Page 3