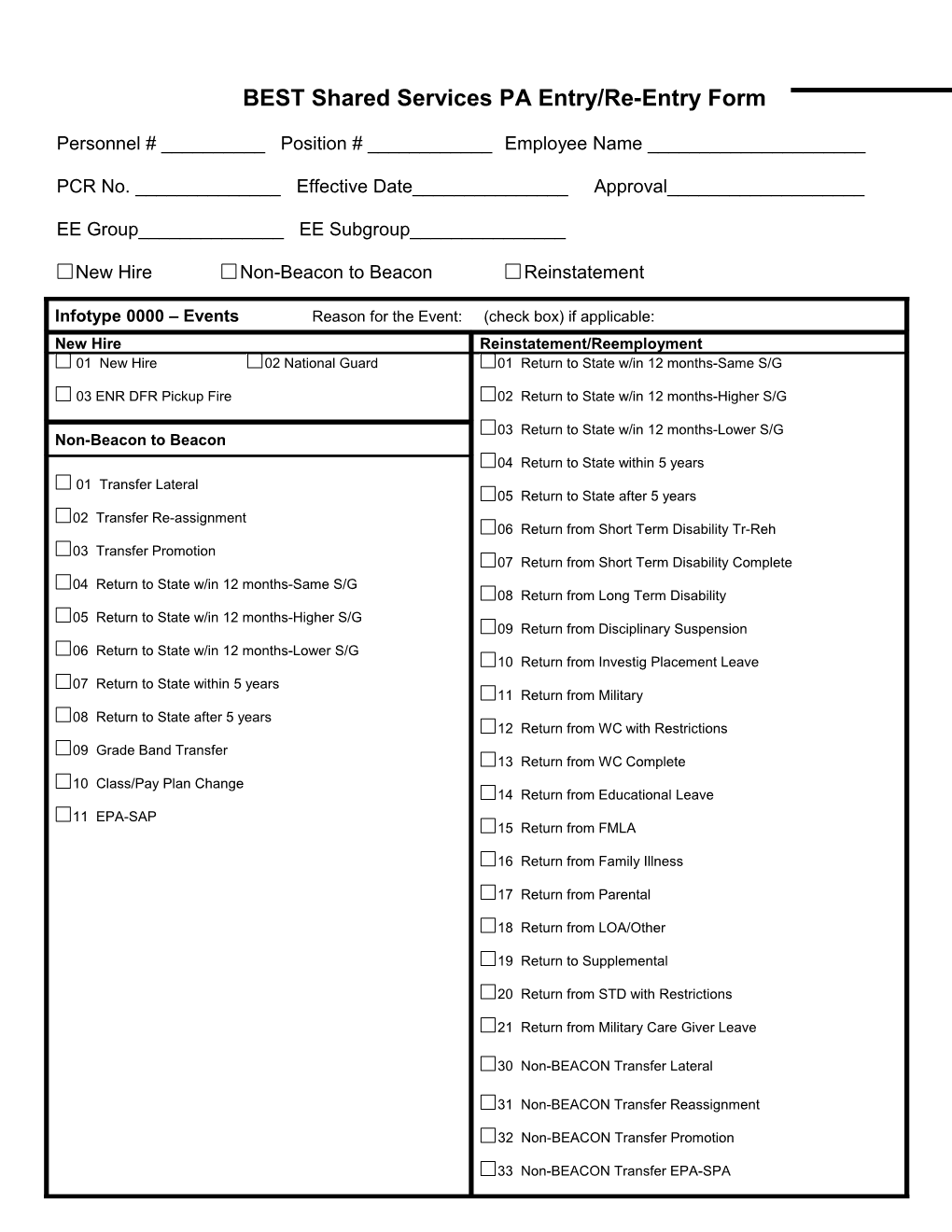
BEST Shared Services PA Entry/Re-Entry Form
Personnel # ______Position # ______Employee Name ______
PCR No. ______Effective Date______Approval______
EE Group______EE Subgroup______
New Hire Non-Beacon to Beacon Reinstatement
Infotype 0000 – Events Reason for the Event: (check box) if applicable: New Hire Reinstatement/Reemployment 01 New Hire 02 National Guard 01 Return to State w/in 12 months-Same S/G
03 ENR DFR Pickup Fire 02 Return to State w/in 12 months-Higher S/G
03 Return to State w/in 12 months-Lower S/G Non-Beacon to Beacon 04 Return to State within 5 years 01 Transfer Lateral 05 Return to State after 5 years 02 Transfer Re-assignment 06 Return from Short Term Disability Tr-Reh 03 Transfer Promotion 07 Return from Short Term Disability Complete 04 Return to State w/in 12 months-Same S/G 08 Return from Long Term Disability 05 Return to State w/in 12 months-Higher S/G 09 Return from Disciplinary Suspension 06 Return to State w/in 12 months-Lower S/G 10 Return from Investig Placement Leave 07 Return to State within 5 years 11 Return from Military 08 Return to State after 5 years 12 Return from WC with Restrictions 09 Grade Band Transfer 13 Return from WC Complete 10 Class/Pay Plan Change 14 Return from Educational Leave 11 EPA-SAP 15 Return from FMLA
16 Return from Family Illness
17 Return from Parental
18 Return from LOA/Other
19 Return to Supplemental
20 Return from STD with Restrictions
21 Return from Military Care Giver Leave
30 Non-BEACON Transfer Lateral
31 Non-BEACON Transfer Reassignment
32 Non-BEACON Transfer Promotion
33 Non-BEACON Transfer EPA-SPA BEST Shared Services PA Entry/Re-Entry Form
34 Non-BEACON Transfer Class Pay Plan Change Infotype 0002 – Personal Data
Last Name: ______First Name: ______Middle Name: ______Social Security Number: ______- ______- ______Date of Birth: ______/______/______Gender: Male Female Marital Status: Single Married Widow Divorced Separated
Infotype 0001 – Create Organizational Assignment Subarea: (Defaults from Position) Refer to Job Aid Bus. Area: (Defaults from Position) Refer to Job Aid
Func. Area, Cost Center #, Fund: (Defaults from FI table)
Contract Type: (Please check box) if applicable RE Ret Ex from Lmt
M1 MedCare EE Elig M4 MedCare SP Elig R0 Ret Non NC Gov
M2 MedCare CH Elig M5 MedCare EE&SP RS Ret Sub to Lmt
M3 MedCare EE&CH S1 SHP Full EE Cost
Infotype 0006 – Addresses (Permanent)
Address line 1: ______City: ______County: ______State: ______Zip: ______Telephone # : (______) ______- ______BEST Shared Services PA Entry/Re-Entry Form Infotype 0006 – Addresses (Emergency Contact) (Employee can modify in ESS)
C/O: ______Address line 1: ______City: ______County: ______State: ______Zip: ______Telephone # : (______) ______- ______
IT0007 – Planned Working Time
Work Schedule Rule: Part-Time Employee Weekly Work Hours: _____
Infotype 0008 – Basic Pay Reason: New Hire Non-Beacon to Beacon Reinstatement Annual Salary: ______Hourly Rate: ______(Temps Only)
Infotype 41 – Date Specifications (Dates Default)
Date type 01 – Original Hire Date: ______Date type 02 – Agency Hire Date ______
Date type 04 – Judicial Anniversary Date ______Date type 07 – Lottery Anniversary Date ______